

Article Figures & Data
- Figure 1
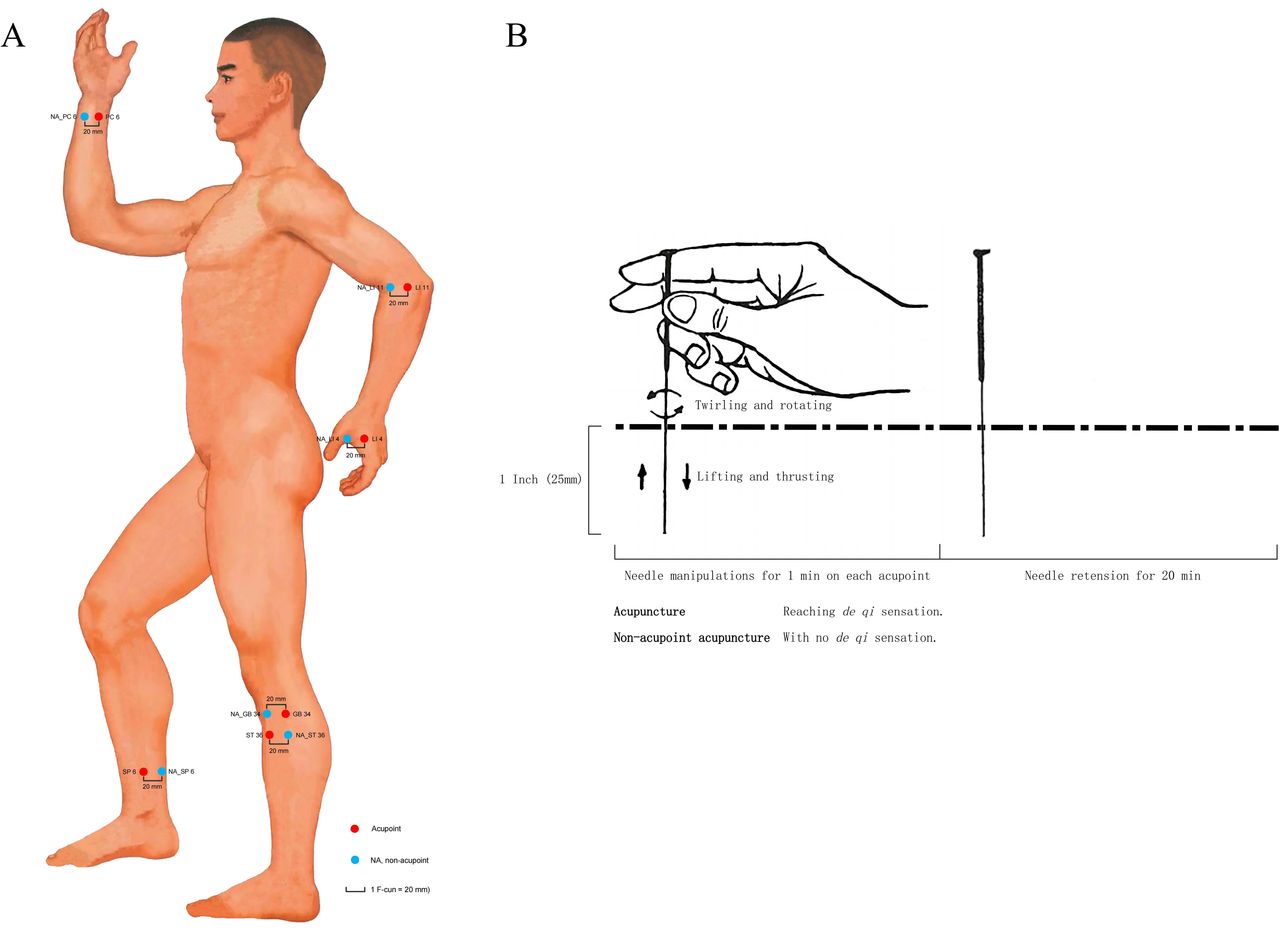
Acupuncture regimens. (A) Location of acupoints and non-acupoints. Standard measuring unit for acupoints was B-cun, which is one equal portion of the length between two points of particular joints. Measuring unit for non-acupoints was F-cun (1 F-cun=20 mm), which is defined as the width of the interphalangeal joint of patient’s thumb. (B) Acupuncture manual manipulation. Measurements involved the needle size and dosage were described with inch (1 inch=25 mm). NA, non-acupoint.
