

Abstract
Background Research data regarding the correlation between elevated oxidised low-density lipoprotein (oxLDL) cholesterol concentrations and unfavourable clinical outcomes in individuals experiencing minor acute ischaemic cerebrovascular events or transient ischaemic attack (TIA) with presumed atherosclerotic aetiology are still limited.
Methods This investigation incorporated a cohort of 5814 participants derived from the Intensive Statin and Antiplatelet Therapy for Acute High-Risk Intracranial or Extracranial Atherosclerosis clinical trial. The core laboratory conducted blinded measurements of baseline plasma oxLDL concentrations. Multivariable Cox regression analyses were employed to assess the correlations between oxLDL levels and adverse clinical events. The principal endpoint for efficacy assessment was defined as the occurrence of stroke within a 90-day follow-up period. Additional secondary endpoints encompassed composite vascular events during the same observation window. The main safety endpoint assessed was the occurrence of bleeding events of moderate to severe intensity.
Results The final analytical cohort comprised 5814 patients included in the final analysis. The mean age was 63.7±9.6 years, and 36.0% were female. The average concentration of circulating oxLDL was 36.62 µg/dL. Elevated oxLDL concentrations demonstrated a potential correlation with heightened stroke risk (T3 vs T1: HR 1.39, 95% CI 1.04 to 1.85), ischaemic stroke (T3 vs T1: HR 1.31, 95% CI 0.98 to 1.76) and composite vascular events (T3 vs T1: HR 1.36, 95% CI 1.02 to 1.81) within 90 days. An increased concentration of oxLDL demonstrated a significant association with elevated susceptibility to moderate and severe haemorrhagic events (T3 vs T1: HR 3.61, 95% CI 1.26 to 10.34) within 90 days.
Conclusion Increased concentrations of oxLDL demonstrated an independent correlation with both stroke recurrence and the occurrence of moderate-to-severe haemorrhagic events in individuals presenting with acute minor ischaemic stroke or TIA at elevated risk, accompanied by intracranial or extracranial atherosclerotic lesions.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Oxidised low-density lipoprotein cholesterol (oxLDL) plays a pivotal role in the pathogenesis of atherosclerosis. Elevated levels of oxLDL independently predicted recurrent stroke in patients with mild stroke or transient ischaemic attack (TIA).
WHAT THIS STUDY ADDS
An increased concentration of oxLDL demonstrated an independent correlation with both stroke recurrence and the occurrence of moderate to severe haemorrhagic events in individuals presenting with acute mild ischaemic cerebrovascular accidents or high-risk TIAs accompanied by intracranial or extracranial atherosclerotic lesions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
OxLDL may prove to be a valuable diagnostic tool in identifying patients at an elevated risk for stroke recurrence or bleeding.
Introduction
Oxidised low-density lipoprotein (oxLDL) is formed by oxidative modification of LDL in response to a number of complex factors in the body.1 OxLDL has been demonstrated to cause damage to vascular endothelial cells, promote the aggregation of mononuclear macrophages at the lesion site, stimulate the proliferation and migration of vascular smooth muscle cells, facilitate the phagocytosis of large amounts of lipids into foam cells, and ultimately result in the formation of atherosclerotic plaques.2 3 These plaques can subsequently lead to a range of cardiovascular and cerebrovascular events.4–6
Several previous studies have suggested the clinical significance of oxLDL in cardiovascular and cerebrovascular diseases. A high level of oxLDL is one of the most effective biomarkers of adverse cardiac events.7 Serum oxLDL level predicted 10-year progression of subclinical carotid atherosclerosis.8 OxLDL can be used as a screening marker for unstable carotid plaques in patients with ischaemic stroke.9 Elevated level of oxLDL independently predicted cerebrovascular event recurrence among individuals presenting with minor ischaemic stroke or transient ischaemic attack (TIA).6 9 Current reports indicated a positive correlation between high NIHSS scores and elevated oxLDL levels in patients with acute ischaemic stroke. OxLDL was significantly associated with a poor 1-year prognosis and 1-year mortality in stroke subtypes of large-artery atherosclerosis and small artery occlusion.10 However, the role of oxLDL in predicting adverse outcomes in patients with cerebral ischaemic attack due to atherosclerosis remains uncertain.
