

Abstract
Background and purpose The association between blood pressure variability (BPV) and stroke recurrence among patients who had ischaemic stroke (IS) remains unclear. This study aimed to investigate the association between BPV and stroke recurrence in patients who had IS of large artery atherosclerosis (LAA) subtype and small artery occlusion (SAO) subtype.
Methods Data from the BOSS (Blood Pressure and Clinical Outcome in Transient Ischemic Attack or Ischemic Stroke) study were examined. IS subtypes were diagnosed according to the Trial of Org 10172 in Acute Stroke Treatment criteria. BPV was performed by 24-hour ambulatory blood pressure monitoring and defined through SD of blood pressure. The primary outcome was stroke recurrence within 90 days after discharge. Multivariable Cox regression model was used to assess the association between BPV and stroke recurrence in patients who had IS of LAA subtype and SAO subtype.
Results A total of 1390 patients who had IS from the BOSS study were included in the present study. Multivariable analysis suggests that 24-hour systolic BPV (SBPV) and night-time diastolic BPV (DBPV) were significantly associated with stroke recurrence among all patients who had IS (HR, 2.50, 95% CI 1.07 to 5.84; HR, 1.85, 95% CI 1.07 to 3.21, respectively). Night-time SBPV and night-time DBPV were significantly associated with stroke recurrence in patients with SAO subtype (HR, 2.77, 95% CI 1.07 to 7.15; HR, 3.60, 95% CI 1.39 to 9.29, respectively). However, in the adjusted model, only night-time DBPV remained significant in patients with SAO subtype (HR, 3.87, 95% CI 1.40 to 10.71). Similar results were not found in patients who had IS of LAA subtype.
Conclusions High night-time DBPV was associated with increased risk of stroke recurrence among patients who had IS of SAO subtype. The results of this study have implications for the secondary prevention management and future research of patients who had IS of SAO subtype. The association between BPV and stroke recurrence in patients who had IS of LAA subtype and SAO subtype should be investigated in larger, population-based studies.
Introduction
Large artery atherosclerosis (LAA) and small artery occlusion (SAO) are the main aetiological subtypes of ischaemic stroke (IS) according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification.1 The incidence rate and recurrence rate of stroke are both high in the two subtypes,2 but much higher in the LAA subtype.3 Hypertension is an independent risk factor for incidence of stroke and possibly a potential risk factor for recurrence of stroke among patients who had IS. Previous studies showed that high blood pressure (BP) was associated with stroke recurrence in patients with SAO subtype rather than LAA subtype or other subtypes,4 and suggested that the high BP might have different effects on the pathogenesis of large artery and small artery diseases.
Most studies used mean BP as the index factor to predict the incidence or recurrence rate of stroke.5 However, BP shows noticeable fluctuation over the short and long term, and mean BP may not be able to reflect the stability of BP.6 Although blood pressure variability (BPV) was historically viewed as a phenomenon that could affect the accuracy of mean BP, it has been increasingly recognised as a potential risk factor for future strokes and coronary events in recent decades, the predictive capacity of which showed even better than the mean BP.7–15
The aim of the present study was to investigate the association between BPV and stroke recurrence in patients who had IS of LAA subtype and SAO subtype. We hope to find the different effects of BPV on stroke recurrence in patients with LAA subtype and SAO subtype and to provide implications for targeted management of BP for patients who had IS with large artery and small artery diseases.
Methods
Study population
The BOSS (Blood Pressure and Clinical Outcome in Transient Ischemic Attack or Ischemic Stroke) study was a hospital-based, prospective cohort study designed to assess the association between BP parameters and clinical outcomes of IS and transient ischaemic attack (TIA). It was conducted in 61 mainly tertiary urban hospitals from 16 provinces and 4 municipalities evenly distributed across the mainland of China. A total of 2608 patients who had IS and patients with TIA (≥18 years) were enrolled consecutively in this registry within 7 days after index events. The methods and the main results have been published previously.16 The present study was a post-hoc analysis of the BOSS study. In the current study, we included participants in the BOSS study who were diagnosed with IS according to the WHO criteria17 and were successfully classified as LAA subtype or SAO subtype according to the TOAST criteria.1
Written informed consent was obtained from all patients or their legal proxies before participation.