- Figure 2
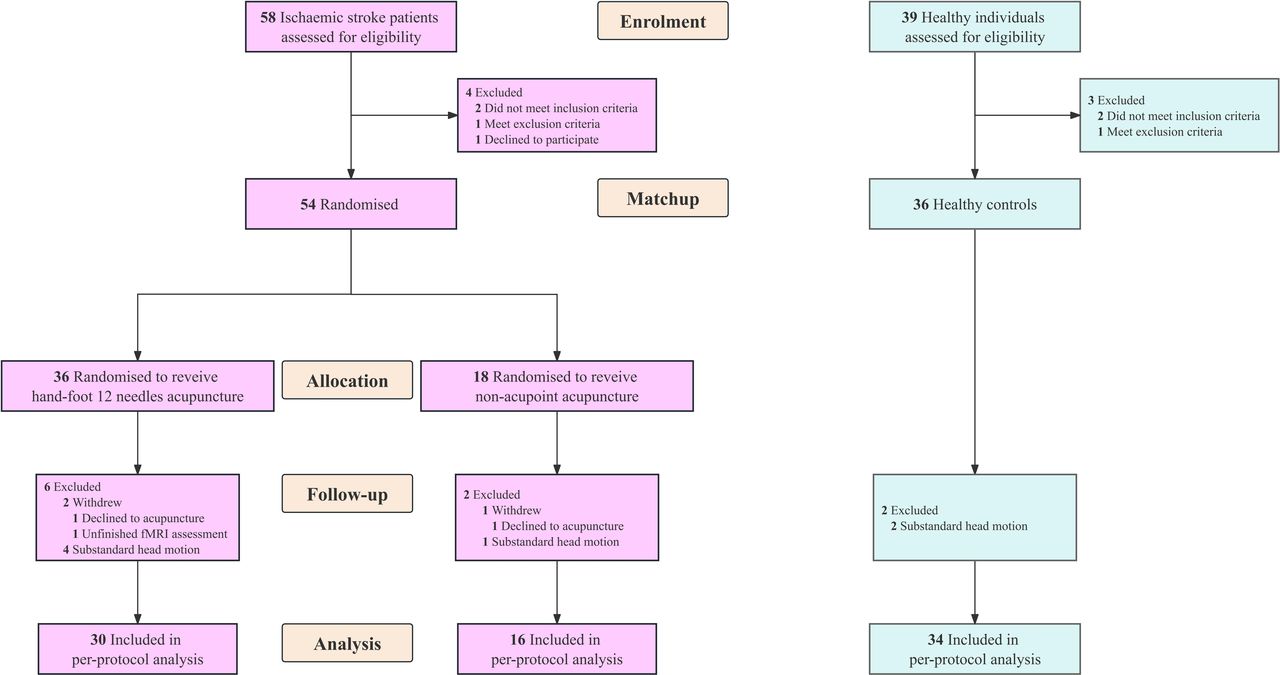
Study flow chart. fMRI, functional MRI.
