

Abstract
Background Recently, computational fluid dynamics (CFD) has been used to simulate blood flow of symptomatic intracranial atherosclerotic stenosis (sICAS) and investigate the clinical implications of its haemodynamic features, which were systematically reviewed in this study.
Methods Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses and Meta-analysis of Observational Studies in Epidemiology statements, we searched PubMed and Embase up to March 2024 and screened for articles reporting clinical implications of haemodynamic parameters in sICAS derived from CFD models.
Results 19 articles met the inclusion criteria, all studies recruiting patients from China. Most studies used CT angiography (CTA) as the source image for vessel segmentation, and generic boundary conditions, rigid vessel wall and Newtonian fluid assumptions for CFD modelling, in patients with 50%-99% sICAS. Pressure and wall shear stress (WSS) were quantified in almost all studies, and the translesional changes in pressure and WSS were usually quantified with a poststenotic to prestenotic pressure ratio (PR) and stenotic-throat to prestenotic WSS ratio (WSSR). Lower PR was associated with more severe stenosis, better leptomeningeal collaterals, prolonged perfusion time and internal borderzone infarcts. Higher WSSR and other WSS measures were associated with positive vessel wall remodelling, regression of luminal stenosis and artery-to-artery embolism. Lower PR and higher WSSR were both associated with the presence and severity of cerebral small vessel disease. Moreover, translesional PR and WSSR were promising predictors for stroke recurrence in medically treated patients with sICAS and outcomes after acute reperfusion therapy, which also provided indicators to assess the effects of stenting treatment on focal haemodynamics.
Conclusions CFD is a promising tool in investigating the pathophysiology of ICAS and in risk stratification of patients with sICAS. Future studies are warranted for standardisation of the modelling methods and validation of the simulation results in sICAS, for its wider applications in clinical research and practice.
WHAT IS ALREADY KNOWN ON THIS TOPIC
CFD is an emerging tool to investigate haemodynamic patterns of sICAS and its clinical implications. However, the CFD modelling methodology, haemodynamic parameters and clinical implications investigated varied among previous studies.
WHAT THIS STUDY ADDS
In a systematic review, we summarized the CFD modelling methodology, haemodynamic parameters of interest and their associations with other imaging markers and clinical indicators, in existing studies using the CFD technique to investigate haemodynamics of sICAS.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This review article provides a summary of the clinical implications of haemodynamics in sICAS based on the CFD technique. It advocates standardisation and validation of the modelling methodology and findings, for future research advance in this area.
Introduction
Intracranial atherosclerotic stenosis (ICAS) is a common cause of ischaemic stroke and transient ischaemic attack (TIA), which accounts for 30%–50% of all ischaemic strokes in Asians and 8%–10% in Caucasians.1 2 Despite optimal medical treatment, patients with stroke or TIA due to ICAS, that is, symptomatic ICAS (sICAS), have a considerable risk of recurrent stroke.3 4 ICAS can be diagnosed with a variety of modalities, such as transcranial Doppler (TCD), MR angiography (MRA), CT angiography (CTA) and digital subtraction angiography (DSA).5 While these imaging techniques are useful tools in identifying vessel lumen changes secondary to atherosclerosis, another emerging tool, computational fluid dynamics (CFD), could furnish other valuable characteristics in ICAS.
CFD, modelling flow pattern by solving equations of fluid dynamics, has been a useful tool for researching haemodynamics in cardiovascular and cerebrovascular diseases, for example, wall shear stress (WSS), velocity and pressure.6 Recent studies indicated that CFD is also promising in studying haemodynamics and relevant clinical implications in sICAS.7 Yet, the CFD modelling results rely very much on the assumptions on blood, vessel wall and boundary conditions, which have varied among previous studies in sICAS. The haemodynamic parameters and the clinical implications also differed among previous studies. These may have hindered generalisability of the findings and further progress in this area. We therefore performed this systematic review, summarising the modelling methodology, haemodynamic parameters of interest and the associations with other imaging and clinical indicators, in existing studies using the CFD method to analyse haemodynamics of sICAS. We also intended to discuss limitations of existing studies and propose some future research directions, in the hope of advocating more investigations and advances in this area.