Ambulatory blood pressure monitoring and BPV
A 24-hour ambulatory blood pressure monitoring (ABPM) was performed within 3–14 days after the index events. Measurements were taken every 15 min during the day (06:00–21:59) and every 30 min at night (22:00–05:59). Patients could take normal daily activities during daytime and go to bed and wake up at the prescribed time. BP recorded readings exceeding 75% of the expected measurements were considered for analysis according to the European Society of Hypertension guideline.18
Daytime BPV and night-time BPV were calculated through SD of the daytime and night-time periods. The 24-hour BPV was identified by weighted 24-hour SD (w24hSD) according to the following formula19 20:

where 16 and 8 were the number of hours included in the daytime and night-time subperiods, respectively.
Classification of stroke subtypes
All patients diagnosed with IS were further classified according to the TOAST criteria.2 The specific standards and methods of classification were performed as described previously.4 21 Subtype classification was based on the patient’s clinical features and was combined with at least one diagnostic test, including brain imaging examination (CT or MRI), imaging of intracranial arteries (magnetic resonance angiography) and extracranial arteries (carotid ultrasonography or CT angiography), as well as laboratory tests for the diagnosis of prethrombotic state. All patients’ clinical features and results of diagnostic tests were reviewed by at least two trained neurologists from each participating hospital, who finally made the decision on the subtype classification.
Covariables
Clinical information was collected by trained investigators or research coordinators at enrolment and follow-up visits. Risk factors for stroke such as medical history (including IS, TIA, myocardial infarction, congestive heart failure, known atrial fibrillation or flutter, hypertension, diabetes mellitus and dyslipidaemia) and lifestyle (including smoking and drinking) were recorded on admission. The presence of IS, TIA, myocardial infarction and congestive heart failure was defined as a medical chart-confirmed history. The presence of hypertension, diabetes mellitus and dyslipidaemia was defined as self-reported disease history or a patient who was on antihypertensive, antidiabetic or lipid-lowering medication. Atrial fibrillation or flutter was defined as a reported history of atrial fibrillation or flutter, or diagnosed by the in-hospital ECG. Current smoker was defined as those who reported smoking at the index of the event. Former smoker was defined as those who quitted smoking within 1 year. Moderate or heavy drinking was defined as consuming at least two standard alcoholic beverages per day. The severity of stroke was assessed using National Institutes of Health Stroke Scale score on admission. Secondary prevention medications (including antiplatelet, antihypertensive, antidiabetic and lipid-lowering treatments) were recorded during hospitalisation.
Clinical outcome
The primary outcome of this study was stroke recurrence within 90 days after discharge. Stroke recurrence was defined as a new stroke (including IS and haemorrhagic stroke) after the index event.22 The new clinical manifestations were not due to oedema, haemorrhagic transformation or other intracranial complications. The new symptoms should last more than 24 hours and there was evidence of a new stroke on MRI or CT brain imaging. At 90-day follow-up after discharge, patients were asked whether they had experienced hospital readmission due to the new symptoms. Hospitals admitting patients with recurrent stroke were connected to verify the diagnosis.
