

Abstract
Background Hypertension is widely acknowledged as a significant contributory factor to the heightened risk of intracranial aneurysm rupture. Nevertheless, the impact of hypertension management on the outcomes subsequent to aneurysmal subarachnoid haemorrhage (aSAH), particularly concerning the severity of aSAH, remains an underexplored area.
Methods We conducted a retrospective analysis using data from a prospectively multicentre cohort of 4545 patients with aSAH in China. Premorbid hypertension status and the utilisation of antihypertensive medications prior to admission were set as key exposure factors. The primary outcomes encompassed unfavourable clinical grading scales observed on admission. Employing multivariable logistic regression, we explored the association between premorbid hypertension status, preadmission use of renin-angiotensin-aldosterone system (RAAS) inhibitors and unfavourable clinical grading scales.
Results In comparison to patients with normal blood pressure, only uncontrolled hypertension demonstrated a significant and independent association with an elevated risk of poor outcomes on the Hunt-Hess scale (OR=1.799, 95% CI 1.413 to 2.291, p<0.001) and the World Federation of Neurological Surgeons (WFNS) scale (OR=1.721, 95% CI 1.425 to 2.079, p<0.001). Furthermore, the antecedent use of RAAS inhibitors before admission was markedly and independently linked to a diminished risk of adverse outcomes on the Hunt-Hess scale (OR=0.653, 95% CI 0.430 to 0.992, p=0.046) and the WFNS scale (OR=0.656, 95% CI 0.469 to 0.918, p=0.014).
Conclusions Uncontrolled hypertension markedly elevates the risk of adverse clinical outcomes following an aSAH. Conversely, the preadmission utilisation of RAAS inhibitors demonstrates a noteworthy association with a favourable clinical outcome after aSAH.
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is evidence that renin-angiotensin-aldosterone system (RAAS) inhibitors reduce the risk of aneurysmal subarachnoid haemorrhage (aSAH). Can preadmission use of RAAS inhibitors improve the severity of aSAH?
WHAT THIS STUDY ADDS
In this large nationwide population-based cohort study, preadmission use of RAAS inhibitors was significantly and independently associated with a reduced risk of poor Hunt-Hess scale and poor World Federation of Neurological Surgeons scale among patients with hypertension with aSAH.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
To attenuate the severity of aSAH, more efforts to achieve normalisation of blood pressure using RAAS inhibitors are suggested to be warranted in patients with hypertension with intracranial aneurysms.
Introduction
Subarachnoid haemorrhage (SAH), constituting around 5% of all strokes, imposes a significant disease burden due to its impact on a relatively young demographic and the associated elevated morbidity and mortality rates.1 In 85% of cases, aneurysm rupture serves as the primary cause, underscoring the pivotal role of effective intracranial aneurysm management in preventing this severe stroke subtype.
Hypertension has been unequivocally established as a modified risk factor for the rupture of intracranial aneurysms.2 3 Indeed, as many as 50% of individuals afflicted with intracranial aneurysms exhibit premorbid hypertension.2 4 More importantly, patients with aneurysmal subarachnoid haemorrhage (aSAH) who have a history of premorbid hypertension commonly exhibit heightened severity of haemorrhage and experience poorer outcomes.5 6 Therefore, effective hypertension management is pivotal for patients with intracranial aneurysms, as it diminishes the risk of rupture and enhances outcomes subsequent to aSAH. While the impact of hypertension management on the risk of aSAH rupture has been recognised in previous studies,3 7 8 there remains a notable gap in understanding its influence on post-aSAH outcomes,9 with a specific dearth of research on the severity of aSAH. The severity of aSAH stands as the paramount determinant influencing both treatment strategies and outcomes. Consequently, an imperative exists to comprehend thoroughly the repercussions of hypertension management on the severity of aSAH.
In hypertension management, the utilisation of appropriate antihypertensive medications is imperative for achieving blood pressure normalisation. Presently, both experimental and clinical evidence strongly indicate that the renin-angiotensin-aldosterone system (RAAS) inhibitors may confer a vasoprotective effect, thereby mitigating the risk of intracranial aneurysm rupture.7 10–12 In light of the documented inhibition of the RAAS, which correlates with a reduction in inflammation within the vessel wall, RAAS inhibitors emerge as potential contributors to a vasoprotective effect, fostering a favourable clinical outcome after aSAH. Building on this evidence, our hypothesis posits that the pre-emptive utilisation of RAAS inhibitors before admission may effectively mitigate the severity of the condition in patients with hypertension experiencing aSAH. Accordingly, the primary objective of this study is to investigate the influence of blood pressure regulation on the severity of aSAH. Specifically, we aim to discern the beneficial impact associated with the preadmission use of RAAS inhibitors on disease severity.
