

Article Figures & Data
Figures
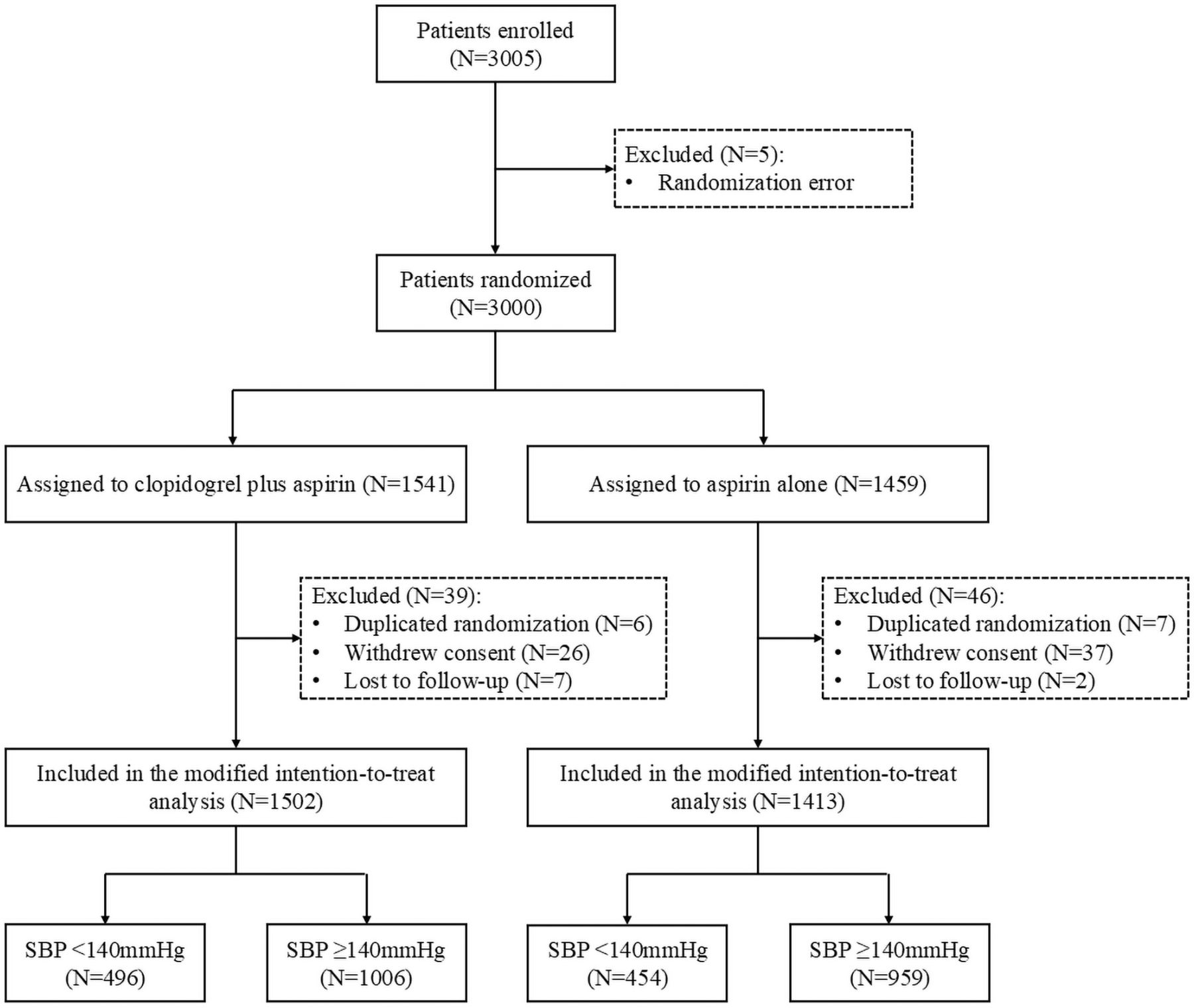
- Figure 1
Trial profile. SBP, systolic blood pressure.