Statistical analysis
In this study, the SD of BP was considered a categorical variable and the optimal cut-off value was identified through 90-day receiver operating curve analysis.9 High BPV (HBPV) was defined as those whose SD of BP was higher than the optimal cut-off values. Patients enrolled in this study were divided into two groups according to the status of HBPV (with and without HBPV). Each group was then stratified by TOAST subtypes. For descriptive analysis, categorical variables were described by frequencies and percentages, and continuous variables were described by mean with SD. For baseline characteristics, χ2 test was used for categorical variables and Kruskal-Wallis test was used for continuous variables to compare the differences between patients with LAA subtype and SAO subtype. χ2 test and multivariable Cox regression model were used to investigate the association between BPV and risk of stroke recurrence, stratified by LAA subtype and SAO subtype. The Cox model was adjusted for potential confounders including age, gender, severity of stroke, history of TIA, lifestyle (including smoking and drinking) and corresponding average BP. These confounders were significant in the univariate analysis between confounders and recurrent stroke events (online supplemental file), or were potential confounders of stroke recurrence according to previous studies.23 The proportional hazards assumption was assessed by testing the interaction between BPV and time. Unadjusted and adjusted HRs with 95% CIs were both reported. A two-tailed probability value of <0.05 was considered significant in the univariate and multivariable analyses. Analyses of this study used SAS V.9.4.
Supplementary data
Results
Baseline characteristics
Of 2608 patients enrolled in the BOSS study, 840 who recorded less than 75% of the expected measurements of ABPM were excluded. Another 378 patients were also excluded, including 290 patients diagnosed with TIA, 18 patients who had IS who failed to be classified by TOAST subtypes and 70 patients classified as cardiogenic embolism subtype or others. Finally, a total of 1390 patients who had IS were included in the present analysis, including 860 patients with LAA subtype and 530 patients with SAO subtype. The mean number of ABPM was 71.1±9.9 for 24 hours, 55.3±10.5 for daytime and 15.8±5.7 for night-time. The baseline characteristics of the included patients are presented in table 1 according to TOAST subtypes. Patients with SAO subtype were a little younger than those with LAA subtype. Besides, the rate of hypertension was higher in patients with LAA subtype than those with SAO subtype.
Baseline characteristics of patients with different TOAST subtypes
Association between BPV and stroke recurrence in patients who had IS of LAA subtype and SAO subtype
The optimal cut-off values calculated through SD were used to separate patients with and without HBPV. For systolic BP, the optimal cut-off values for 24 hours, night-time and daytime were 12.5 mm Hg, 14.5 mm Hg and 16.5 mm Hg. For diastolic BP, the corresponding values were 14.0 mm Hg, 11.5 mm Hg and 7.5 mm Hg. The rate of stroke recurrence in all patients was 3.8%, in patients with LAA subtype was 4.1% and in patients with SAO subtype was 3.4%.
Table 2 shows the results of the univariate analysis on the association between BPV and stroke recurrence in patients who had IS of LAA subtype and SAO subtype. For all patients, the rates of stroke recurrence were different between patients with and without high 24-hour systolic BPV (SBPV) and night-time diastolic BPV (DBPV) (p=0.02 and p=0.02, respectively). After stratification by TOAST subtypes, the rates of stroke recurrence in patients with high night-time SBPV and night-time DBPV were significantly higher than those without corresponding HBPV in SAO subtype (p=0.02 and p=0.002, respectively). Similar results were not found in patients with LAA subtype.
