

Abstract
Background and purpose To date, no large cohort study has investigated the effects of intravenous thrombolysis (IVT) in Chinese patients aged over 80 years who had a stroke. This study aimed to assess the trends in the use of alteplase, the clinical characteristics and the outcomes of Chinese patients aged above 80 years who had an acute ischaemic stroke.
Methods Data for this analysis were obtained from the China Stroke Center Alliance programme, a nationwide, multicentre, prospective registry encompassing 1751 hospitals across 31 provinces, covering the period from 1 January 2018 to 14 December 2022. The primary outcome was defined as a modified Rankin Scale (mRS) Score of 0–2 at discharge. Secondary outcomes included an mRS Score of 0–1 and independent ambulation on discharge. Safety outcomes assessed were in-hospital mortality and symptomatic intracranial haemorrhage (sICH).
Results Out of 30 902 patients over 80 years old who qualified for thrombolysis, 8673 (median age (IQR), 84 (82–87) years) received alteplase treatment. Patients administered alteplase demonstrated improved short-term functional outcomes, such as an mRS Score of 0–2 (adjusted OR (aOR) 1.12, 95% CI, 1.06 to 1.18, p<0.001), an mRS Score of 0–1 (aOR 1.14, 95% CI, 1.08 to 1.19, p<0.001) and independent ambulation at discharge (aOR 1.14, 95% CI, 1.08 to 1.20, p<0.001). Moreover, no significant increase was observed in the risk of in-hospital mortality (aOR 1.12, 95% CI, 0.93 to 1.35; p=0.23). However, the risk of sICH was significantly higher among patients treated with alteplase (aOR 3.22, 95% CI, 2.77 to 3.75; p<0.001).
Conclusions IVT with alteplase in elderly patients who had a stroke resulted in improved short-term functional outcomes without elevating the risk of in-hospital mortality. Nonetheless, this population remains at a higher risk of sICH.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Currently, neither China nor the USA imposes an upper age limit for administering intravenous thrombolysis (IVT) to patients who had an ischaemic stroke. However, the Chinese Food and Drug Administration continues to restrict the use of alteplase for those over 80 years old. Furthermore, no large-scale cohort studies have evaluated the application of IVT in Chinese patients above the age of 80 in real-world clinical settings.
WHAT THIS STUDY ADDS
This nationwide cohort study of patients over 80 years who had an ischaemic stroke reveals that the use of IVT rose by 13.6% between 2018 and 2022. Elderly patients who received alteplase therapy showed improved functional outcomes at discharge compared with those who did not, without experiencing a higher rate of in-hospital mortality.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The results of this study provide stronger evidence supporting the application of alteplase in patients over 80 years who had a stroke, potentially influencing future research, clinical practices and policy guidelines.
Introduction
Stroke remains the leading cause of mortality in China,1–3 with the nation having the highest lifetime stroke risk among individuals aged 25 years and older.4 Despite the Chinese government’s efforts to implement comprehensive stroke prevention strategies, stroke prevalence continues to rise alongside population growth.3 5 Additionally, stroke incidence increases with age. In 2019, the prevalence of ischaemic stroke was 6.58% among individuals aged 65–69 years, while in those aged 80 and above, the prevalence was notably higher at 12.81%.6 Acute ischaemic stroke in the elderly leads to more significant neurological deficits compared with younger individuals, resulting in higher rates of disability and mortality.7 With the rapidly ageing population in China, the number of individuals aged 80 years and older, which was 26 million in 2019, is expected to surge to 115 million by 2050.8 This demographic shift makes it crucial to address strategies for reducing disability in patients over 80 years who had a stroke.
Intravenous thrombolysis (IVT) with alteplase has been shown to be an effective treatment for acute ischaemic stroke, reducing disability by promoting reperfusion.9 10 However, its use in older patients has historically been limited due to concerns about age. In 2013 and 2014, the American Heart Association11 and the Chinese Academy of Neurology12 removed age>80 years as a contraindication for IVT within 3 hours of symptom onset. By 2018, the recommended time window for IVT was extended to 4.5 hours.13 14 As guidelines continue to evolve both domestically and internationally, a growing number of elderly patients are becoming eligible for IVT. Consequently, in the USA, IVT usage in elderly patients saw a significant increase from 2008 to 2009 to 2016–2017.15 However, there has yet to be a large cohort study examining the use of IVT in Chinese patients over 80 years old,16 17 and the trends in IVT use among this population remain underexplored. A thorough understanding of IVT use in elderly patients who had a stroke in China is essential for guiding healthcare providers and policymakers in optimising treatment strategies for this demographic.