Extensive research has established that increased levels of oxLDL play a pivotal role in the pathogenesis of atherosclerotic disease. Individuals presenting with TIA of high-risk profile exhibit significant susceptibility to subsequent cerebrovascular events. This investigation used clinical data from the INSPIRES trial (Intensive Statin and Antiplatelet Therapy for Acute High-Risk Intracranial or Extracranial Atherosclerosis) to examine the prognostic value of circulating oxLDL concentrations in predicting unfavourable clinical outcomes.
Methods
Study design and participant characteristics
The participants were from INSPIRES study. The rationale, design and methodology of this clinical trial have been previously described in detail.11 12 This research used a 2×2 factorial experimental framework incorporating randomisation, double-blind procedures and placebo-controlled conditions. The participant cohort comprised individuals aged 35–80 years presenting with either minor stroke (NIHSS score ≤5) or TIA with elevated risk (ABCD2 score ≥4), evaluated within 24–72 hours post-onset. Additionally, patients experiencing ischaemic stroke with NIHSS scores of 4–5 within 24 hours of symptom onset were included in the study population. Additionally, eligible patients are required to fulfil one or more of the specified conditions: (1) demonstration of ≥50% luminal narrowing in either intracranial or extracranial major arteries, which is considered causative for both the cerebral infarction and clinical manifestations, as verified through carotid ultrasound examination or vascular imaging techniques or (2) the presence of simultaneous acute infarcts presumably originating from large-artery atherosclerotic disease, encompassing cases with unstable non-obstructive plaques, as evidenced by neuroimaging modalities such as cranial CT or MRI. Between 17 September 2018 and 15 October 2022. The study was carried out at a network of 222 medical centres distributed throughout China. A cohort of 11 431 individuals diagnosed with either ischaemic stroke or TIA underwent eligibility assessment, resulting in the enrolment of 6100 participants. A cumulative number of 5814 blood serum specimens were obtained.
Ethical approval procedures, study registration protocols and participant consent acquisition
The INSPIRES trial was approved by the ethics committee of Beijing Tiantan Hospital (No.KY2017-065-02) and all other participating sites. Before enrollment, patients or their representatives provided written informed consent. This trail was registered at ClinicalTrials.gov (NCT03635749).
Outcome assessment
The main effectiveness endpoint was defined as the incidence of any cerebrovascular accident (either ischaemic or haemorrhagic subtype) during the 90-day follow-up period. Additional outcome measures encompassed a combined endpoint of vascular events, which consisted of cerebrovascular accidents, acute myocardial infarction (MI) or mortality attributable to vascular causes, all evaluated within the same 90-day time frame. The main safety endpoint was defined as the occurrence of moderate to severe haemorrhagic events, as classified by the bleeding criteria established in the Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries study.13 These outcome measures were operationally defined in accordance with the standardised criteria implemented in the preceding INSPIRES randomised controlled trial.11 All local investigators received standardised training to ensure the accuracy and consistency of their assessments. All documented outcomes pertaining to both efficacy and safety were validated by an independent committee responsible for clinical event adjudication. The members of this committee were blinded to the allocation of study groups.
Determination of oxLDL concentrations
Venous blood specimens were obtained from participants who had undergone fasting, with collection occurring within a time frame of 24±12 hours post randomisation. The serum components were isolated at respective clinical sites and promptly cryopreserved at a temperature of −80°C. These processed specimens were subsequently transferred under cryogenic conditions using dry ice from multiple collection centres to the central laboratory at Beijing Tiantan Hospital for comprehensive processing and analytical procedures. The level of oxLDL in serum was quantified by using a monoclonal antibody−4E6-based14 ELISA kit (Xi‘an GoldMag Nanobiotech Co., Ltd. China). The experimental procedures were executed in adherence to the manufacturer’s guidelines at the central clinical laboratory facility of Beijing Tiantan Hospital. The experiment operators were unaware of the clinical information pertaining to the samples.