Methods
We conducted this study following Preferred Reporting Items for Systematic Reviews and Meta-Analyses and Meta-analysis of Observational Studies in Epidemiology statements.8 9 We searched PubMed and Embase database with English full-text articles between January 2000 and March 2024. Key searching terms included ‘intracranial arter*’, ‘cerebral arter*’, ‘steno*’, ‘occlus*’ and ‘atherosclero*’, in combination with ‘haemodynamic*’ and ‘computational fluid dynamic*’ (online supplemental tables S1,S2). Reference lists were also manually searched for eligible studies.
Supplementary data
Study inclusion criteria were (1) cross-sectional or longitudinal study recruiting patients with sICAS, (2) using CFD models to study focal (adjacent to ICAS lesion) or global cerebral haemodynamics and (3) reporting clinical implications of the haemodynamic metrics from CFD models, for example, associations of the haemodynamic metrics with other imaging markers or clinical features/outcomes. Animal/experimental studies, pure technical papers with no imaging or clinical association investigations, studies simply verifying the CFD-based haemodynamic parameters with invasively measured counterparts, case reports/series or studies with sample size <10 cases, and review, letter and comment articles were excluded. Studies involving both patients with sICAS and patients with extracranial atherosclerotic stenosis, without separate data on those with sICAS, were also excluded.
Study characteristics, haemodynamic parameters and the main findings on clinical implications were extracted. The risk of bias was assessed. More details over the methods are described in online supplemental methods.
Results
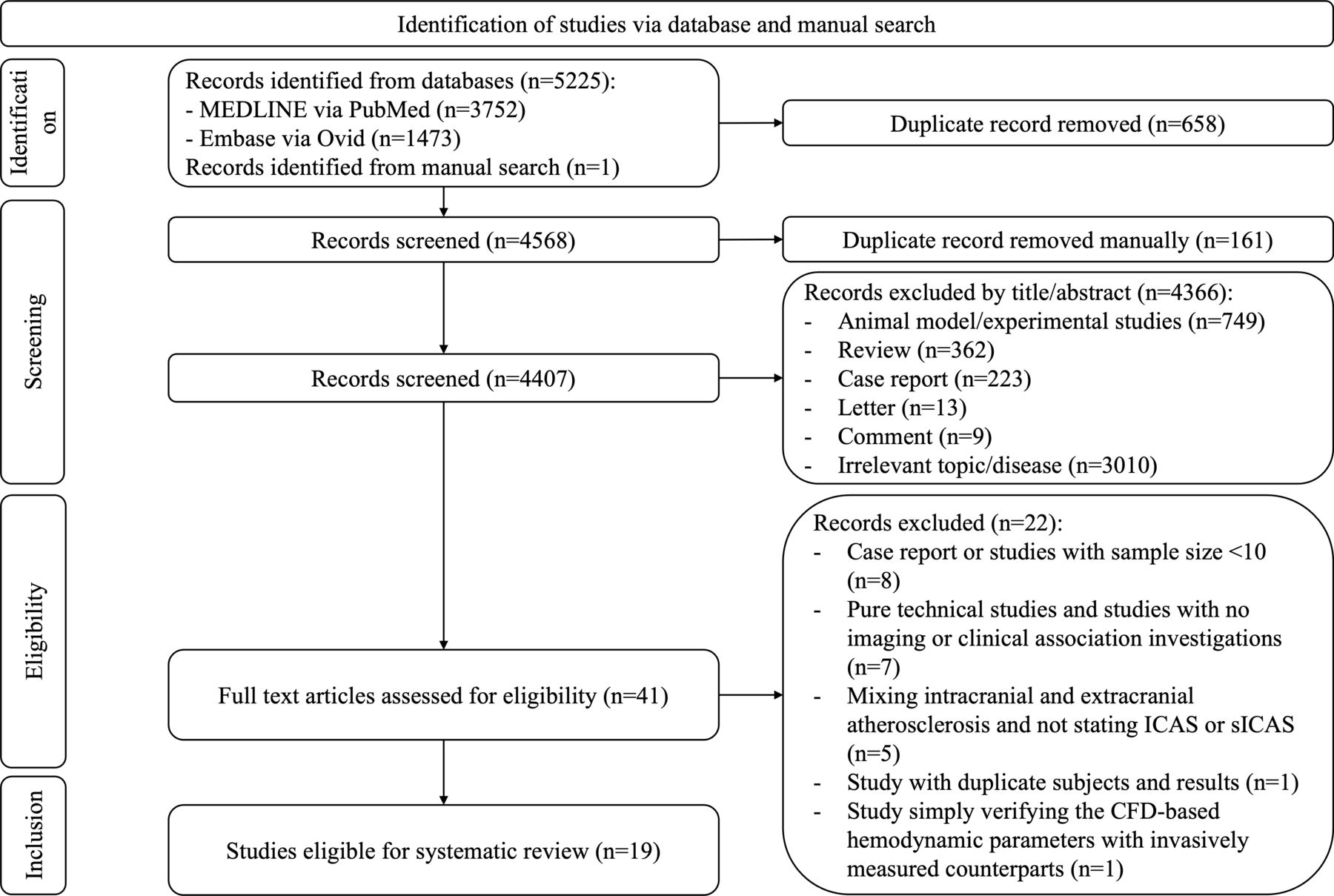
Among the 5226 articles identified through literature search, 40 remained after screening the title and abstract, of which 19 studies met the inclusion criteria (figure 1).

Flow chart for study screening. CFD, computational fluid dynamics; ICAS, intracranial atherosclerotic stenosis; sICAS, symptomatic intracranial atherosclerotic stenosis.
Study and patient characteristics