The objective of this study was to analyse data from a nationwide registry to assess in-hospital outcomes in elderly patients who had a stroke who received IVT with alteplase and to evaluate trends in IVT treatment rates among patients older than 80 years compared with those 80 years or younger.
Methods
The China Stroke Center Alliance (CSCA) programme is a large-scale, nationwide, multicentre, voluntary and prospective registry designed to promote continuous quality improvement in the care of patients who had a stroke. The details of the programme’s design and data collection methods have been thoroughly documented in earlier studies.18 This initiative was open to both secondary and tertiary hospitals across China. Trained staff at each participating hospital collected data using a web-based patient management system developed by the Medicine Innovation Research Center. Data analysis was conducted by the China National Clinical Research Center for Neurological Diseases. Participating hospitals agreed to use anonymised data for research purposes and to assess the quality of care provided. Collected data at the time of admission included demographic factors (such as sex, age and body mass index (BMI)), as well as clinical risk factors, including smoking status, alcohol use, hypertension, diabetes, dyslipidaemia, myocardial infarction, peripheral arterial disease and history of stroke or transient ischaemic attack (TIA). Additionally, the National Institutes of Health Stroke Scale (NIHSS) Score, stroke severity, onset-to-door time (ODT), onset-to-treatment time, door-to-needle time, alteplase dosage, medical history, hospital classification (secondary or tertiary) and geographic region (eastern, central, or western China) were recorded.
Patient population
This study involved patients who had an ischaemic stroke treated at 1751 hospitals participating in the CSCA between 1 January 2018 and 14 December 2022. Eligibility was determined based on the occurrence of stroke symptoms within 4.5 hours and the absence of any absolute contraindications for thrombolysis, as outlined in the guidelines.11 Patients were excluded if they had undergone thrombectomy, received alternative thrombolytic agents, underwent intra-arterial thrombolysis or had incomplete data regarding NIHSS scores, prior modified Rankin Scale (mRS) scores, key time points (such as door-to-needle or onset-to-treatment time), alteplase dosage or in-hospital outcomes.
Patient and public involvement
No patient involved.
Outcome measurement
The primary outcome was the mRS, which scores from 0 (normal) to 6 (death), with an mRS Score of 0–2 at discharge. Secondary outcomes included achieving an mRS Score of 0–1 and the ability to walk independently on discharge. Safety measures encompassed in-hospital mortality and symptomatic intracranial haemorrhage (sICH), following the National Institute of Neurological Disorders and Stroke criteria, which defines sICH as any parenchymal haemorrhage detected via CT or MRI, accompanied by clinical deterioration within 36 hours of treatment initiation.9 To assess treatment effects in elderly patients with ischaemic stroke, predefined subgroups based on sex, NIHSS-classified stroke severity (ranging from mild (0–4), moderate,5–15 moderate to severe16–20 to severe (>20)), prior stroke or TIA, diabetes and atrial fibrillation were analysed. Additionally, outcomes were stratified into three categories based on the ODT: group 1 (ODT≤2 hours), group 2 (2–3.5 hours) and group 3 (ODT>3.5 hours).
Statistical analysis
Continuous variables were expressed as medians, while categorical variables were summarised using frequencies and percentages. Logistic regression models were applied to evaluate in-hospital outcomes among elderly patients who received alteplase compared with those who did not. To address baseline differences between the two groups, inverse probability weighting (IPTW) was employed to generate propensity scores.19 20 Sensitivity analyses were conducted using 1:1 propensity score matching to assess the robustness of thrombolysis outcomes. A calliper width of 0.2 SD was used, ensuring that standardised differences were maintained below 0.1 for balance. The models were adjusted for several covariates, including sex, age, hospital type, BMI, relevant risk factors (such as prior stroke or TIA, and atrial fibrillation) and medical history (use of antiplatelet agents and statins). For in-hospital outcomes stratified by ODT, multivariable logistic regression models were used, adjusting for statistically significant covariates in each group.