- Figure 3
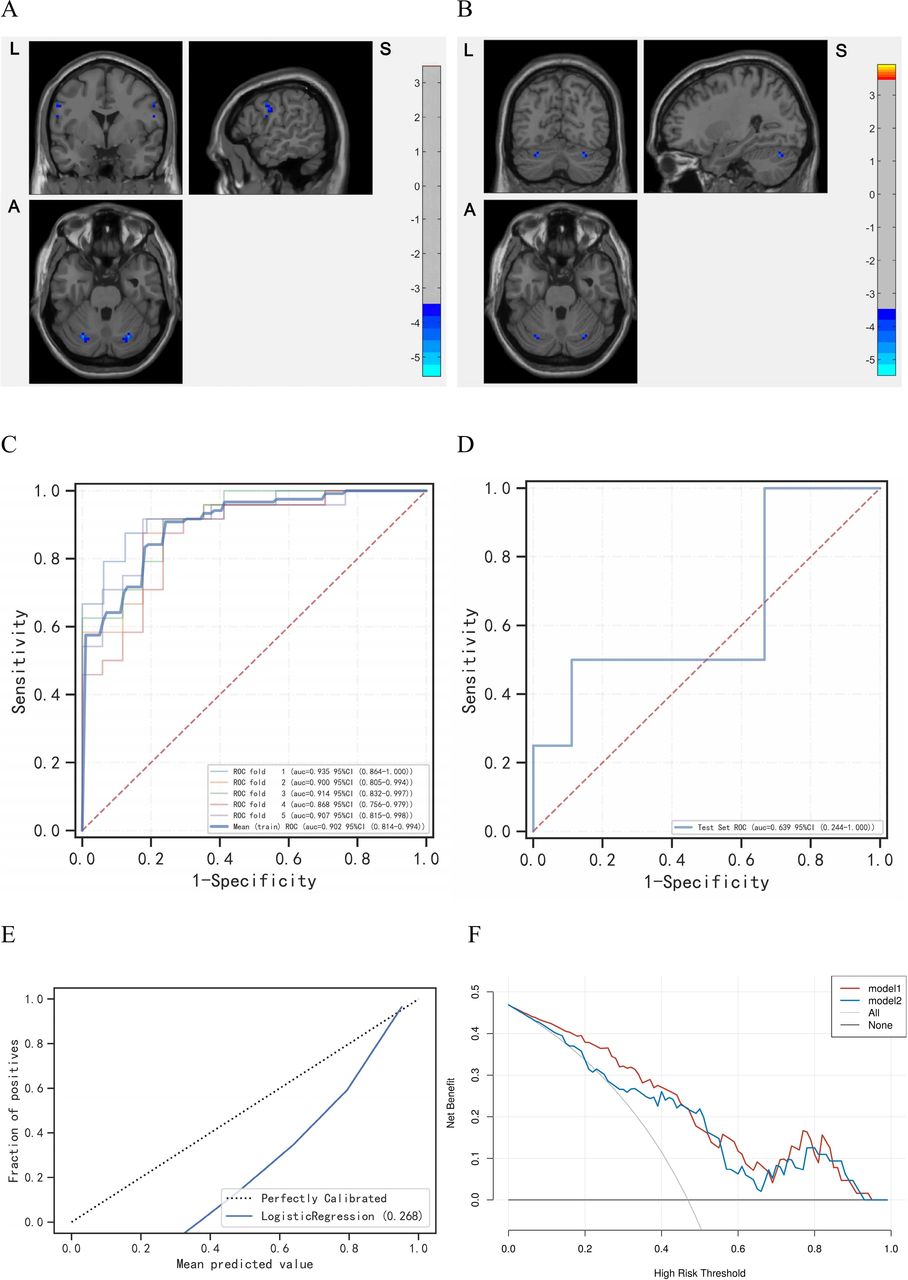
The pathologically cerebro-cerebellar VMHC captured by logistic regression based on machine learning. (A) The decreased VMHC in postcentral gyrus and cerebellum crus1 among the mild to moderate ISs. Red is increasing and blue is decreasing. (B) The decreased VMHC in cerebellum crus1 and cerebellum_6 among the severe ISs. Red is increasing and blue is decreasing. (C) The ROC of train set. (D) The ROC of test set. (E) The calibration curve of the logistic regression. (F) The test decision curve of the logistic regression. The model 1 is VMHC_Postcentral, and the model 2 is VMHC_Cerebellum. AUC, area under curve; IS, ischaemic stroke; ROC, receiver operating characteristic curve; VMHC, voxel-mirrored homotopic connectivity.