Study characteristics were summarised in table 1, and detailed CFD model setup and clinical implications of each study were described in online supplemental table S3). Of the 19 studies included, 5 were published between 2014 and 2019 and 14 published after 2020. All studies were conducted in China. Regarding the sICAS lesion, 13 and 4 studies, respectively, recruited patients with 50%–99% and 70%–99% stenosis. Additionally, two studies focused on 30%–99% and 50%–70% stenosis, respectively. Nine and one studies limited sICAS in the anterior circulation or posterior circulation, respectively, and nine studies involved both circulations. The sample size was >100 in 5 studies. Most of the included studies were observational and retrospective, and 11 of them had a low risk of bias (online supplemental table S4).
Study characteristics of the 19 primary studies included in this systematic review
CFD modelling methods
CFD modelling for ICAS mostly involves the following steps: (1) reconstruction of the arteries of interest from source images of neurovascular exams; (2) generation of a mesh in the vessel lumen, wall and inlet/outlet; (3) setup of boundary conditions on inlet/outlet and blood properties; (4) simulation of blood flow by solving fluid dynamics equations and (5) postprocessing of haemodynamic parameters (online supplemental figure S1). The software used for CFD modelling in the 19 primary studies was listed in online supplemental table S5).
Supplementary data
Most studies used CTA as the source images for vessel segmentation, others used time-of-flight MRA, three-dimensional rotational angiography and biplane DSA. In the CFD model setup, most studies used generic boundary conditions, rigid with no-slip vessel wall and Newtonian blood assumptions. Five studies used patient-specific inlet or outlet boundary conditions. Among them, two studies used lumped parameter models to simulate microcirculation resistance on the outlet, and Liu et al also considered vascular compliance.10 11 Raynald et al developed an innovative computational approach, incorporating patient-specific measurements of pressure-wire and CFD simulation, to evaluate microcirculation resistance and blood flow, which was strongly correlated with TCD-based volumetric flow measurements.12 Six studies simulated transient-state blood flow, while other studies conducted steady-state simulations.
Haemodynamic metrics of interest
Regarding the haemodynamic features, most studies quantified pressure and WSS across the sICAS lesion, and other studies also assessed shear strain rate (SSR), velocity and vorticity.