The demographic profile, behavioural patterns and clinical features
Demographic information, encompassing variables such as age and sex, along with clinical background details including previous medical conditions, tobacco use patterns and pharmaceutical treatment records, were obtained through structured survey instruments. The patient’s medical history includes the following: hypertensive, diabetes, dyslipidaemia, ischaemic stroke, TIA and MI. On hospital admission, qualified nursing staff conducted measurements of both blood pressure (BP) and body mass index (BMI) following standardised protocols established through the INSPIRES initiative.
Statistical analysis
Categorical variables are expressed as frequencies and percentages. Continuous variables with skewed distributions are expressed as median and IQR spacing. The study participants were stratified into three distinct cohorts based on the tertile distribution of oxLDL concentrations. Statistical comparisons for continuous variables were performed using the non-parametric Wilcoxon or Kruskal-Wallis tests, while categorical variable analyses were conducted through the application of the χ2 test.
The association between oxLDL and unfavourable clinical events was analysed through Cox proportional hazards regression analysis. The first tertile served as the baseline comparison category in this investigation. In order to ascertain the most accurate results, variables were included in the adjustment if they were associated with oxLDL or if they were traditional predictors of recurrent stroke. Both unadjusted and adjusted HRs were computed, along with their corresponding 95% CIs.
The interaction between oxLDL and randomised antiplatelet, statin therapy and lipid-lowering before events was studied using crude and multivariate Cox proportional hazards models. The patients were divided into two groups based on their treatment with clopidogrel and aspirin respectively. For each group, the incidence of adverse outcomes was evaluated in relation to the level of oxLDL using both univariate and multivariate Cox proportional hazard models during the 90-day follow-up period. Statistical significance was defined as a two-tailed p value below the threshold of 0.05. The data analysis was conducted using SAS statistical package, V.9.4 (SAS Institute) for all computational procedures.
Results
The initial demographic and clinical profiles of the participants
A total of 6100 patients were enrolled in the INSPIRES study, 5814 (95.31%) patients provided blood samples, and oxLDL values were detected in all blood samples which were included in the final analysis. A flow chart of this study is shown in figure 1. The mean age was 63.7±9.6 years, and 36.0% were female. The median concentration of circulating oxLDL was measured at 36.62 µg/dL, with an IQR spanning from 18.53 to 54.71 µg/dL. The enrolled population was divided into three groups, designated as oxLDL T1 (≤30.59 µg/dL), oxLDL T2 (30.59–42.65 µg/dL) and oxLDL T3 (<42.65 µg/dL), based on the tertiles of oxLDL levels. In comparison to patients with lower levels of oxLDL, patients with higher levels of oxLDL exhibited a higher proportion of women, a higher BMI, higher systolic and diastolic BP, and a higher proportion of a known history of diabetes mellitus, hypertension and dyslipidaemia. Conversely, a lower proportion of these patients had a history of ischaemic stroke. The baseline levels of LDL, high-density lipoprotein (HDL), triglyceride (TG), cholesterol (CHO), apolipoprotein A1 (APOA1) and apolipoprotein B (APOB) increased with an increase in the oxLDL grade (table 1).

Flow chart of the study. INSPIRES, Intensive Statin and Antiplatelet Therapy for High-risk Intracranial or Extracranial Atherosclerosis; oxLDL, oxidised low-density lipoprotein.
Baseline characteristics of patients according to oxLDL level
During the follow-up period, all patients received lipid-lowering therapy. There was no statistically significant difference in the proportion of patients receiving antihypertensive therapy, CEA therapy and stent implantation therapy between patients with different oxLDL level grades (online supplemental table 1).