Comparison of stroke recurrence rates in patients who had IS with and without HBPV, stratified by TOAST subtypes
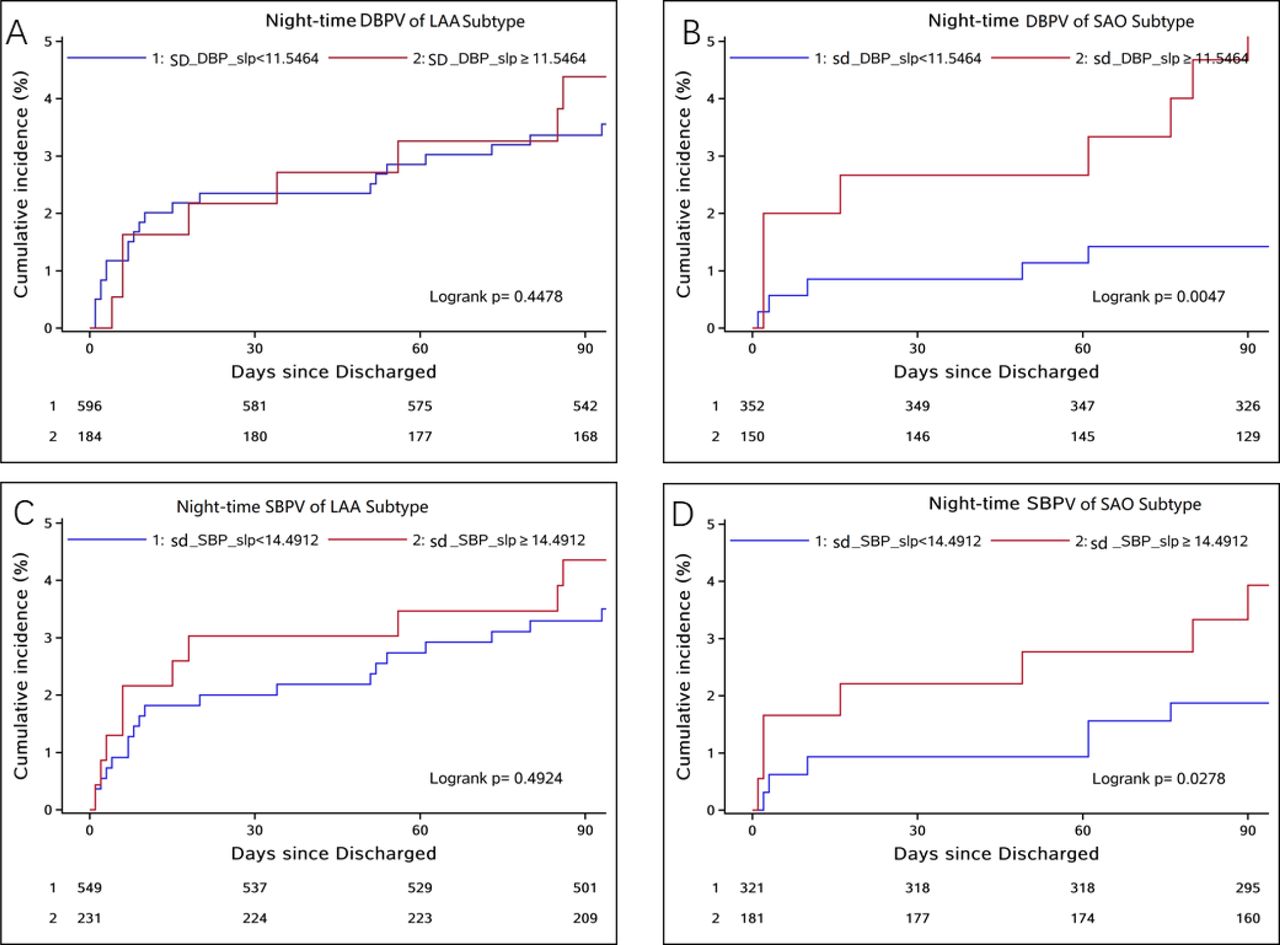
At the same time, we used multivariable Cox regression model to investigate the association between BPV and stroke recurrence in patients with LAA subtype and SAO subtype, in which BPV was entered as a dichotomous variable. For all patients, the high 24-hour SBPV and high night-time DBPV showed significant trends of association with increased risk of stroke recurrence (HR, 2.50, 95% CI 1.07 to 5.84, p=0.03; HR, 1.85, 95% CI 1.07 to 3.21, p=0.03, respectively). However, after stratification by TOAST subtypes, the association between BPV and stroke recurrence was only found during night-time, and the association was only found in patients with SAO subtype (for SBPV: HR, 2.77, 95% CI 1.07 to 7.15, p=0.04; for DBPV: HR, 3.60, 95% CI 1.39 to 9.29, p=0.008). After adjusting for potential confounders, including age, gender, severity of stroke, history of TIA, lifestyle (including smoking and drinking) and corresponding average BP, only in patients with SAO subtype was BPV associated with stroke recurrence and only night-time DBPV remained associated with stroke recurrence (HR, 3.87, 95% CI 1.40 to 10.71, p=0.01). The above data suggest that when DBPV was high at night (SD of night-time DBP >11.5 mm Hg), the risk of stroke recurrence might increase by 287% in patients with SAO subtype. However, similar results were not found in patients with LAA subtype. Unadjusted and adjusted HRs with 95% CIs are listed in table 3. Figure 1 shows the Kaplan-Meier curves of the association between night-time BPV and risk of stroke recurrence among patients who had IS of SAO subtype and LAA subtype.