15 studies used various terms to reflect the pressure change across a sICAS lesion, including pressure ratio (PR) and absolute pressure gradient. PR was calculated as poststenotic pressure distal to the lesion divided by prestenotic pressure in the proximally normal artery segment. The pressure gradient was calculated as the absolute value of prestenotic pressure minus poststenotic pressure.
Seven studies assessed WSS, such as WSS ratio (WSSR) or relative WSS (rWSS). Most studies used WSSR, calculated as WSS at the stenotic-throat divided by prestenotic WSS, to reflect WSS change across a sICAS lesion. Some other studies measured rWSS at one location on the vessel wall across a sICAS lesion,13 calculated as the ratio of the absolute WSS value at one location and the mean WSS value across the circumference in the proximally normal artery segment. The principles of calculating WSSR and rWSS were similar, both to offset the effects of individual arterial geometry on focal WSS in comparing the WSS values among individuals.
Other studies also evaluated SSR, velocity, vorticity and their related parameters. Leng et al and Nam et al calculated the ratio of SSR at the stenotic-throat and at the prestenotic arterial segment, and similarly the velocity ratio, to reflect the velocity changes across the sICAS lesion.14 15
Correlations of the haemodynamic metrics with anatomical characteristics of the sICAS lesions in cross-sectional and longitudinal studies
In cross-sectional studies, Nam et al observed in-average lower PR, higher SSR ratio and higher velocity ratio in severe (70%–99%) sICAS lesions than moderate (50%–69%) stenosis (all p<0.001).15 However, PR might not be linearly proportional to the stenosis rate in sICAS, according to Liu et al.11 In addition, Zhang et al found higher WSSR (medians 9.98 vs 5.99, p=0.004) and WSS (means 53.99 Pa vs 39.98 Pa, p=0.023) at the narrowest location in patients with symptomatic middle cerebral artery (MCA) stenosis with positive remodelling than those with negative remodelling in high-resolution MRI (HRMRI), while the remodelling index (Pearson’s r=0.376, p=0.026) and plaque area (Pearson’s r=0.407, p=0.015) were positively correlated with WSSR.16 In a longitudinal study, Lan et al associated a higher maximum WSS (adjusted OR (aOR), 1.20; 95 % CI, 1.03 to 1.39; p=0.019) and larger mean rWSS of the high-WSS region (aOR, 1.53; 95% CI, 1.07 to 2.19; p=0.021) with regression of luminal stenosis in sICAS in CTA over 1 year, in medically treated patients; such associations were similar when analysing the proximal and distal segments of the lesion separately.13 It was speculated that positive remodelling may play a role underlying such associations, which, however, could not be verified in this study using CTA only to assess features of the sICAS lesions. These findings indicated complicated relationships between the haemodynamic and anatomical features of sICAS lesions that warrant further investigations.
Correlations with collateral and perfusion status in cross-sectional studies
In cross-sectional studies, CFD models were used to investigate haemodynamic metrics affecting leptomeningeal collateral (LMC) and perfusion status in patients with sICAS. Leng et al found the correlation of a larger pressure gradient with better LMCs in patients with sICAS (aOR for 10 mm Hg increment in absolute pressure gradient, 1.70; 95% CI, 1.06 to 2.74; p=0.029), which indicated a significant translesional pressure drop served as a driving force for recruiting LMCs.17 In addition, Lan et al investigated the interrelationships among antegrade residual flow through symptomatic MCA stenosis (as reflected by translesional PR in CFD models), LMC flow assessed in CTA that could retrogradely perfuse distal brain territories and the overall cerebral perfusion measured in CT perfusion (CTP).18 The study showed lower PR (means 0.79 vs 0.90, p=0.015) and better LMC status (56.7% vs 34.5% with good LMCs, p=0.079) among patients with severe stenosis (70%–99%) than those with moderate stenosis (50%–69%). Moreover, the study also indicated that cerebral perfusion in the supplying territory of a stenotic MCA may depend more on LMC flow (Pearson’s r=0.038, p=0.051) among patients with severe stenosis but more on antegrade residual flow (Pearson’s r=−0.605, p<0.001) among those with moderate stenosis. In another study, Wang et al found a negative correlation between PR and Tmax (Spearman’s r=−0.73, p<0.01), the duration to the maximum of residue function in perfusion-weighted MRI, which means a larger translesional pressure gradient associating with prolonged perfusion time.19 Yin et al found a significantly lower PR in patients with sICAS with apparent hypoperfusion than those with normal perfusion defined in 4D CTA (means 0.38 vs 0.76, p<0.01), although the sample size was small for the analysis (n=10).10 In addition, Raynald et al observed a good agreement on the blood flow rate derived from CFD modelling and TCD measurements (mean difference: −0.78 mL/s, p for Bland-Altman test=0.027), while the mean velocities showed less agreement between CFD simulation and TCD measurements (mean difference: −0.05 cm/s, p for Bland-Altman test=0.399), which indicated greatly varied flow resistance among individuals.12
Overall, these studies have revealed the role of translesional pressure gradient across sICAS lesions in affecting the distal collateral and perfusion status, while various factors could affect these relationships. Of note, none of these studies reported data separately in patients with posterior-circulation sICAS, for whom standard perfusion parameters have not been established and more investigations are needed.
