

Article Figures & Data
Figures
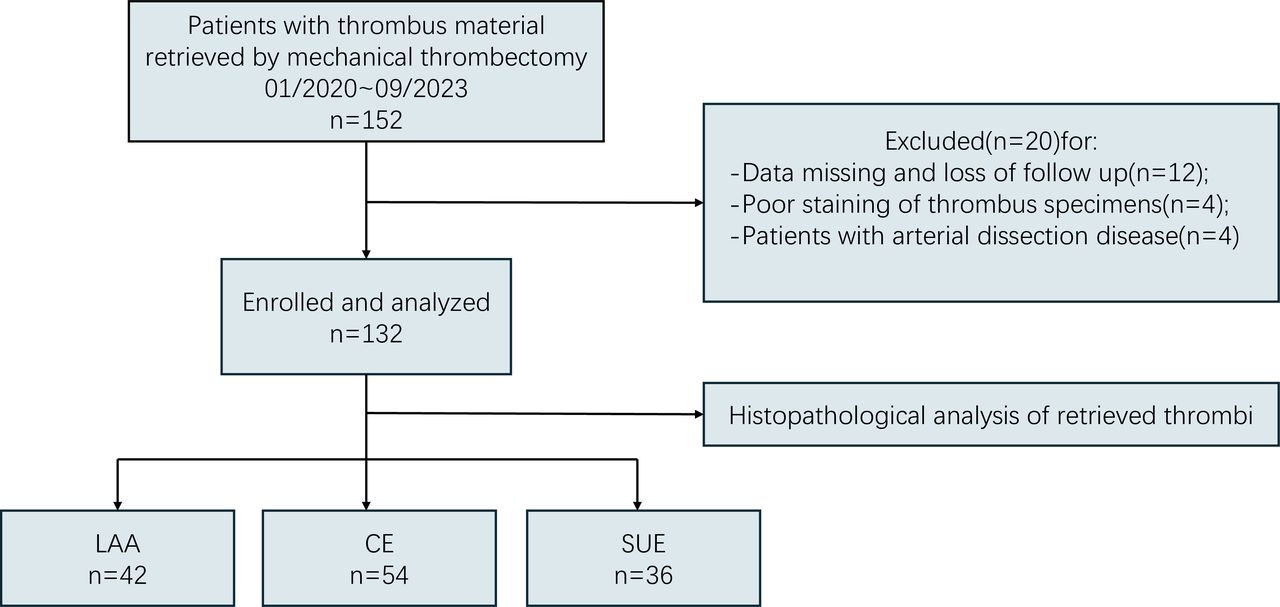
- Figure 1
Flow diagram of patients screened, enrolled and analysed. CE, cardioembolic; LAA, large artery atherosclerosis; SUE, stroke of undetermined aetiology;NIHSS, National Institute of Health Stroke Scale .