Subgroup analyses were performed to evaluate the interaction effects of treatment on primary outcomes across specific patient subgroups using multivariable logistic regression. The impact of prior anticoagulant or antithrombotic therapy on hospital outcomes in patients over 80 years of age receiving thrombolytic therapy was also examined. Previous antithrombotic therapy refers to taking one or more antithrombotic agents continuously for at least 2 weeks within the 6 months before the condition started.
Temporal trends in IVT use from 2018 to 2022 were evaluated through Cochran-Armitage trend tests.
Outcome variables with missing data were excluded from the analysis. Sensitivity analyses were performed to compare baseline characteristics between populations with and without missing data.
Two-sided p values of less than 0.05 were deemed statistically significant. Given the large sample size, small differences might have reached statistical significance without clinical relevance, prompting the calculation of absolute standardised differences (ASDs). An ASD greater than 10% was considered indicative of significant imbalance.21 22 All statistical analyses were conducted using SAS V.9.4.
Results
Baseline characteristics
After excluding ineligible cases, the study included 212 814 patients who had an ischaemic stroke from 1751 hospitals between 1 January 2018 and 14 December 2022. Among these, 30 902 patients were aged over 80 years, with 8673 receiving alteplase treatment and 22 229 not receiving it (figure 1 and online supplemental eTable 1). For patients over 80 years old (table 1), the median age of those treated with alteplase was 84 years (IQR, 82.0–87.0), with a higher proportion of women (52.7%, n=4570). The median door-to-needle time was 44.2 min (IQR, 29.0–65.0 min). Compared with those not treated with alteplase, patients who received the treatment had more severe strokes (median NIHSS Score 9 vs 5, ASD=60.0%), a lower BMI (median 21.7 (IQR, 19.2–24.2) vs 22.8 (IQR, 20.8–24.8), ASD=29.1%), a higher prevalence of atrial fibrillation (20.7% vs 15.8%, ASD=12.9%), a lower history of stroke or TIA (27.0% vs 37.5%, ASD=22.6%), shorter ODTs (median 1.5 hours (IQR, 0.9–2.2) vs 1.9 hours (IQR, 1.0–3.0), ASD=29.7%) and lower usage rates of antiplatelet agents (17.9% vs 24.2%, ASD=14.6%) and statins (15.4% vs 21.0%, ASD=14.2%). After adjustment via propensity score matching, baseline characteristics between the two groups achieved balance, except for baseline NIHSS and pre-stroke mRS 0–2 (online supplemental eTable 2).
Supplementary data

Flowchart for patient selection. BMI, body mass index; CSCA, China Stroke Center Alliance; EVT, endovascular thrombectomy; IVT, intravenous thrombolysis; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; sICH, symptomatic intracranial haemorrhage; tPA tissue-type plasminogen activator.
Baseline characteristics of patients aged>80 years according to assigned treatment
The main reason for not administering alteplase thrombolysis was exceeding the 4.5-hour thrombolysis window for treatment (11 765 of the 22 299 patients, 52.9%, online supplemental eTable 3). Other reasons included patients or family members declining the recommendation (7091 of the 22 299 patients, 31.9%), hospital-related and other factors (208 of the 22 299 patients, 0.9%), economic reasons such as intravenous tissue-type plasminogen activator not being covered by health insurance (183 of the 22 299 patients, 0.9%) and unknown reasons (2992 of the 22 299 patients, 13.5%).
Patients with missing outcome data were excluded from the final analysis. Sensitivity analyses indicated no significant baseline differences between patients with and without missing data (online supplemental eTable 4).