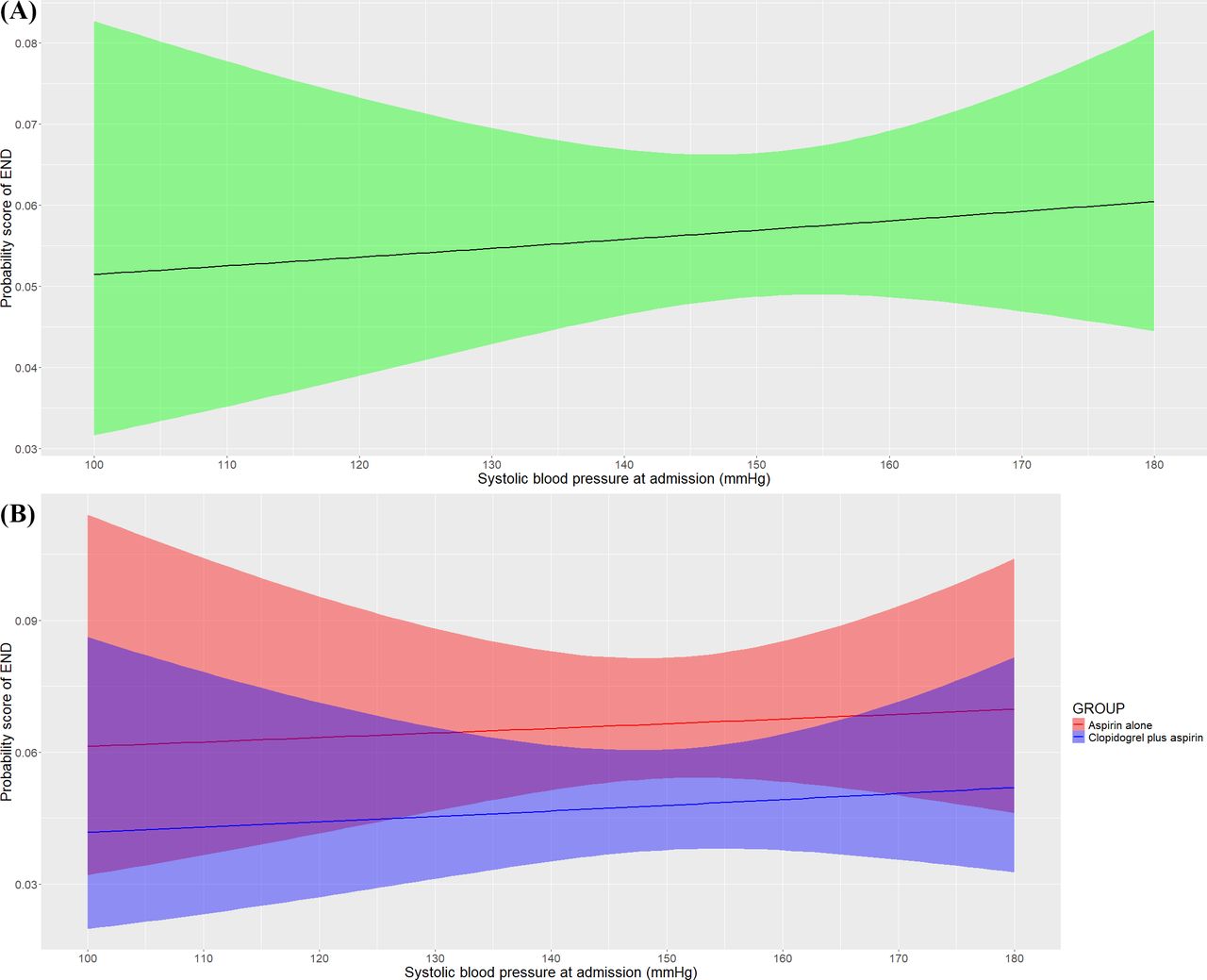
- Figure 2
Association of baseline SBP with risk of END. (A) The probability score of END at 7 days raised with SBP at admission increasing. (B) The probability score of END was stratified by treatment groups, raised as the SBP at admission increased in both two treatment groups and kept higher in the aspirin alone group, and the gap of probability score between treatment groups seemed to be consistent. The baseline SBP was associated with the risk of END (adjusted OR, 1.16; 95% CI, 1.08 to 1.24; p<0.001). END, early neurological deterioration; SBP, systolic blood pressure.
- Figure 3
Distribution of modified Rankin Scale Score at 90 days. The raw distribution of scores was shown in two treatment groups of all the patients (A), the patients with SBP≥140 mm Hg (B), and the patients with SBP<140 mm Hg (C). Scores ranged from 0 to 6. 0=no symptoms, 1=symptoms without clinically significant disability, 2=slight disability, 3=moderate disability, 4=moderately severe disability, 5=severe disability and 6=death. SBP, systolic blood pressure.