Supplementary data
OxLDL levels and adverse outcomes
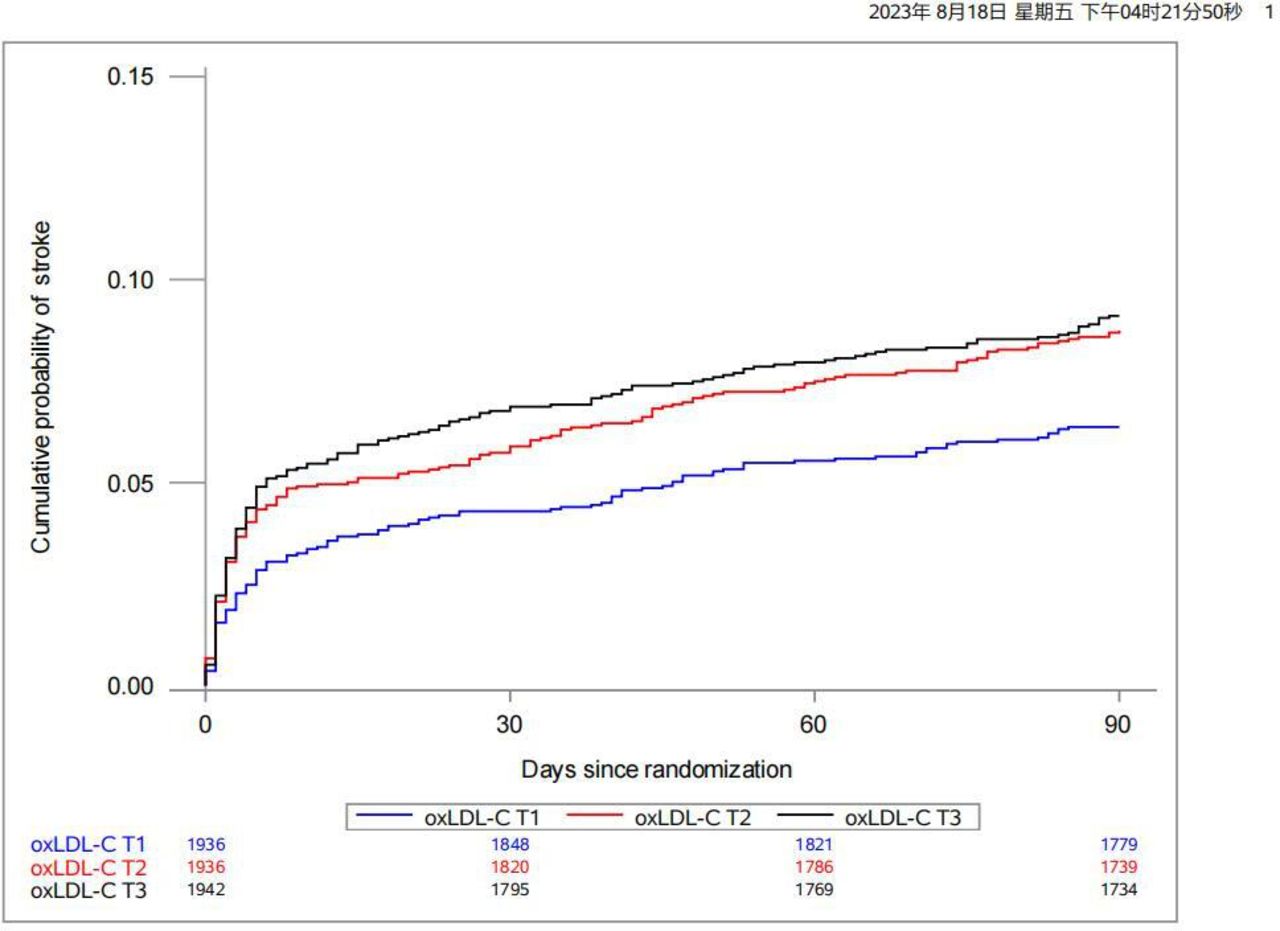
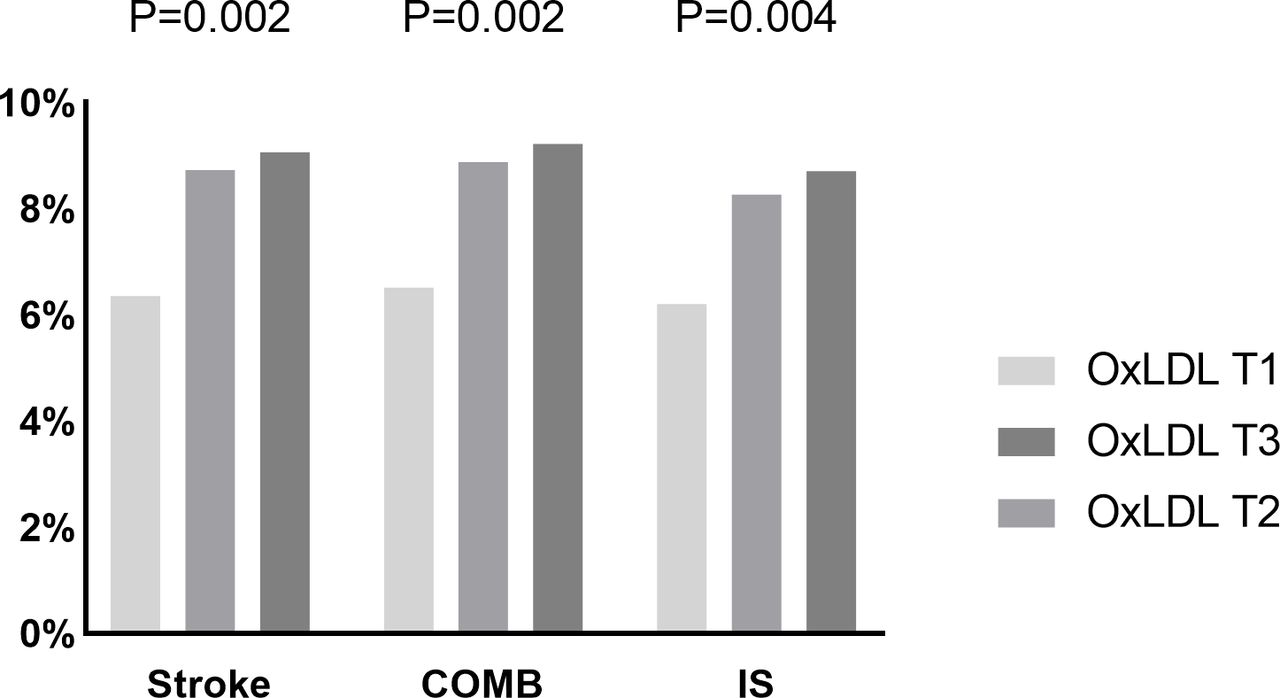
During the 90-day follow-up period, the rates of recurrent stroke, ischaemic stroke events, haemorrhagic stroke occurrences, composite vascular incidents and moderate to severe bleeding episodes were observed at 8.05%, 7.72%, 0.34%, 8.20% and 0.65%, respectively. The Kaplan-Meier survival analysis demonstrated that the tertile groups stratified based on oxLDL concentrations exhibited significant separation in stroke recurrence rates during the initial observation period, with this divergence becoming more pronounced as the follow-up duration progressed (figure 2). Individuals categorised in the upper oxLDL tertiles demonstrated an elevated incidence of cerebrovascular accidents, specifically ischaemic strokes, as well as a greater frequency of composite vascular occurrences during the 90-day follow-up period (see figure 3).