In-hospital outcomes for elderly patients
A detailed comparison of outcome measures is shown in table 2. After adjusting for covariates using IPTW scores, elderly patients treated with alteplase had significantly better functional outcomes at discharge. Specifically, a higher proportion of patients achieved an mRS Score of 0–2 (55.5%, n=4815; adjusted OR (aOR) 1.12, 95% CI, 1.06 to 1.18, p<0.001), an mRS Score of 0–1 (43.3%, n=3743; aOR 1.14, 95% CI, 1.08 to 1.19, p<0.001) and independent ambulation (65.0%, n=5640; aOR 1.14, 95% CI, 1.08 to 1.20, p<0.001). However, patients treated with alteplase exhibited higher rates of sICH compared with those not treated (4.9% (n=423) vs 1.2% (n=273); aOR 3.22, 95% CI, 2.77 to 3.75, p<0.001). The incidence of in-hospital mortality was similar between the two groups (2.3% vs 1.3%, aOR 1.12, 95% CI, 0.93 to 1.35, p=0.23). Sensitivity analysis using propensity score matching yielded consistent results (table 2).
Comparison of in-hospital outcomes in patients aged>80 years for stroke with or without alteplase treatment
After adjusting for the statistically significant variables listed in online supplemental eTable 5 using a multivariate regression model, the results for in-hospital outcomes stratified by ODT are shown in online supplemental eTable 6. Compared with untreated patients, each treatment group had a better adjusted primary outcome (group 1, p<0.001; group 2, p<0.001; group 3, p=0.002) and independent ambulation (group 1, p<0.001; group 2, p<0.0001; group 3, p=0.0043). Otherwise, there was no difference in mRS 0–1 between patients treated with alteplase and those who were not (143 (39.8%) vs 1865 (48.3)], aOR 1.15, 95% CI, 0.89 to 1.49, p=0.291) in group 3 (ODT>3.5 hours). Patients who were treated with alteplase were more likely to have sICH regardless of ODT (group 1, p<0.001; group 2, p<0.001; group 3, p<0.001). There was no significant difference in in-hospital mortality rates between patients treated with alteplase and those who were not except for ODT≤2 hours in group 1 (2.8% vs 1.5%, aOR 1.32, 95% CI, 1.05 to 1.67, p<0.001).
Subgroup analysis
In the subgroup of patients with ischaemic stroke aged>90 years, thrombolysis with alteplase versus no alteplase demonstrated comparable treatment effects regarding the proportion achieving an mRS Score of 0–1 (aOR 1.19, 95% CI, 0.98 to 1.43, p=0.07), mRS Score of 0–2 (aOR 1.11, 95% CI, 0.93 to 1.34, p=0.236) and independent ambulation at discharge (aOR 1.04, 95% CI, 0.87 to 1.25, p=0.660). In contrast, the alteplase group showed a higher risk of haemorrhage (aOR 1.19, 95% CI, 1.78 to 5.37, p<0.001) without a significant difference in mortality in the hospital (aOR 1.30, 95% CI, 0.77 to 2.21, p=0.327) (online supplemental eTable 7).
As shown in figure 2, we performed exploratory subgroup analyses stratified by sex, stroke severity according to the NIHSS, previous stroke/TIA status, atrial fibrillation status and diabetes status by multivariate regression model. Overall, each characteristic tended to be associated with better functional outcomes with thrombolysis. However, there were interactions within three specific subgroups: atrial fibrillation, stroke severity, diabetes (p for interaction in each group<0.001). Patients with a history of atrial fibrillation (aOR 1.75, 95% CI, 1.51 to 2.03, p<0.001), moderate stroke (aOR 1.62, 95% CI, 1.49 to 1.76, p<0.001) or without diabetes (aOR 1.41, 95% CI, 1.35 to 1.51, p<0.001) benefitted more from thrombolysis.

Subgroup analysis of the primary outcome in patients older than 80 years according to assigned treatment. NIHSS, National Institutes of Health Stroke Scale; TIA, transient ischaemic attack.
Covariates were corrected for age, sex and all statistically significant variables listed in online supplemental eTable 8, except for BMI. As a result, the findings regarding the impact of prior antithrombotic therapy on thrombolysis, which are detailed in online supplemental eTable 9, were adjusted accordingly. In elderly patients undergoing thrombolysis, no significant differences in functional outcomes (mRS scores of 0–1 and 0–2, and independent ambulation at discharge) were observed when comparing individuals with a history of antithrombotic therapy, regardless of the type of prior antithrombotic therapy: antiplatelet alone, anticoagulant alone or a combination of both (p>0.05 for all groups). Additionally, prior antithrombotic therapy did not increase the incidence of sICH or in-hospital mortality following thrombolysis in patients (p>0.05 for all groups).