Correlations with stroke mechanisms in cross-sectional studies
ICAS can cause an ischaemic stroke or TIA via different mechanisms with different infarct topography, for example, hypoperfusion (usually with borderzone infarcts), artery-to-artery embolism (usually with multiple cortical or territorial infarcts) and parent artery atherosclerosis occluding penetrating artery (usually with single subcortical small infarct). The stroke mechanisms have been associated with different risks of stroke relapse in medically treated patients with sICAS.20 The associations between haemodynamic features of sICAS in CFD models and stroke mechanisms have been investigated in studies by Feng et al 21 and Li et al.22 First, Feng et al found high WSSR as an independent predictor of artery-to-artery embolism as a stroke mechanism (aOR, 3.90; 95% CI, 1.22 to 12.47; p=0.022), in patients with sICAS in the anterior circulation.21 More interestingly, such association was more prominent in those with a low PR (large translesional pressure gradient). In addition, Li et al compared haemodynamic features of sICAS lesions and other imaging characteristics between patients with sICAS with internal and cortical borderzone infarcts, in whom hypoperfusion has usually been considered as the stroke mechanism.22 They found low PR (PR≤median) independently associated with internal borderzone infarcts (aOR: 4.22, p=0.026) and higher incidence of coexisting small cortical infarcts in those with cortical borderzone infarcts. The findings suggested artery-to-artery embolism as a possible pathogenic mechanism underlying cortical borderzone infarcts, which was against previous speculations. Overall, these studies indicated important roles of haemodynamics in determining the stroke mechanisms in sICAS, while further studies are needed to explain and verify the findings.
Correlations with cerebral small vessel disease in cross-sectional study
Cerebral small vessel disease (CSVD) commonly coexists with ICAS, particularly in older individuals.23 In a cross-sectional study, Zheng et al 24 associated abnormal PR (PR≤median) and WSSR (WSSR≥fourth quartile) with moderate-to-severe white matter hyperintensities (aOR: 10.12, p=0.018), presence of cortical microinfarcts (aOR: 5.25, p=0.003) and moderate-to-severe overall CSVD burden (aOR: 12.55, p=0.033) in the ipsilateral hemisphere to sICAS, independent of these CSVD imaging markers and overall burden in the contralateral hemisphere. The study indicated the role of haemodynamics in affecting the severity of CSVD in patients with sICAS.