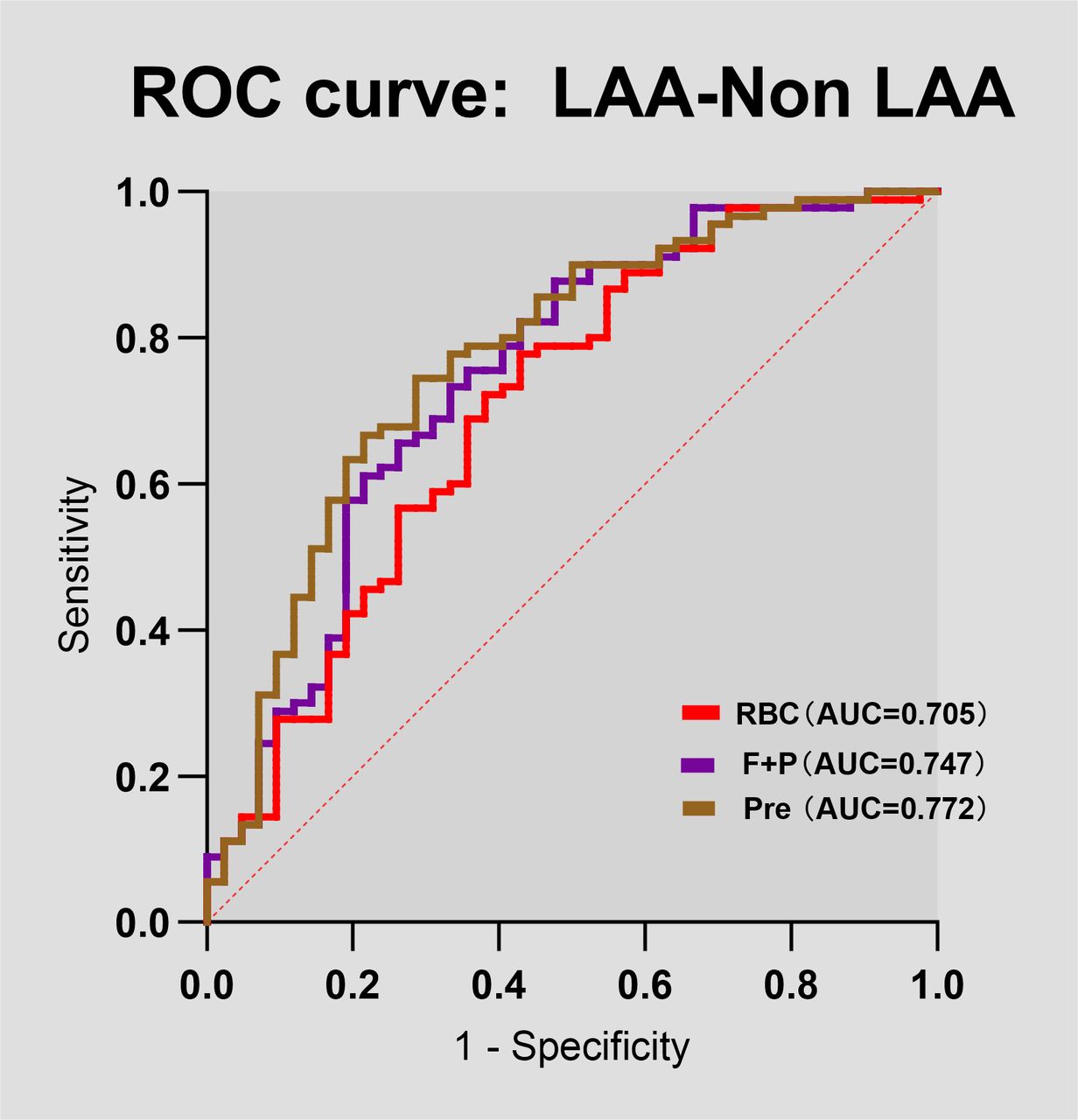
- Figure 2
Predictive value of thrombus components composition in discriminating stroke aetiology. The ROC curve displaying the performance of thrombus RBC, F+P content in discriminating a large artery atherosclerosis (LAA) aetiology from a non-LAA (non-LAA) aetiology. AUC, area under the curve; F+P, fibrin and platelet; Pre, the joint prediction probability; RBC, red blood cell; ROC, receiver operator characteristic; WBC, white blood cell.