- Figure 4
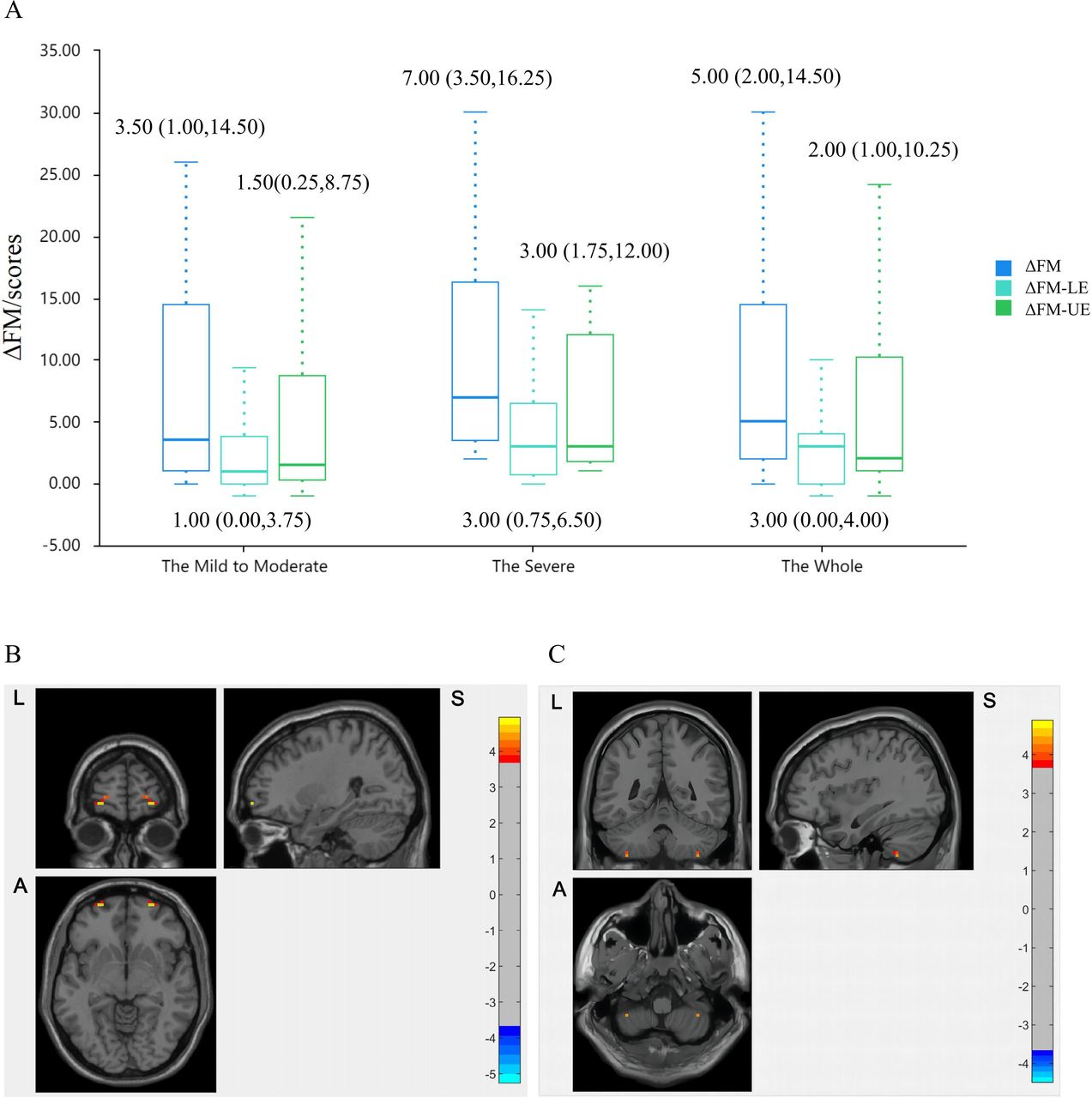
The clinical and neuroimaging outcomes. (A) The improvement of FM scores in HA group across motor-impairment severity subgroups. (B) The increased VMHC_Frontal_Sup_Orb in HA group following acupuncture. Red is increasing and blue is decreasing. (C) The higher VMHC_Cerebellum_8 in HA group compared with NA group in postacupuncture stage. Red is high and blue is low. FM, Fugl-Meyer; HA, hand-foot 12 needles acupuncture; LE, lower extremity; NA, non-acupoint; UE, upper extremity; VMHC, voxel-mirrored homotopic connectivity.