Correlations with risk of recurrent stroke in medically treated patients with sICAS
In a pilot study, Leng et al 14 associated higher SSR ratio (HR, 1.03; 95% CI, 1.00 to 1.05; p=0.023) and higher velocity ratio (HR, 1.03, 95% CI, 1.00 to 1.06; p=0.035) with a higher risk of recurrent ischaemic stroke in the same territory within 1 year, in medically treated patients with sICAS with 70%–99% stenosis. Additionally, a lower PR also tended to be correlated with the stroke risk, however, which did not achieve statistical importance (HR, 0.98; 95% CI, 0.97 to 1.00; p=0.074). This study demonstrated that stenosis rate may not be the sole or primary indicator for assessing the risk of recurrent stroke in patients with sICAS. In the subsequent Stroke Risk and Haemodynamics in Intracranial Atherosclerotic Disease (SOpHIA) study of 245 patients with sICAS with 50%–99% stenosis, low PR (PR≤median, adjusted HR (aHR), 3.16; 95% CI, 1.15 to 8.72; p=0.026) and high WSSR (WSSR≥4th quartile, aHR, 3.05; 95% CI, 1.25 to 7.41; p=0.014) were independently correlated with a higher risk of stroke relapse in the same territory.7 Based on the SOpHIA cohort, Tian et al developed a D2H2A nomogram to predict recurrent ischaemic stroke in the same territory in patients with sICAS.25 Diabetes, dyslipidaemia, haemodynamic status (PR and WSSR), hypertension and age ≥50 years were incorporated in the predictive model, which could be a useful tool to stratify patients with sICAS receiving medical treatment. Further, in a substudy of SOpHIA, Feng et al 26 divided 157 patients with 50%–99% sICAS into normal PR (PR>median) and low PR (PR≤median) groups and investigated the influence of PR on the association between systolic blood pressure (SBP) levels throughout follow-up (SBPFU) and the risk of recurrent stroke in the same territory, in medically treated patients with sICAS. They found patients with normal PR and lower SBPFU had a significantly decreased risk of recurrent stroke (HR for 10 mm Hg decrement, 0.46, 95% CI, 0.24 to 0.88; p=0.018); yet, patients with low PR and SBPFU≤130 mm Hg had an increased risk of recurrent stroke, relative to 130<SBPFU<150 mm Hg (HR, 5.08; 95%CI, 1.05 to 24.49; p=0.043).
Correlations with functional outcome in patients with sICAS receiving acute reperfusion therapy
In patients with 50%–99% sICAS in MCA who mostly received intravenous thrombolysis and some received acute endovascular treatment, Wu et al associated the WSSR before treatment (OR:0.86, 95%CI:0.75 to 0.99, p=0.041) and the difference of WSSR before and after treatment (OR, 0.72; 95% CI, 0.52 to 1.03; p=0.043) with the functional outcome by modified Rankin Scale at 3 months.27 In contrast to prediction models solely incorporating clinical variables, the inclusion of haemodynamic metrics may enhance the predictive capacity for functional outcomes in such patients (p<0.05).
Changes of the haemodynamic parameters in sICAS with stenting treatment
In patients with severe M1 MCA stenosis, Zhang et al reported that successful stenting could reduce the pressure loss across the sICAS lesion compared with that before stenting (means 6.46 Pa vs 12.84 Pa, p<0.001), which could enhance antegrade blood flow.28 In patients with severe basilar artery stenosis, Zhou et al found significantly reduced WSS (means 14.84 Pa vs 139.49 Pa, p<0.001) at the stenosis segment after stenting treatment.29
Discussion
In this study, we overviewed the CFD modelling methodology and the haemodynamic parameters of interest in sICAS in previous relevant studies, moreover, the clinical implications of the findings. Most of the studies recruited patients with sICAS with 50%–99% or 70%–99% stenosis in the anterior and posterior circulations. Regarding CFD methodology, many studies used CTA as the source image for artery reconstruction, and generic boundary conditions, rigid with no-slip vessel and Newtonian blood assumptions with steady-state simulations. Pressure and WSS, and their changes across the lesion, were most often used to assess the haemodynamic impact of sICAS lesions. In cross-sectional and longitudinal studies, haemodynamic metrics from CFD models were correlated with the stenosis rate and plaque characteristics of sICAS, the collateral and perfusion status, the stroke mechanism as well as the presence and severity of CSVD. The haemodynamic metrics obtained from CFD models were also promising predictors for the risk of recurrent stroke in medically treated patients with sICAS and outcomes after intravenous thrombolysis or endovascular treatment, which also provided indicators to assess the effects of stenting treatment on focal haemodynamics.