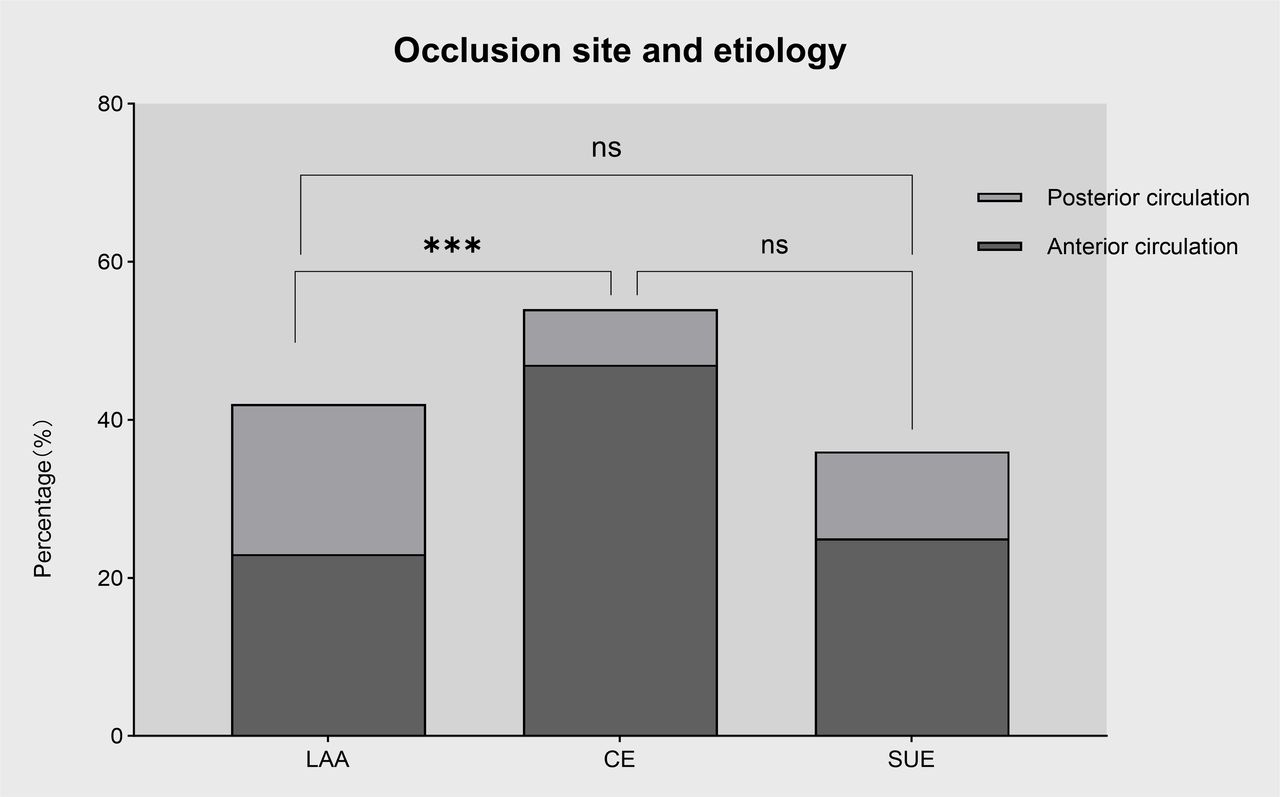
- Figure 3
Relationship between occlusion site and different aetiologies. There was a significant difference in occlusion site according to stroke subtype. Compared with LAA strokes, cardioembolic strokes were more likely to occur in the anterior circulation. ***p<0.001. CE, cardioembolic stroke; LAA, large artery atherosclerosis; SUE, stroke of undetermined aetiology.