Temporal trends in IVT rates among potentially eligible patients
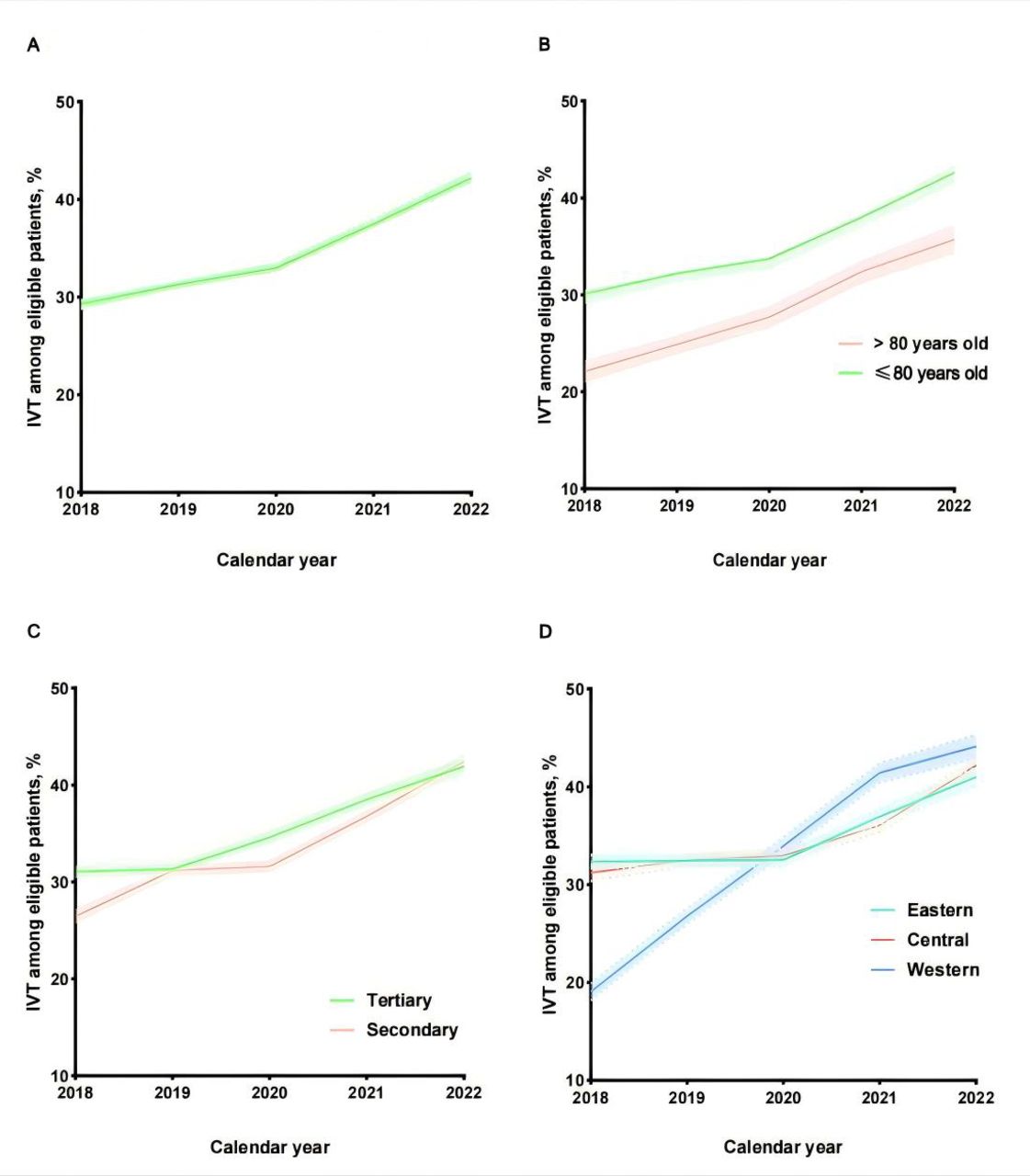
As demonstrated in figure 3, the rate of IVT increased over time in both age groups. For patients over 80 years old, IVT use rose from 22.1% in 2018 to 35.7% in 2022, while in younger patients, the increase was from 30.5% to 43.3% during the same period. The absolute growth rates were similar between the groups (13.6% vs 12.8%). Despite starting at a lower baseline, the older cohort exhibited a higher average annual percentage increase in IVT usage compared with younger patients (12.5% vs 9.1%). All groups exhibited an increasing trend in thrombolysis rates, regardless of their level of hospitalisation or geographical location. Tertiary hospitals had a lower absolute growth rate than secondary hospitals (tertiary vs secondary, 10.8% vs 12.6%). The thrombolysis rate increased most rapidly in hospitals in the western region (absolute growth of 25.0%), despite having the lowest initial rate (19.1% in 2018). Moreover, at the study endpoint, the thrombolysis rate was comparable between secondary and tertiary hospitals (42.4% vs 41.0% in 2022) and between the western and eastern regions (44.1% vs 41.0% in 2022).