Kaplan-Meier curves of oxidised low-density lipoprotein (oxLDL) for recurrent stroke within 90 d.

Proportion of 90-day adverse outcome based on oxidised low-density lipoprotein (OxLDL) tertile. COMB, 3-month combined vascular event; IS, ischaemic stroke.
After adjusting for age, gender, BMI, history of ischaemic stroke, hypertension, diabetes mellitus, dyslipidaemia, application of agents before events, qualifying event, BP and baseline LDL, HDL, CHO, TG, APOA1, and APOB levels, a higher oxLDL level was associated with an increased risk of stroke recurrence and moderate-to-severe bleeding within 90 days. Patients in the highest tertile (T3) of oxLDL had a higher risk of stroke recurrence than those in the lowest tertile (T1) (HR 1.39, 95% CI 1.04 to 1.85, p=0.04). In patients with moderate to severe bleeding at 90 days, the corrected HR for the highest tertile of oxLDL compared with the lowest tertile was 3.61 (95% CI 1.26 to 10.34). Subjects in the T3 of oxLDL tended to have more composite vascular events than those in the T1 (HR 1.36 95% CI 1.02 to 1.81) (table 2). Following multifactorial adjustment, the traditional lipid indices LDL, HDL, TG, CHO, APOA1 and APOB were found to be of no predictive value for the recurrence of stroke. Conversely, oxLDL was identified as a significant predictor (online supplemental figure 1).
Supplementary data
HRs (95% CIs) for outcomes according to oxLDL grading
Changes in lipid indices at follow-up in patients
After 90 days of follow-up, we measured the levels of the patients’ lipid indices again: oxLDL, LDL, HDL, CHO, TG, APOA1 and APOB. We found that clopidogrel–aspirin therapy increased HDL levels more and decreased TG levels less compared with patients on aspirin therapy. However, no differences were found in the change values of oxLDL, LDL, CHO, APOA1 and APOB (online supplemental table 2). The study also showed that patients in the immediate intensive statin treatment group had a smaller reduction in LDL, CHO, APOB and TG levels and a greater increase in HDL levels than patients in the delayed statin treatment group (online supplemental table 3).
Supplementary data
Supplementary data
OxLDL levels and the effect of antiplatelet therapy, statin therapy and lipid-lowering before events.
The present study did not identify any interaction between oxLDL levels and antiplatelet therapy with regard to the occurrence of adverse outcomes (online supplemental table 4). In contrast, a significant interaction between oxLDL levels and statin therapy on the occurrence of bleeding events was identified in this study (P for interaction=0.0308). In the cohort of patients treated with immediate statin, elevated levels of oxLDL have been demonstrated to be a predictor of any bleeding events (HR 3.89 95% CI 1.83 to 8.29) (online supplemental table 5). At the same time, this study found no interaction between oxLDL levels and lipid-lowering before events in terms of the occurrence of adverse outcomes (online supplemental table 6).
Supplementary data
Supplementary data
Supplementary data
Discussion
This study examined the correlation between oxLDL levels and clinical outcomes in individuals diagnosed with acute minor ischaemic stroke or TIA at elevated risk, presenting with intracranial or extracranial atherosclerotic lesions. The main results indicated that oxLDL was an independent predictor of 90-day stroke recurrence and moderate-to-severe bleeding. All patients received lipid-lowering therapy during follow-up, and almost one-fifth received antihypertensive therapy, suggesting that the predictive value of baseline oxLDL applies to the intensively treated population.