Tables
- Table 1
Baseline patient characteristics in the analysis
SBP<140 mm Hg SBP≥140 mm Hg P value§§ Total patients
(N=950)Clopidogrel plus aspirin (N=496) Aspirin alone
(N=454)P value Total patients
(N=1965)Clopidogrel plus aspirin (N=1006) Aspirin alone
(N=959)P value Age, years 65 (58–73) 66 (58–73) 65 (59–73) 0.46 66 (59–74) 66 (59–73) 66 (59–74) 0.11 0.27 Sex Male 657 (69.2) 344 (69.3) 313 (68.9) 0.89 1238 (63.0) 628 (62.4) 610 (63.6) 0.59 <0.01 Female 293 (30.8) 152 (30.6) 141 (31.1) 727 (37.0) 378 (37.6) 349 (36.4) Current smoking 325/942 (34.5) 165/491 (33.6) 160/451 (35.5) 0.55 642/1950 (32.9) 338/998 (33.9) 304/952 (31.9) 0.36 0.40 Current drinking* 190/941 (20.2) 104/491 (21.2) 86/450 (19.1) 0.43 400/1950 (20.5) 197/998 (19.7) 203/952 (21.3) 0.39 0.84 Comorbidities† Hypertension 448 (47.2) 229 (46.2) 219 (48.2) 0.52 1362 (69.3) 702 (69.8) 660 (68.8) 0.65 <0.01 Diabetes mellitus 238 (25.1) 115 (23.2) 123 (27.1) 0.17 504 (25.6) 286 (28.4) 218 (22.7) <0.01 0.73 Previous stroke‡ 327/942 (34.7) 176/490 (35.9) 151/452 (33.4) 0.42 612/1958 (31.3) 306/1001 (30.6) 306/957 (32.0) 0.50 0.06 Previous transient ischaemic attack 5/943 (0.5) 3/493 (0.6) 2/450 (0.4) 0.73 7/1951 (0.4) 4/1000 (0.4) 3/951 (0.3) 0.76 0.50 Blood pressure at randomisation, mm Hg Systolic 132 (126–140) 133 (127–140) 131 (125–140) 0.18 160 (151–176) 160 (151–177) 160 (151–176) 0.10 <0.01 Diastolic 80 (78–90) 80 (77–90) 80 (79–90) 0.97 90 (86–100) 92 (86–100) 90 (85–100) 0.08 <0.01 Blood glucose, mmol/L 5.9 (5.1–7.7) 5.9 (5.1–7.5) 5.9 (5.1–8.1) 0.89 6.1 (5.3–8.1) 6.2 (5.3–8.1) 6.1 (5.2–7.9) 0.41 <0.01 Baseline NIHSS score§ 4 (4-6) 4 (4-6) 5 (4-6) 0.80 5 (4-6) 5 (4-6) 5 (4-6) 0.87 0.04 Estimated premorbid function (mRS)¶ No symptoms 658 (69.3) 334 (67.3) 324 (71.4) 0.40 1414 (72.0) 722 (71.8) 692 (72.2) 0.38 0.26 Symptoms without disability 290 (30.5) 161 (32.5) 129 (28.4) 549 (27.9) 282 (28.0) 267 (27.8) Mild disability 2 (0.2) 1 (0.2) 1 (0.2) 2 (0.1) 2 (0.2) 0 (0.0) Time from stroke onset to antiplatelet therapy, hours 19.1 (8.2–26.0) 18.6 (8.1–26.0) 19.5 (8.3–26.1) 0.75 16.8 (7.4–26.1) 16.8 (7.1–26.0) 16.9 (7.8–26.3) 0.91 0.06 Presumed stroke cause** Undetermined cause 600/949 (63.2) 306/495 (61.8) 294 (64.8) 0.44 1172/1961 (59.8) 611/1004 (60.9) 561/957 (58.6) 0.28 0.18 Small artery occlusion 286/949 (30.1) 160/495 (32.3) 126 (27.8) 612/1961 (31.2) 294/1004 (29.3) 318/957 (33.2) Large artery atherosclerosis 28/949 (6.3) 28/495 (5.7) 32 (7.0) 165/1961 (8.4) 91/1004 (9.1) 74/957 (7.7) Other determined cause 2/949 (0.2) 1/495 (0.2) 1 (0.2) 9/1961 (0.5) 6/1004 (0.6) 3/957 (0.3) Cardioembolic 1/949 (0.1) 0/495 (0.0) 1 (0.2) 3/1961 (0.2) 2/1004 (0.2) 1/957 (0.1) Location of responsible vessel (identified by circulation infarction) Anterior 571/794 (71.9) 303/425 (71.3) 268/369 (72.6) 0.88 1209/1713 (70.6) 607/892 (68.0) 602/821 (73.3) <0.01 0.38 Posterior 195/794 (24.6) 106/425 (24.9) 89/369 (2.1) 456/1713 (26.6) 265/892 (29.7) 191/821 (23.3) Anterior and posterior 16/794 (3.8) 16/425 (3.8) 12/369 (3.3) 48/1713 (2.8) 20/892 (2.2) 28/821 (3.4) Patients receiving hypertension treatment†† 107 (11.3) 62 (12.5) 45 (9.9) 0.21 541 (27.5) 280 (27.8) 261 (27.2) 0.76 <0.01 Timing of starting treatment after admission, days 0 (0–4) 0 (0–4) 0 (0–4) 0.48 0 (0–2) 0 (0–2) 0 (0–2) 0.52 0.73 Patients receiving hyperglycaemia treatment‡‡ 93 (9.8) 45 (9.1) 4 (10.6) 0.44 223 (11.3) 121 (12.0) 102 (10.6) 0.33 0.20 Timing of starting treatment after admission, days 0 (0–1) 0 (0–1) 0 (0–1) 0.50 0 (0–1) 0 (0–1) 0 (0–2) 0.47 0.43 The data were shown with median (IQR) for continuous characteristic or frequency (percentages) for categorical characteristic.
*Current drinker means consuming alcohol at least once a week within 1 year before onset of the disease and consuming alcohol continuously for more than 1 year.
†The comorbidities were based on the patient or family report.
‡Previous ischaemic stroke referred only to the patients with prestroke mRS≤1.
§Patients with NIHSS scores of 4–10 were eligible for this study; NIHSS scores range from 0 to 42, with higher scores indicating more severe neurological deficit.
¶Scores on the mRS of functional disability range from 0 (no symptoms) to 6 (death). No symptoms indicates scoring 0, symptoms without disability indicates scoring 1, and mild disability indicates scoring 2.
**The presumed stroke cause was classified according to the Trial of Org 10 172 in Acute Stroke Treatment classification system20 using clinical findings, brain imaging and laboratory tests. Other determined causes included pulmonary embolism, peripheral vessel incident and cardiovascular incident.
††Type of antihypertension drug included ACE inhibitors and angiotensin receptor blocker (106/648), beta receptor blocker (15/648), calcium channel blocker (479/648), diuretic (5/648) and others (43/648).
‡‡The population included 742 patients who were diagnosed with diabetes mellitus and 130 patients who were found hyperglycaemia at admission.
§§The p value represented the significance when compared between SBP<140 mm Hg and SBP≥140 mm Hg subgroups.
mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; SBP, systolic blood pressure.