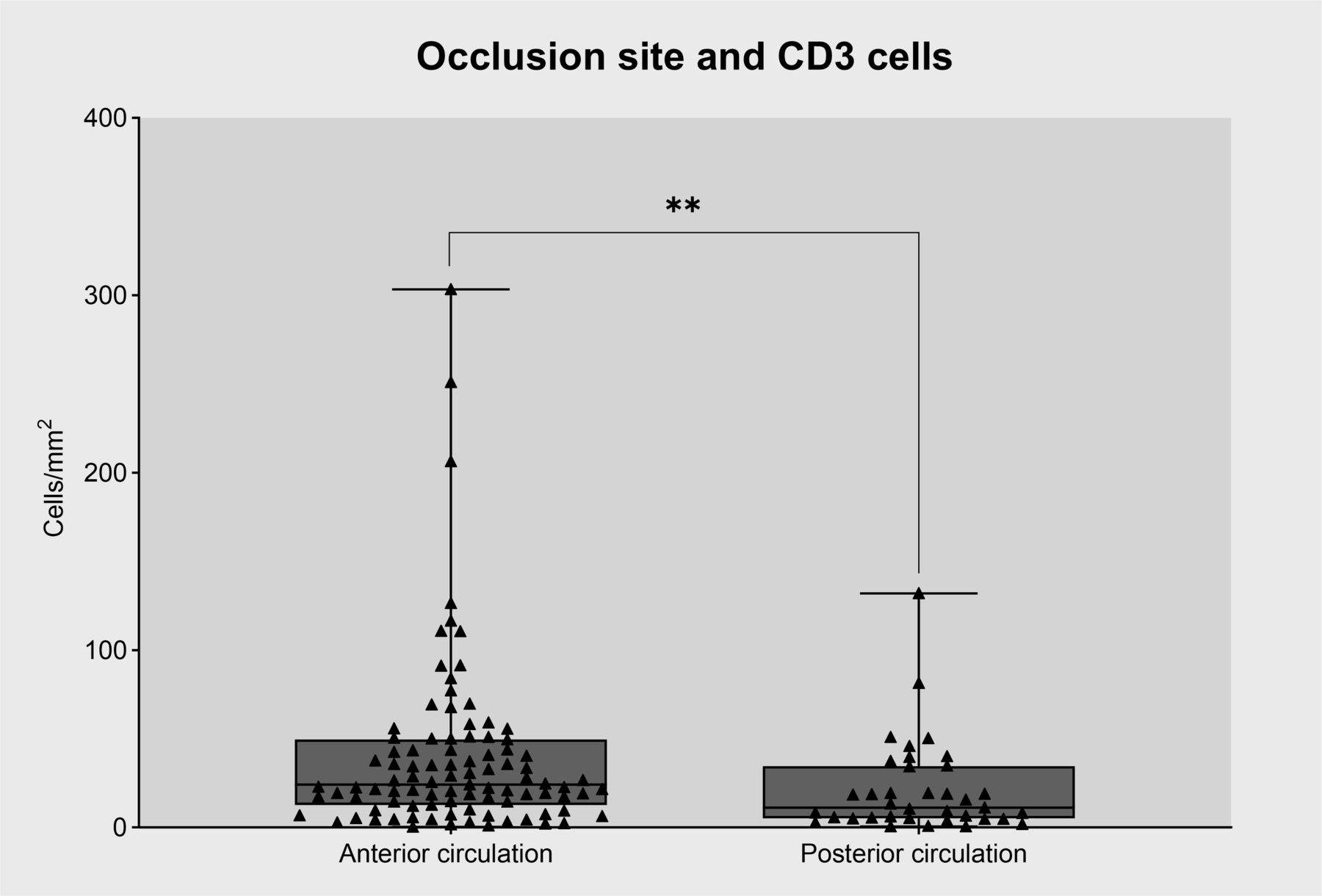
- Figure 4
Relationship between occlusion site and CD3+ cell content in intracranial thrombi. CD3+ cells were significantly more numerous in anterior circulation clots. **p<0.01.