Temporal trends in rates of intravenous thrombolysis (IVT) use among potentially eligible patients from 2018 to 2022. Use rate of IVT with alteplase in all patients (A); use rate of IVT with alteplase in patients aged>80 years and 80 years and younger (B); use rate of IVT with alteplase by hospital grade (C) and use rate of IVT with alteplase by hospital region (D). Shading represents 95% CIs.
Discussion
To date, there has been no extensive research focusing on IVT in Chinese patients over 80 years who had an ischaemic stroke. In this large cohort study, drawn from a nationwide stroke registry, we observed that alteplase treatment in patients over 80 years old led to improved functional outcomes at discharge when compared with those who did not receive alteplase, without an increase in in-hospital mortality, despite a higher risk of sICH. Few studies have directly evaluated the efficacy and safety of IVT in older populations. Our results align with findings from the Safe Implementation of Treatments in Stroke–International Stroke Thrombolysis Registry (SITS-ISTR) and the Virtual International Stroke Trials Archive (VISTA), the largest observational studies in this field. These studies included 29 500 patients who had an ischaemic stroke who presented within 3 hours of symptom onset, of which, 3472 (11.8%) were over 80 years old. Sensitivity analyses in those studies demonstrated that patients receiving alteplase had significantly better functional outcomes at 3 months.23 Specifically, the odds of achieving a mRS Score of 0–2 were 2.1 (95% CI, 1.7 to 2.5), and for an mRS of 0–1, the OR was 1.9 (95% CI, 1.5 to 2.3). Unlike those studies, our research examined patients treated within 4.5 hours of symptom onset and found that alteplase consistently resulted in better in-hospital outcomes across all ODT groups. These findings support the current Class IIA guidelines recommending thrombolytic therapy for elderly patients within the 3–4.5 hours of window, further reinforcing its use in patients over 80 years of age within 4.5 hours of symptom onset.
Our study found that 55.0% (n=4815) of elderly patients treated with alteplase had mRS scores of 0–2 at discharge, a significantly higher proportion than reported in the Baden-Wuerttemberg (BW) stroke registry. In the BW cohort, which involves patients aged 18 years and older who were treated within 7 days of symptom onset, the mRS 0–2 outcome was 32.0% for those aged 80–89 years (n=2849) and 17.0% for patients over 90 years (n=394).24 For patients with ischaemic stroke aged>90 years, our study shows that thrombolytic therapy does not improve functional outcomes. This finding aligns with the results of the SITS-ISTR and VISTA study. The analysis demonstrated no statistically significant difference in 90-day functional outcomes (mRS 0–2) between the thrombolysis group (n=133) and the non-thrombolysis group (n=77) among patients aged 90–100 years (OR 1.2, 95% CI, 0.69 to 2.0). Given our large sample size (thrombolysis: n=606 vs non-thrombolysis: n=2084), we recommend that thrombolytic therapy for patients over 90 years old in China be considered with caution.