- Table 2
Association of categorical baseline systolic blood pressure with outcomes
Subgroup Clopidogrel plus aspirin (N=1502) Aspirin alone
(N=1413)Treatment effect metric Unadjusted Adjusted Pint value Treatment difference
(95% CI)P value Treatment difference
(95% CI)P value Primary outcome END at 7 days* SBP<140 mm Hg 17/496 (3.4) 19/454 (4.2) RD† −0.8 (−3.2 to 1.7) 0.54 −0.8 (−3.2 to 1.7) 0.54 0.50 SBP≥140 mm Hg 55/1006 (5.5) 76/959 (7.9) −2.5 (−4.7 to −0.2) 0.03 −2.5 (−4.1 to −1.0) <0.01 Secondary outcomes mRS 0–1 at 90 days‡ SBP<140 mm Hg 395/489 (80.8) 346/441 (78.5) RD† 2.3 (−2.9 to 7.5) 0.38 2.3 (−2.9 to 7.5) 0.38 0.90 SBP≥140 mm Hg 735/981 (74.9) 669/920 (72.7) 2.2 (−1.7 to 6.2) 0.27 2.2 (−0.6 to 5.0) 0.12 mRS at 90 days‡ SBP<140 mm Hg NA NA OR§ 1.07 (0.84 to 1.36) 0.59 1.07 (0.84 to 1.36) 0.59 0.96 SBP≥140 mm Hg NA NA 1.10 (0.93 to 1.29) 0.28 1.09 (0.97 to 1.23) 0.14 Change in NIHSS at 14 day¶ SBP<140 mm Hg −0.69 (−1.25 to −0.34) −0.65 (−1.61 to −0.34) GMR† 0.02 (−0.57 to 0.59) 0.96 −0.15 (−0.72 to 0.42) 0.60 0.98 SBP≥140 mm Hg −0.51 (−0.92 to −0.22) −0.51 (-0.92 to −0.22) 0.32 (−0.28 to 0.91) 0.29 0.32 (−0.09 to 0.73) 0.13 New stroke within 90 days** SBP<140 mmHg 3/489 (0.6) 3/441 (0.7) HR†† 0.90 (0.18 to 4.47) 0.90 0.90 (0.18 to 4.47) 0.90 0.74 SBP≥140 mm Hg 9/981 (0.9) 10/920 (1.1) 0.85 (0.34 to 2.08) 0.71 0.82 (0.33 to 2.04) 0.65 Other vascular events or death within 90 days SBP<140 mm Hg 6/489 (1.2) 2/441 (0.5) HR†† 2.72 (0.55 to 13.47) 0.22 2.72 (0.55 to 13.47) 0.22 0.39 SBP≥140 mm Hg 10/981 (1.0) 10/920 (1.1) 0.94 (0.39 to 2.25) 0.89 0.93 (0.39 to 2.24) 0.87 Safety outcomes Any bleeding events SBP<140 mm Hg 6/496 (1.2) 5/454 (1.1) RD† 0.1 (−1.3 to 1.5) 0.88 0.1 (−1.3 to 1.5) 0.88 0.65 SBP≥140 mm Hg 4/1006 (0.4) 9/959 (0.9) −0.5 (−1.3 to 0.2) 0.14 −0.5 (−1.1 to 0.0) 0.05 Intracranial haemorrhage SBP<140 mm Hg 1/496 (0.2) 1/454 (0.2) RD† 0.0 (−0.6 to 0.6) 0.95 0.0 (−0.6 to 0.6) 0.95 0.99 SBP≥140 mm Hg 0/1006 (0.0) 1/959 (0.1) −0.1 (−0.3 to 0.1) 0.31 −0.1 0.14 The data were shown with median (IQR) for continuous characteristic or frequency (percentages) for categorical characteristic.
*END was defined as an increase between baseline and 7 days of ≥2 on the NIHSS score, but not as result of cerebral haemorrhage.18
†Calculated using the generalised liner model.
‡Scores on the mRS of functional disability range from 0 (no symptoms) to 6 (death).
§A shift measures of function according to the full range of scores on the mRS at 90 days was analysed by ordinal logistic regression.
¶Patients with NIHSS scores of 4–10 were eligible for this study; NIHSS scores range from 0 to 42, with higher scores indicating more severe neurological deficit. The log (NIHSS+1) was analysed using generalised linear model.
**New stroke included ischaemic stroke and haemorrhagic stroke.
††Calculated using the Cox regression model.
END, early neurological deterioration; GMR, geometric mean ratio; mRS, modified Rankin Scale; NA, not applicable; NIHSS, National Institute of Health Stroke Scale; RD, risk difference; SBP, systolic blood pressure.
- Table 3
Propensity score matching analysis for primary outcome
Primary outcome Subgroup Clopidogrel plus aspirin Aspirin alone RD (95% CI)* P value Pint value END at 7 days† SBP<140 mm Hg (N=940) 17/490 (3.5) 19/450 (4.2) −0.8 (−3.2 to 1.7) 0.55 0.91 SBP≥140 mm Hg
(N=940)27/494 (5.5) 31/446 (7.0) −1.5 (−4.6 to 1.6) 0.35 *Calculated using the generalised liner model.
†END was defined as an increase between baseline and 7 days of ≥2 on the NIHSS score, but not as result of cerebral haemorrhage.18
END, early neurological deterioration; NIHSS, National Institutes of Health Stroke Scale; RD, risk difference; SBP, systolic blood pressure.





{kind=link}
{kind=link}
{kind=link}