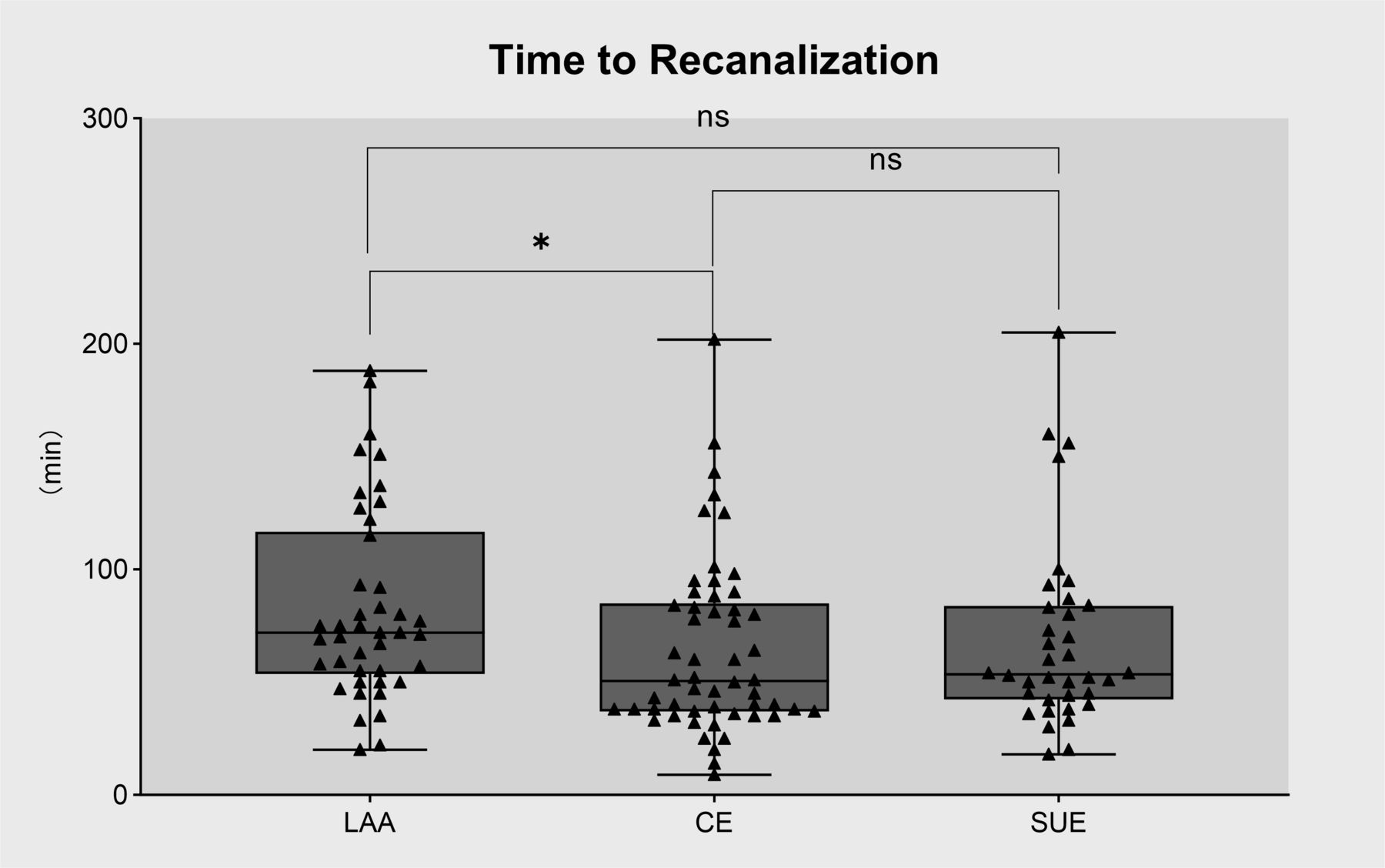
- Figure 5
Association between recanalisation time and thrombus composition in patients with different aetiologies. Patients with LAA strokes experienced longer reperfusion times than those with cardioembolic strokes. *p<0.05 . CE, cardioembolic stroke; LAA, large artery atherosclerosis; SUE, stroke of undetermined aetiology.