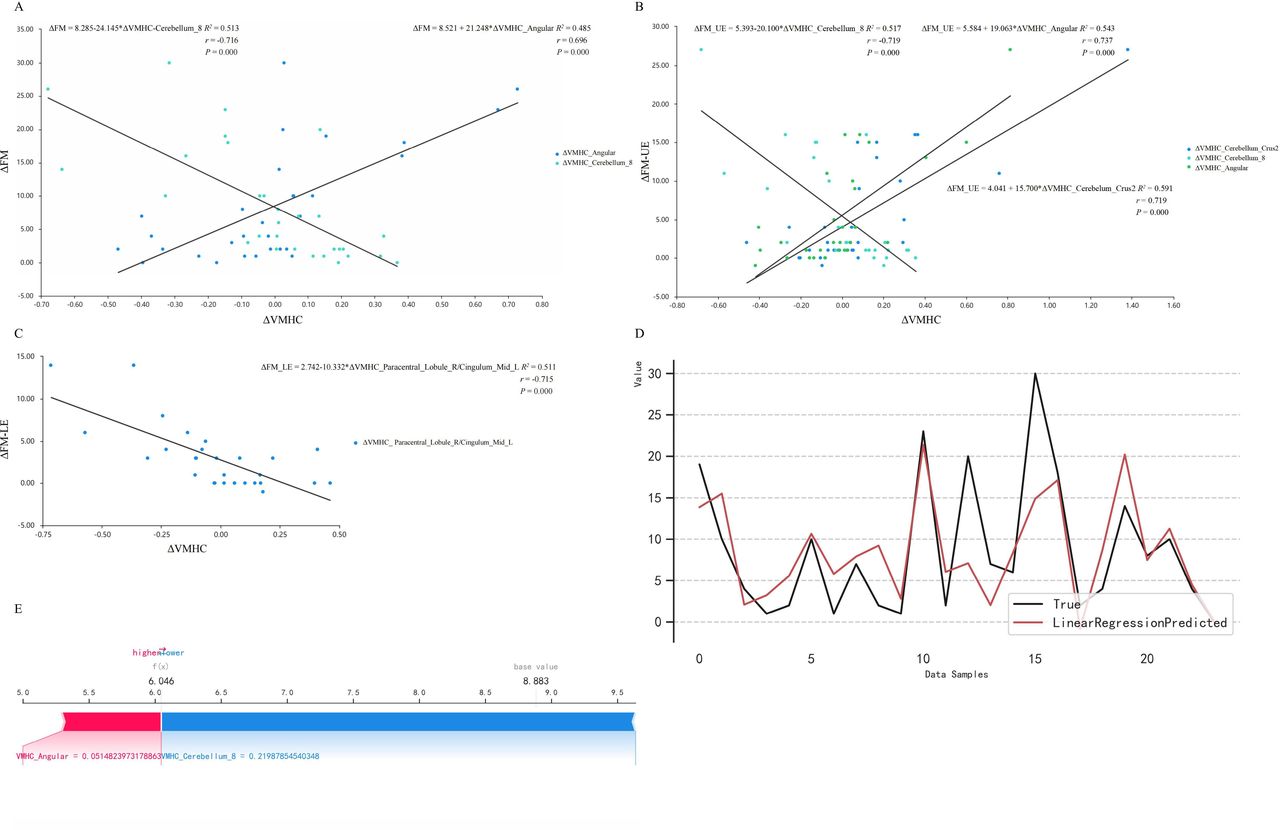
- Figure 5
The brain and behaviour effects of acupuncture. (A) The ΔFM was positively correlated with ΔVMHC_Angular and negatively with ΔVMHC_Cerebellum_8. (B) The ΔFM-UE was positively correlated with ΔVMHC_Cerebellum_Crus2 and ΔVMHC_Angular, and negatively with ΔVMHC_Cerebellum_8. (C) The ΔFM-LE was negatively correlated with ΔVMHC_Paracentral_Lobule_R/Cingulum_Mid_L. (D) The fitting curve of true value and predicted value based on the linear regression model. (E) The SHAP values of the ΔVMHC with its predictive values meaning the contribution to the ΔFM. The predicted positive contribution of angular gyrus was smaller than the negative contribution of cerebellum (base value=8.883, predicted value=6.046). FM, Fugl-Meyer; LE, lower extremity; SHAP, shapley additive explanation; UE, upper extremity; VMHC, voxel-mirrored homotopic connectivity.