CFD is a promising technique to quantify the haemodynamic impact of sICAS and to investigate the clinical implications of the haemodynamic parameters. To conduct valid CFD modelling in sICAS, it is crucial to obtain accurate three-dimensional geometry of arteries of interest and set up proper boundary conditions and blood properties. However, there are limitations with the current CFD modelling methodology, which may have hindered its application in ICAS research and clinical practice. First, CFD modelling is time-consuming and complex. Second, current CFD models lack patient-specific data. In recent studies in patients with sICAS, the boundary conditions are usually set using estimates from previous studies or based on physiological models. Deep learning techniques may address these issues, which could decrease the expansive computational time for complex biomedical problems, and help to solve problems when boundary conditions are unknown.30 Third, the Newtonian assumption of blood and hence a constant viscosity are used in most studies for simplicity, although blood flow is non-Newtonian. However, CFD models simulated with Newtonian and non-Newtonian conditions in severe ICAS cases may yield significant differences of WSS estimates in areas with low WSS values, according to a small-scale study.31 Finally, although several preliminary studies have validated the haemodynamic measures obtained from CFD modelling with other non-invasive or invasive measuring methods. for example, conventional CT or MR perfusion imaging, phase-contrast or quantitative MRI or pressure-wire guided measurements during angiogram performance,32 33 larger-scale studies are needed for the validation. With the many promising applications of the CFD approach in stroke and ICAS research, validation of the modelling methodology and findings would be a prerequisite for its ultimate application in clinical practice to guide prognostication, clinical decisions and treatment in patients with stroke and ICAS, as it is in the cardiology field.
In sICAS, the stenosis rate has been used to scale the lesion severity, which is insufficient for risk stratification of affected patients.34 Previous studies have indicated that the anatomical severity of sICAS does not always translate to a similar haemodynamic significance when anatomically ‘moderate’ stenosis could be haemodynamically significant.35 Moreover, various factors, such as the haemodynamic impact, plaque morphology and stability, collateral and perfusion status and their intercorrelations, may also influence the stroke mechanisms and recurrent risks in patients with sICAS. Some of these could be investigated using CFD technique. For instance, in preliminary investigations, focal haemodynamics quantified in CFD models were associated with positive remodelling of intracranial plaques.16 Studies are warranted to further uncover the interrelationships between focal haemodynamics and plaque morphology/components, which could enhance the understanding of the pathophysiology of atherosclerosis and vascular remodelling process. Coupling HRMRI with the CFD technique can help from this perspective. On the other hand, the collateral circulation plays a crucial role in maintaining cerebral perfusion and hence affecting subsequent stroke risk in patients with sICAS, but the mechanism of collateral recruiting is far from being elucidated.36 Using the CFD technique, a preliminary study has provided evidence supporting the translesional pressure gradient as a driving force for the presence of good collaterals in patients with sICAS.17 Yet, this was a cross-sectional study that cannot establish the causal relationships or reveal the dynamic evolution of the sICAS lesion and the collateral status, which needs to be followed up with serial evaluation for collateral status.
In recent years, with more effective medical treatment and possibly better patient compliance, the risk of recurrent stroke of patients with sICAS have significantly declined. Yet, up to 10% of patients with sICAS could have a stroke recurrence after 1 year.4 7 As mentioned above, the haemodynamic metrics of sICAS derived from CFD models may be promising indicators for risk stratification of affected patients, supported by the SOpHIA study and other relevant studies. For instance, the SOpHIA study revealed higher stroke relapse risk in patients with sICAS with low PR (large translesional pressure gradient) and high WSSR (significantly increased WSS around lesions).7 Hypoperfusion and artery-to-artery embolism, which have been associated with excessively high risk of recurrent stroke in a previous study,20 could be the potential mechanisms for stroke recurrence related with low PR and high WSSR.