Tables
- Table 1
Clinical characteristics of the study population
Characteristic Total (n=132) LAA (n=42) CE (n=54) SUE (n=36) Age, years, mean (±SD) 65.3±13.1 62.4±11.5 70.5±11.8 60.8±14.4 Female, n (%) 45 (34.1) 6 (14.3) 33 (61.1) 6 (16.7) Vascular risk factors, n (%) Atrial fibrillation 56 (42.4) 0 (0.0) 51 (94.4) 5 (13.9) Hypertension 80 (60.6) 23 (54.8) 36 (66.7) 21 (58.3) Diabetes mellitus 38 (28.8) 14 (33.3) 12 (22.2) 12 (33.3) Dyslipidaemia 71 (53.8) 31 (73.8) 24 (44.4) 16 (44.4) History of stroke or TIA 26 (19.7) 11 (26.2) 11 (20.4) 4 (11.1) Smoking 49 (37.1) 23 (54.8) 13 (24.1) 13 (36.1) Coronary heart disease 39 (29.5) 7 (16.7) 24 (44.4) 8 (22.2) Valvular heart disease 10 (7.6) 0 (0.0) 9 (16.7) 1 (2.8) Patent foramen ovale 4 (3.0) 1 (2.4) 1 (1.9) 2 (5.6) Oral anticoagulation at baseline 29 (22.0) 0 (0.0) 23 (42.6) 6 (16.7) Antiplatelet therapy at baseline 22 (16.7) 8 (19.0) 8 (14.8) 6 (16.7) IV tPA 54 (40.9) 15 (35.7) 21 (38.9) 18 (50.0) NIHSS score on admission, median (IQR) 17.5 (12.25–23.0) 15.5 (10.0, 29.0) 18.0 (13.0, 21.0) 17.5 (13.5, 23.75) Occlusion site, n (%) ICA/MCA 95(72) 23 (54.8) 47 (87.0) 25 (69.4) VA/BA 37 (28) 19 (45.2) 7 (13.0) 11 (30.6) Thrombus components RBC, mean, % (±SD) 40.97±19.43 51.19±21.12 38.21±15.41 33.19±18.22 F+P, mean, % (±SD) 51.46±19.10 39.95±19.37 55.37±15.18 59.04±18.30 WBC, median, % (IQR) 6.88 (3.62–10.21) 7.61 (4.36–12.35) 5.86 (2.85–8.58) 8.18 (3.62, 10.82) CD3, median, cell/mm2 (IQR) 20.64 (7.61–42.11) 19.39 (6.45, 45.16) 20.64 (9.12, 34.91) 25.17 (6.08, 64.61) NETs, median, % (IQR) 1.03 (0.20–3.29) 0.86 (0.18, 2.34) 1.07 (0.17, 3.94) 1.16 (0.32, 5.53) Procedural outcome, median (IQR) Puncture-to-recanalisation time 60 (40–87.8) 72.0 (53.75, 116.75) 50.5 (37.0, 85.0) 53.5 (42.5, 83.75) No of manoeuvres 2 (1–2) 2.0 (1.0, 2.0) 2.0 (1.0,2.0) 2.0 (1.0, 3.0) Final mTICI score, n (%) 0–2 a 11 (8.3) 4 (9.5) 3 (5.6) 4 (11.1) 2b–3 121 (91.7) 38 (90.5) 51 (94.4) 32 (88.9) First-pass effect, n (%) 53 (40.2) 19 (45.2) 21 (38.9) 13 (36.1) Clinical outcome, n (%) Any haemorrhage events 51 (38.6) 14 (33.3) 23 (42.6) 14 (38.9) Parenchymal haemorrhage 32 (24.2) 9 (21.4) 14 (25.9) 9 (25.0) NIHSS score at discharge, median (IQR) 11 (5–31.8) 9.0 (3.0, 33.0) 12.5 (4.0, 29.75) 10.5 (5.25, 31.0) 90d mRS, median (IQR) 4.0 (2.0, 5.0) 3.0 (1.0, 5.0) 4.0 (2.0, 5.0) 4.0 (2.0, 5.0) 90d mRS, (0–2), n (%) 55 (41.7) 19 (45.2) 23 (42.6) 13 (36.1) Mortality within 90 days 23 (17.4) 7 (16.7) 9 (16.7) 7 (19.4) CE, cardiogenic embolism; F+P, fibrin and platelet; ICA, internal carotid artery; LAA, large artery atherosclerosis; MCA, middle cerebral artery; mRS, modified Rankin scale; mTICI, Thrombolysis in Cerebral Infarction scale; NETs, neutrophil extracellular traps; NIHSS, National Institute of Health Stroke Scale; RBC, red blood cell; SUE, stroke of undetermined aetiology; TIA, transient ischaemic attack; IV tPA, intravenous tissue plasminogen activator; VA/BA, vertebral artery/basilar artery; WBC, white blood cell.