OxLDL plays a pivotal role in the pathogenesis of atherosclerosis, whereby it promotes an inflammatory milieu and lipid accumulation within the arterial wall.15 Various studies have indicated a correlation between high oxLDL levels and the increased recurrence of cardiac events in patients with a history of cardiovascular disease. A longitudinal investigation conducted on a population scale revealed that elevated levels of circulating oxLDL exhibited a significant correlation with a heightened risk of developing metabolic syndrome over a 5-year observation period.16 The concentration of circulating oxLDL is indicative of the extent of systemic vascular inflammation and oxidative stress.17 A cohort study based on cardiovascular morbidity in a Chinese population revealed that serum oxLDL levels predicted the 10-year progression of subclinical carotid atherosclerosis, and this effect was independent of the CHO content of LDL particles, LDL size and the number of sdLDL particles.8
In recent years, studies have also emerged on the predictive value of circulating oxLDL for stroke recurrence. A study conducted on the CHANCE cohort revealed that elevated levels of oxLDL independently predicted recurrent stroke in patients with mild stroke and TIA.6 Furthermore, the ratio of oxLDL to HDL may serve as an indicator of recurrent stroke.9 Moreover, several studies have investigated the relationship between oxLDL and clinical symptoms in stroke patients. In patients with acute ischaemic stroke, plasma oxLDL levels were found to be positively correlated with NIHSS scores.10 Furthermore, oxLDL was significantly associated with 1-year poor prognosis and 1-year mortality in stroke subtypes with large-artery or small-artery atherosclerotic stroke.18 Partially consistent with past results, the present study also revealed the relationship between elevated oxLDL and adverse outcomes in patients with concomitant atherosclerotic stroke. The current subgroup study suggested that oxLDL may serve as an indicator to identify the risk for prognosis in stroke patients.
The underlying mechanisms for the association of oxLDL and adverse outcomes are not well elucidated. There were several potential explanations. OxLDL is formed by oxidative modification of LDL in response to a number of complex factors within the body. First, the lipid molecules on the surface of LDL are peroxidised, generating a large number of acetaldehyde complexes.19 These complexes then further modify the ApoB proteins (mainly lysine residues) to become oxLDL.20 The oxidative process has resulted in the acquisition of an important property of the oxLDL molecule: the ability to be recognised by the scavenger receptor, LOX-1 receptor and other similar receptors.21–23 This property allows oxLDL to interact with a wide range of cell types, which is the basis for the pathological function of oxLDL. OxLDL plays a pivotal role in the atherosclerotic process. On the one hand, oxLDL damages endothelial cells in the vessel wall and induces endothelial cell apoptosis, which results in increased endothelial permeability.24 Subsequently, subendothelial mononuclear macrophages phagocytose oxLDL and form foam cells.25 In addition, oxLDL exerts effects on smooth muscle cell proliferation, migration and apoptosis, which in turn influence plaque stability.26 The plaque further causes luminal narrowing and occlusion, which in turn leads to the development of cardiovascular and cerebrovascular diseases. The inclusion criteria for participants in this investigation necessitate the fulfilment of a minimum of one specified condition from the subsequent list: (1) a stenosis of 50% or more in either an intracranial or extracranial major artery, as verified through carotid duplex ultrasonography or angiographic examination, which may have contributed to the occurrence of infarction and its associated clinical symptoms or (2) the presence of acute multiple cerebral infarctions, attributed to atherosclerotic changes in the major cerebral arteries encompassing unstable non-sclerotic plaque formations, was verified through cranial CT or MRI examinations. OxLDL levels may reflect the degree of atherosclerosis as well as plaque stability and thus predict stroke recurrence. In the present study, we found no difference in the effect of dual antiplatelet therapy compared with antiplatelet therapy alone and immediate intensive statin therapy compared with delayed statin therapy on changes in oxLDL levels. This may suggest that oxLDL levels do not assess resistance to treatment, but the burden of the disease itself.
In patients with mild stroke or TIA, stroke recurrence is more likely in patients with increased atherosclerotic burden. In our study, all enrolled patients had atherosclerotic stroke. Circulating oxLDL affects plaque stability, which may explain the increased risk of stroke recurrence in stroke patients with concomitant atherosclerosis due to elevated oxLDL. In the meantime, our subgroup analysis of the INSPIRES trial demonstrated that elevated oxLDL levels were an independent predictor of moderate-to-severe bleeding in patients with mild stroke or TIA. This discovery could hold considerable importance, as existing diagnostic approaches lack reliable indicators for forecasting the probability of haemorrhagic stroke occurrences. The underlying mechanisms between oxLDL and bleeding need further investigation.