In addition, the CFD method may also be a promising tool in investigating the target for BP control in secondary stroke prevention in patients with sICAS. The latest guidelines recommend a BP <140/90 mm Hg for secondary stroke prevention in sICAS.37 However, this BP target was determined following the treatment regimen in the Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis trial,3 which was not tested against other BP targets in randomised controlled trials. Previous studies indicated that long-term, stringently controlled BP may increase the risk of recurrent stroke in patients with sICAS with hypoperfusion, when low BP levels could further aggravate the reduced cerebral perfusion.38 39 A CFD study echoed such findings that the altered relationship between SBP during follow-up and recurrent stroke risk in patients with sICAS could be attributed to the change in translesional PR.26 SBP level maintained below 130 mm Hg was correlated with a minimal risk of recurrent stroke in patients with normal PR, which, however, was associated with an increased risk of recurrent stroke in patients with low PR (hence possibly reduced perfusion). This could be explained by the impaired cerebral autoregulation in patients with sICAS, when the cerebral perfusion could be passively affected by systemic BP changes.40 Yet, these were retrospective, small-scale studies, which need further validation.
Moreover, CFD may also help in guiding stenting treatment in sICAS. Angioplasty +/- stenting is not recommended by the latest guidelines as a first-line treatment for patients with sICAS.41 Yet, stenting may be effective in certain subgroups of patients with sICAS. First, the CFD technique allows blood flow simulations with different vascular and stent geometry, which may help plan stenting treatment. For example, a small-scale study indicated that the stent shape may affect focal WSS and low-density lipoprotein filtration rate in sICAS,42 which study, however, was not included in this review because of the small sample size (<10). Second, the CFD technique may help assess the effects of stenting on focal haemodynamics in patients with sICAS, according to some preliminary studies as mentioned above.28 29 Yet, it is largely unknown regarding the associations of prestenting and poststenting haemodynamics with imaging and clinical outcomes in such patients, for example, in-stent restenosis and stroke recurrence, which need further investigations. In addition, studies are needed to investigate the value of CFD-based PR in identifying ischemia-causing sICAS lesions, who may truly benefit from stenting treatment, as what is being done for coronary artery lesions.43
This systematic review has some limitations. First, we did not conduct a meta-analysis of the haemodynamic parameters and associations of interest. This again reflects a major limitation of the existing CFD studies, with heterogenous CFD modelling methods, various haemodynamic metrics and research questions investigated, and usually small sample sizes, which has hindered comparisons or synthesis of findings from different studies. Second, multiple imaging methods can be used to assess or quantify haemodynamic features of sICAS, for example, vascular ultrasound, contrast-dependent or contrast-independent perfusion imaging, phase-contrast or quantitative MRI, or invasive measurements with pressure wire,44 which were not discussed or compared against the CFD approach in this systematic review. However, this is not within the focus of this systematic review. Third, all studies included in this review article were conducted in China. Although there were CFD studies on sICAS conducted in other areas of the world, they did not meet the sample size criterion or did not report the clinical relevance of the findings by the inclusion criteria and objectives of this study. This also reflects the greater interest in ICAS research in Asian populations, with a higher ICAS prevalence than that in Western populations. Yet, on the other hand, this could cause selection bias; hence, the study findings should be corroborated in different populations. Last but not least, most of the primary studies included in this systematic review investigated anterior-circulation sICAS, or mixed anterior-circulation and posterior-circulation lesions, while data were scarce for posterior-circulation sICAS separately.
Conclusions
This study systematically reviewed the methods and findings of studies investigating the clinical relevance of haemodynamic parameters obtained with CFD models in patients with sICAS. By simulating blood flow, the CFD technique is a promising tool in investigating the pathophysiology of ICAS and in risk stratification of patients with sICAS. However, there are also limitations and challenges with the current CFD models. Standardisation of the modelling methods and validation of the simulation results in sICAS are needed, for wider applications of this technique in clinical research and practice.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors YL, SL and XL contributed to the concept of the manuscript. YL and SL screened the articles and assessed the risk of bias of the included studies. YL and XL examined the full text and extracted the eligible studies. YL and XL drafted the manuscript. All authors have read and approved the final manuscript.
Funding This study was supported by General Research Fund (Ref No. 14106019), Early Career Scheme (Ref No. 24103122), Research Grants Council of Hong Kong; Health and Medical Research Fund (Reference No. 10210366), Hong Kong Food and Health Bureau; and Li Ka Shing Institute of Health Sciences.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}