- Table 2
Differences between thrombus composition and associated clinical data in stroke of different aetiologies
LAA (n=42) CE (n=54) SUE (n=36) P value RBC, mean, % (±SD) 51.19±21.12a 38.21±15.41b 33.19±18.22b <0.001 F+P, mean, % (±SD) 39.95±19.37a 55.37±15.19b 59.04±18.30b <0.001 WBC, median, % (IQR) 7.61 (4.36,12.35) 5.86 (2.85,8.58) 8.18 (3.62,10.82) 0.099 CD3, median, cells/mm2 (IQR) 19.39 (6.45,45.16) 20.64 (9.12,34.91) 25.17 (6.08,64.61) 0.545 NETs, median, % (IQR) 0.86 (0.18,2.34) 1.07 (0.17,3.94) 1.16 (0.32,5.53) 0.509 IV tPA, n (%) 15 (35.7) 21 (38.9) 18 (50.0) 0.408 NIHSS score on admission, median (IQR) 15.5 (10.0,29.0) 18.0 (13.0,21.0) 17.5 (13.5,23.75) 0.461 NIHSS score at discharge, median (IQR) 9.0 (3.0,33.0) 12.5 (4.0, 29.75) 10.5 (5.25,31.0) 0.691 Occlusion site, ICA/MCA, n (%) 23(54.8)a 47 (87.0)b 25 (69.4)a,b 0.002 Puncture-to-recanalisation time, median (IQR) 72.0(53.75,116.75)a 50.5 (37.0,85.0)b 53.5 (42.5,83.75)a,b 0.034 No of manoeuvres, median (IQR) 2.0 (1.0,2.0) 2.0 (1.0,2.0) 2.0 (1.0,3.0) 0.392 First-pass effect,n (%) 19 (45.2) 21 (38.9) 13 (36.1) 0.693 Final successful reperfusion (mTICI 2b and 3), n (%) 38 (90.5) 51 (94.4) 32 (88.9) 0.623 90-day mRS, median (IQR) 3.0 (1.0,5.0) 4.0 (2.0,5.0) 4.0 (2.0,5.0) 0.641 90-day mRS, good prognosis (mRS 0–2), n (%) 19 (45.2) 23 (42.6) 13 (36.1) 0.706 Mortality within 90 days 7 (16.7) 9 (16.7) 7 (19.4) 0.932 The Bonferroni method was used for multiple comparisons; the same letter indicated no statistical difference between groups and different letters indicated statistical difference between groups. The same letter indicates a significant difference between groups, and the same letter indicates no statistical difference, a/b indicate significant differences between groups. There were significant differences in RBC content (p<0.001) and fibrin/platelet content (p<0.001) between LAA group and CE group. There were significant differences in RBC (p<0.001) and fibrin/platelets (p<0.001) between the LAA group and the SUE group. There was no significant difference in RBC (p=0.201) and fibrin/platelets (p=0.330) between the CE and SUE groups. There was significant difference in time (p=0.032) between the CE and LAA puncture-to-recanalisation time groups.
CE, cardiogenic embolism; F+P, fibrin and platelet; ICA, internal carotid artery; LAA, large artery atherosclerosis; MCA, middle cerebral artery; mRS, modified Rankin scale; mTICI, Thrombolysis in Cerebral Infarction scale; NETs, neutrophil extracellular traps; NIHSS, National Institute of Health Stroke Scale; RBC, red blood cell; SUE, stroke of undetermined aetiology; IV tPA, intravenous tissue plasminogen activator; WBC, white blood cell.
Supplementary data





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}