Association between BPV and stroke recurrence in patients who had IS, stratified by TOAST subtypes

Relations between night-time BPV and risk of stroke recurrence among patients who had IS of SAO subtype and LAA subtype. (A) High night-time DBPV of LAA subtype was not related to increased risk of stroke recurrence. (B) High night-time DBPV of SAO subtype was significantly related to increased risk of stroke recurrence. (C) High night-time SBPV of LAA subtype was not related to increased risk of stroke recurrence. (D) High night-time SBPV of SAO subtype was significantly related to increased risk of stroke recurrence before adjusting for corresponding confounders and potential risk factors. BPV, blood pressure variability; DBP, diastolic blood pressure; DBPV, diastolic blood pressure variability; IS, ischaemic stroke; LAA, large artery atherosclerosis; SAO, small artery occlusion; SBP, systolic blood pressure; SBPV, systolic blood pressure variability.
Discussion
In the present study, we found that 24-hour SBPV and night-time DBPV were associated with stroke recurrence in all patients who had IS. Night-time SBPV and night-time DBPV were associated with stroke recurrence in patients who had IS of SAO subtype. However, after adjusting for several traditional risk factors and potential confounders, only night-time DBPV was found to be associated with stroke recurrence in patients who had IS of SAO subtype. The results of this study suggest that high night-time DBPV assessed through 24-hour ABPM might be a predictor of a recurrent stroke in patients who had IS of SAO subtype.
Comparison with other studies
Several prospective studies including populations and patients with hypertension or diabetes have searched for the association between BPV and stroke outcomes but reported inconsistent results.24–29 The post-hoc analysis of the Syst-Eur (Systolic hypertension in Europe) trial found that only increased night-time SBPV was an independent risk factor for stroke incidence in an elderly population with hypertension.24 However, the results of the PIUMA (Progetto Ipertensione Umbria Monitoraggio Ambulatoriale) study found that the rate of cerebrovascular events was higher in patients with hypertension with increased SBPV or DBPV during daytime or night-time than in those with low BPV.25 However, a meta-analysis of individual data from the IDACO (International Database of Ambulatory Blood Pressure in relation to Cardiovascular Outcome) study, which included >8000 people randomly recruited from 11 populations and covered on average 11 years of follow-up, suggested that 24-hour SBPV and 24-hour DBPV were associated with a fatal or non-fatal stroke; similar results were not found for daytime or night-time BPV.28 These studies included different subjects with or without treatment and there were various BPV devices used, which limited the interpretation of the results. In addition, in these studies, no results were provided for risk of stroke recurrence in patients who had IS. To assess the association between BPV and risk of stroke recurrence, we used 24-hour ABPM to measure BPV in patients who had IS and finally found that high night-time DBPV was associated with increased risk of stroke recurrence among patients who had IS of SAO subtype, which might be a novel finding. The results of the study suggested that night-time DBPV might play an important role in the prognosis of small artery diseases.