Although previous studies have demonstrated the predictive capacity of oxLDL in relation to stroke recurrence, the potential interaction between oxLDL and therapeutic effects remains undocumented. Consequently, we conducted a study to assess the impact of antiplatelet and intensive statin treatment modalities on the role of oxLDL in predicting adverse outcomes. The INSPIRES clinical investigation reveals that the administration of dual antiplatelet therapy comprising clopidogrel and aspirin within a 72-hour window following acute stroke manifestation significantly decreases the probability of subsequent cerebrovascular events within a 90-day period when contrasted with solitary aspirin treatment. This therapeutic advantage is particularly evident in cases presenting with minor ischaemic cerebrovascular accidents or TIAs with elevated risk profiles, where the underlying aetiology is attributed to atherosclerotic pathology.12 The present study did not identify any interaction between oxLDL levels and antiplatelet therapy with regard to the occurrence of adverse outcomes. Moreover, the modality of intensive statin therapy had no impact on the predictive role of oxLDL in recurrent stroke events. In the immediate statin therapy group, elevated levels of oxLDL were associated with an increased risk of any bleeding events. OxLDL is a reliable indicator of the extent of intravascular oxidative stress. Following the onset of an acute stroke, the activation of oxidative stress, inflammatory and vascular responses results in the release of a series of inflammatory factors, oxygen-free radicals and cytokines that disrupt the blood–brain barrier, thereby precipitating a haemorrhagic transformation.27 28 Nevertheless, the precise mechanism by which this occurs remains elusive.
Several limitations in our study need consideration. In this investigation, the oxLDL-4E6 antibody, used for quantifying circulating oxLDL concentrations, exhibited potential cross-reactivity with unmodified LDL. Its specificity relied heavily on sufficient lysine modifications present on APOB-10013, a factor that could introduce measurement inaccuracies. Second, the overall occurrence of moderate to severe bleeding is low in this study, which may result in bias. Furthermore, site-to-site variability also needs to be considered as a potential limitation.
Conclusions
In conclusion, a high level of oxLDL was suggestively associated with poor prognosis among individuals experiencing a minor acute stroke or TIA resulting from atherosclerotic lesions in either intracranial or extracranial arteries. If these results can be validated in additional studies, they may have clinical utility for identifying patients at high risk of stroke recurrence or bleeding.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethics committee of Beijing Tiantan Hospital (No.KY2017-065-02). Participants gave informed consent to participate in the study before taking part.
Footnotes
X @yilong
YD, LJ, TW and YC contributed equally.
Contributors All authors contributed to the study conception and design. Study concept and design: YW, GZ and WC. Acquisition of data: YD, LJ, YC and YP. Analysis and interpretation of data: YD, LJ, TW and XL. Drafting of the manuscript: YD and LJ. Statistical analysis: YP and HY. Critical revision of the manuscript for important intellectual content: YW and GZ. The author(s) read and approved the final manuscript. YW is responsible for the overall content (as guarantor).
Funding This work was supported by the Capital’s Funds for Health Improvement and Research (2024-1-2043), National Natural Science Foundation of China (No. 82425101, No.82101358), Beijing Nova Program (20230484336), Capital's Funds for Health Improvement and Research (2022-2-2045), the National Key R&D Program of China (No. 2022YFF1501500, 2022YFF1501501, 2022YFF1501502, 2022YFF1501503, 2022YFF1501504, 2022YFF1501505, 2017YFC1307900, 2017YFC1307905), Beijing Laboratory of Oral Health (PXM2021_014226_000041).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}
{kind=link}