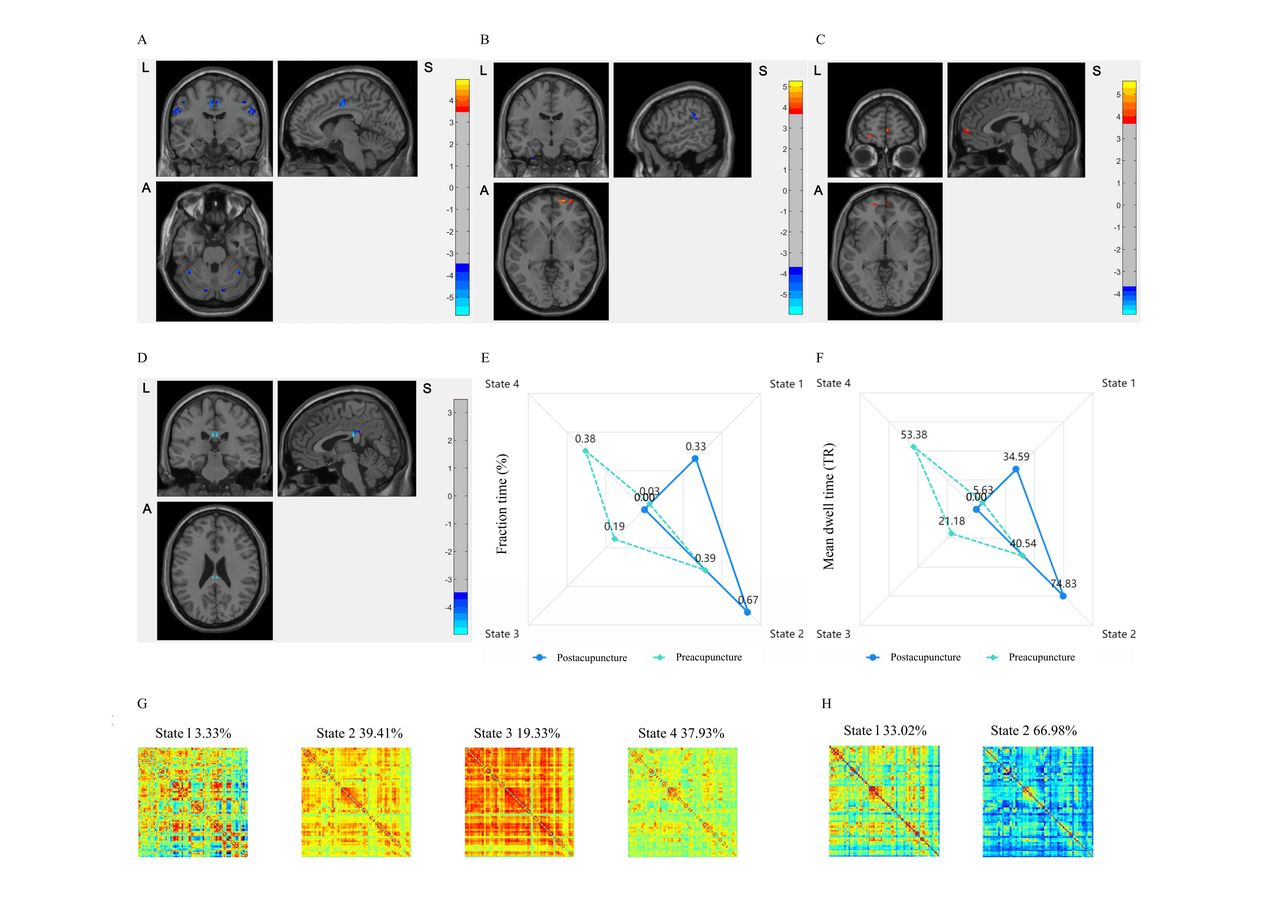
- Figure 6
The static and dynamic modification of acupuncture. (A) Regions reported decreased VMHC in HA group compared with HCs. (B) Changes on sFC with Frontal_Sup_Orb_R as ROI following acupuncture. (C) Changes on sFC with Frontal_Sup_Orb_L as ROI following acupuncture. (D) The decreased CV_VMHC of PCC following acupuncture. Red is increasing and blue is decreasing. (E) FT changes among DFC states following acupuncture. (F) MDT changes among DFC states following acupuncture. (G) The pattern of DFC states clustering in preacupuncture stage. (H) The pattern of DFC states clustering in postacupuncture stage. Red is positive weights and blue is negative weights. CV_VMHC, coefficient of variability of VMHC; DFC, dynamic functional connectivity; HA, hand-foot 12 needles acupuncture; HC, healthy control; PCC, posterior cingulate gyrus; ROI, region of interest; sFC, static function connectivity; VMHC, voxel-mirrored homotopic connectivity.