Potential mechanisms
Several possible reasons had been presented in previous studies to explain why BPV during night was more predictive than daytime BPV; for example, nocturnal monitoring could exclude the external interference and avoid the persistent hyperactivity of sympathetic nerve system. The underlying mechanisms whereby BPV is related to stroke recurrence in SAO subtype are largely unknown. Reasonable explanations can only be speculated. HBPV represents increased fluctuation of blood flow, which could dampen smooth blood flow to small arteries, resulting in less perfusion of the arterioles.30 31 At the same time, increased BPV could inhibit nitric oxide production, which might impair endothelial function and damage the blood–brain barrier as well as the ‘neurovascular unit’.32 33 For small vessels which had already been damaged, the above potential mechanisms could further destroy their structure and function, which could result in the dysfunction of autoregulation of cerebral blood flow and thereby increase the risk of a recurrent stroke.34 For example, when BP is below the lower threshold of cerebral blood flow autoregulation, hypotension would happen and result in IS. Inversely, when BP exceeds the upper threshold, hypertension would lead to haemorrhagic stroke. Heart is perfused during diastole. Meanwhile, high DBPV might influence the ventricular end diastolic volume, which could lead to extreme cerebral perfusion, especially in patients with destroyed autoregulation of cerebral blood flow.
Strengths and limitations
To our knowledge, this is the first study to investigate the association between BPV and stroke recurrence in patients who had IS of different TOAST subtypes. We found that high night-time DBPV was associated with increased risk of stroke recurrence in patients who had IS of SAO subtype. Moreover, we collected detailed clinical features at enrolment so that we could realise to account for several potential confounders. However, there were several limitations to our study. First, the sample size was relatively small in each TOAST subtype, which was responsible for the lower statistical power in this study. Second, the ABPM devices were not unified among all participating hospitals. Although internal monitoring, duration, qualified recording numbers and other parameters required were the same, the quality of monitoring was not guaranteed, which might have influenced the analysis of data. Third, we used SD to calculate BPV in our study. Other metrics used to calculate BPV, such as average real variability or successive variation, were also demonstrated to be effective in predicting the outcomes. However, these measures were complicated and the correlation coefficients were more than 0.83.35 In contrast, SD is easier to obtain and more practical and we believe it will have greater value in clinical application. Fourth, although we have accounted for the most important potential confounders in our study, we could not exclude unknown and residual confounding factors cannot be completely excluded as explanations for the results.
Conclusions
High night-time DBPV calculated through 24-hour ABPM was associated with increased risk of stroke recurrence among patients who had IS of SAO subtype. This association was independent of average night-time DBP. The results of this study suggest that, compared with SBPV, night-time DBPV might play a more important role in the prognosis of small artery diseases. The secondary prevention of patients who had IS of SAO subtype might pay more attention to the management of night-time DBPV. The association between BPV and stroke recurrence in patients who had IS with large artery and small artery diseases should be investigated in larger, population-based studies.
Data availability statement
Data are available upon reasonable request. The corresponding author is responsible for the data in this study. Anyone wishing to access the data has to obtain the consent of the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the central institutional review boards of Beijing Tiantan Hospital. Written informed consent was obtained from all patients or their legal proxies before participation. The ethics approval number was KYSB2017-084-01.
Footnotes
Contributors TW: study concept and design, analysis and interpretation of data, drafting of the manuscript. JX: analysis and interpretation of data, drafting of the manuscript. AW: analysis and interpretation of data. YL: revision of the manuscript. XZ: study concept and design, study supervision. YoW: study concept and design, obtaining funding, study supervision. YiW: study concept and design, study supervision, analysis and interpretation of data, clinical revision of the manuscript for intellectual content.
Funding The study was funded by grants from the National Key R&D Program of China (no. 2018YFC1312400, 2018YFC1312402), the Ministry of Science and Technology of the Beijing Outstanding Young Scientist Program (BJJWZYJH01201910025030), the National Natural Science Foundation of China (no. 81825007), the 'Thirteenth-Five' Key Development and Research Plan by the Ministry of Science and Technology of the People’s Republic of China (no. 2017YFC1307900), and Supporting-Top Youth Team by Beijing Municipal Science and Technology Commission (no. 2016000021223TD03).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References




{kind=link}