Although thrombolytic therapy for acute ischaemic stroke is linked to an elevated risk of sICH shortly after treatment, our study showed that the incidence of sICH in elderly patients treated with alteplase was 3.22 times higher compared with untreated patients.25 26 However, the sICH rate of 5% in our study was still lower than those reported in earlier studies, where rates ranged from 6.7% to 17.5%.7 24 27 28 This lower rate may be explained by the fact that our patients had lower baseline NIHSS scores, which correlates with a reduced risk of sICH.24 In contrast, elderly patients treated with alteplase in randomised controlled trials (RCTs) had a higher average NIHSS Score (mean (SD): 13.3 (6.4))18 and several registry studies reported a median NIHSS of 14,7 24 29 potentially accounting for their higher sICH rates. Our study also indicated that IVT was not associated with an increase in short-term mortality among elderly patients who had a stroke, which is consistent with findings from individual analyses of seven RCTs.30 This study reported no significant difference in mortality at 7 days between patients receiving alteplase and those on placebo (10.6% vs 7.8%, p=0.13), with similar outcomes for mortality within 90 days.
The rate of IVT use increased annually in both older and younger patient groups throughout the study period, with the average annual growth rate being higher in older patients compared with younger ones (12.5% vs 9.1%). This trend aligns with the increasing IVT rates seen in developed countries. However, our study found that the IVT rate for patients treated within 4.5 hours of stroke onset was still significantly lower than the 63.9% reported in the Get with the Guidelines-Stroke initiative in the USA.31 Specifically, in 2022, the IVT usage rate in elderly patients was 34.2%, indicating that nearly two-thirds of eligible patients aged over 80 did not receive thrombolysis, highlighting the need for further improvement in this area.
Subgroup analysis showed that patients with moderate stroke derived more benefit from IVT, which is consistent with prior studies indicating stroke severity as an independent predictor of thrombolysis outcomes. Patients with less severe strokes (NIHSS<20) were shown to benefit more from IVT.32 While no evidence suggests that diabetes alters the efficacy of IVT, diabetic patients are generally linked to worse functional outcomes after thrombolysis.33–36 Our study also confirmed that diabetes does not modify the effect of thrombolysis; however, patients without diabetes tend to have better functional outcomes. Interestingly, elderly patients with atrial fibrillation benefit more from thrombolytic therapy, which may be related to our primary focus on in-hospital outcomes. This warrants further investigation into the long-term effects of thrombolysis in patients over 80 years who had a stroke with atrial fibrillation. Additionally, our findings indicate that prior use of antithrombotic agents should not be a reason to withhold IVT with alteplase in patients over 80 years with acute ischaemic stroke.
Several limitations should be acknowledged when interpreting these findings. First, we lacked data on 90-day postdischarge outcomes. However, previous studies have shown that discharge disability status and ambulation are strong predictors of 90-day outcomes37; suggesting that our discharge data may serve as reliable indicators. Second, as a retrospective, non-randomised study, there is potential for selection bias; however, we used the IPTW method to mitigate this issue. Finally, the study only included data from CSCA hospitals, which may not represent all hospitals in China. Nevertheless, the CSCA remains the largest stroke registry and quality improvement programme in China, including over 1 million patients who had an acute ischaemic stroke across 1751 hospitals, which provides a robust sample size for generalisation.
Conclusions
This nationwide, multicentre registry study evaluating the use of IVT in patients over 80 years who had an ischaemic stroke showed that alteplase treatment is beneficial for this population. Additionally, despite an increased incidence of sICH, there was no associated rise in in-hospital mortality. These findings further support the effectiveness of IVT with alteplase in elderly patients in China. While the rate of IVT use in older patients has increased each year, nearly two-thirds of eligible elderly patients who had a stroke still do not receive thrombolysis. Continued research is needed to better understand the medium-term and long-term outcomes of IVT in this age group.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the ethical review board of Beijing Tiantan Hospital (ethical approval number: KY2018-061-02). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank all participating hospitals, relevant clinicians, statisticians and imaging and laboratory technicians. We would like to thank Editage (www.editage.cn) for English language editing.
Footnotes
CL and YJ contributed equally.
Contributors ZL taken responsibility for the overall content as the guarantor. CW and ZL had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was supported by grants 2022YFC2504902 and 2022YFC2504904 from the Ministry of Science and Technology of the People’s Republic of China, grant Z200016 from the Beijing Natural Science Foundation, grant 2018000021223ZK03 from Beijing Talents Project and grants Z201100005620010 and Z211100002921064 from the Beijing Municipal Committee of Science and Technology.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}
{kind=link}