- Table 1
Demographics and baseline characteristics
Characteristics IS group (n=46) HC group (n=34) P value HA group (n=30) NA group (n=16) Gender, n (%)
(male/female)*31 (67.39)/15 (32.61) 21 (61.76)/13 (38.24) 0.602 Age, mean (SD), years
(male/female)†57.57 (13.68)/62.89 (9.79) 58.00 (9.89)/62.67 (5.50) 50.76 (10.89)/56.31 (6.33) 0.082/0.069
0.086/0.050Location of lesion, n (%)
(left/right)*15 (50.00)/15 (50.00) 7 (43.75)/9 (56.25) 0.686 Severity of motor impairment, n (%)
(mild to moderated/severed)*20 (66.67)/10 (33.33) 11 (68.75)/5 (31.25) 0.886 Duration, median (IQR), days ‡ 11.50 (7.00–20.50) 12.50 (4.30–34.80) 0.936 HAMD, median (IQR), scores‡ 6.00 (2.00–13.00) 7.50 (4.00–11.80) 0.835 MMSE, median (IQR), scores‡ 28.00 (24.80–29.00) 27.00 (24.30–29.80) 0.953 NIHSS, median (IQR), scores‡ 3.00 (1.00–5.00) 2.50 (1.00–5.80) 0.861 FM, median (IQR), scores‡ 74.00 (39.30–96.30) 85.00 (39.00–97.80) 0.579 Antihypertensives, n (%)
(yes/no)*14 (46.67)/16 (53.33) 7 (43.75)/9 (56.25) 0.850 Lipid-lowering agents, n (%)
(yes/no)*5 (16.67)/25 (83.33) 6 (37.50)/10 (62.50) 0.115 Hypoglycaemic agents, n (%)
(yes/no)*9 (30.00)/21 (70.00) 3 (18.75)/13 (81.25) 0.408 *χ² test. In order to avoid the information bias resulted from matching numbers, we adopted χ² test in HC group and IS group received acupuncture or non-acupoint acupuncture in sexual subgroups, respectively.
†Two-sample t-test.
‡Mann-Whitney U test.
FM, Fugl-Meyer; HA, hand-foot 12 needles acupuncture; HAMD, Hamilton Depression Scale; HC, healthy control; IS, ischaemic stroke; MMSE, Mini-mental State Examination; NA, non-acupoint; NIHSS, National Institute of Health Stroke Scale.
- Table 2
Primary and secondary outcomes
Variable HA group (n=30) NA group (n=16) Effect size (95% CI)* P value Primary outcomes† ΔFM, median (IQR), scores 5.00 (2.00–14.50) 2.50 (0.25–15.75) −1.00 (−7.00 to 1.00) 0.000 Secondary outcomes† ΔFM-UE, median (IQR), scores 2.00 (1.00–10.25) 2.00 (0.00–7.75) −1.00 (−4.00 to 1.00) 0.012 ΔFM-LE, median (IQR), scores 3.00 (0.00–4.00) 1.50 (0.00–3.75) 0.00 (−2.00 to 1.00) 0.000 *Estimated mean differences for clinical outcomes.
†Scheirer-Ray-Hare test.
FM, Fugl-Meyer; HA, hand-foot 12 needles acupuncture; IS, ischaemic stroke; LE, lower extremity; NA, non-acupoint; UE, upper extremity.
Supplementary Materials
Supplementary data
Additional Files
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}