Methods
Study database
The study database was derived from the National Research and Development Project of Intracranial Aneurysms in China. The details regarding the project have been described previously.7 8 The project entailed collaboration with 20 tertiary academic medical centres to establish a nationwide, prospectively maintained database of intracranial aneurysms. Within this dedicated database, information on patients with intracranial aneurysms from the designated centres was systematically and prospectively recorded using an Electronic Data Capture system, adhering to predefined coding rules. The current study involved a retrospective analysis, drawing insights from the prospectively collected multicentre cohort of aSAH. To mitigate potential distortion and bias in the analysis, we meticulously executed a standard operating procedure in accordance with pertinent recommendations.13 The detailed methodology has been comprehensively documented in our prior publication.7 In addition, the presentation of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology statement,14 and the corresponding checklist is provided in the online supplemental material, section S1.
Supplementary data
Study population
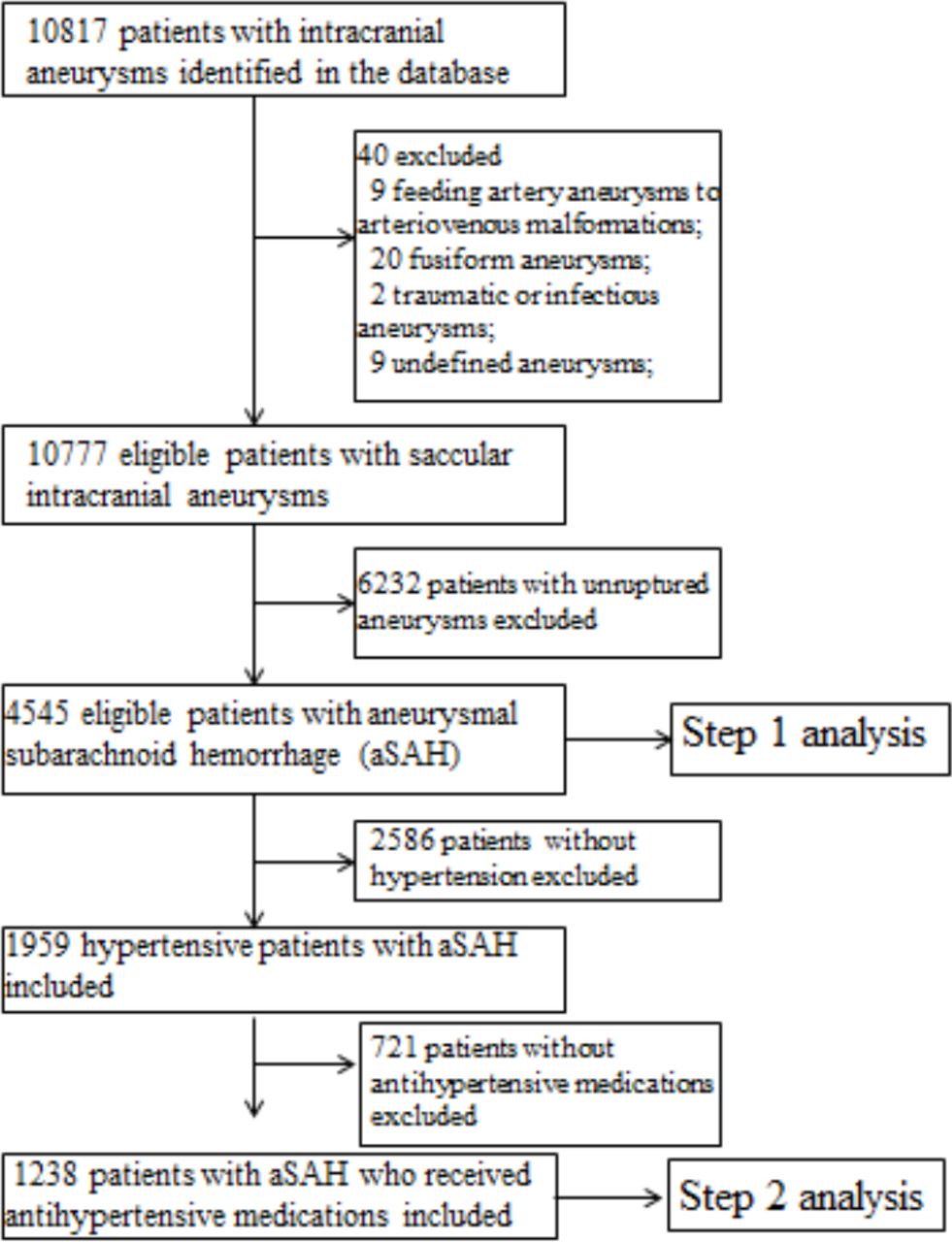
During the process of analysing the impact of blood pressure control on the severity of aSAH (step 1 analysis), the study population was adult patients with aSAH registered in the database. During the process of analysing the effect of preadmission use of RAAS inhibitors on the disease severity (step 2 analysis), the study population was patients with hypertension with aSAH who had been regularly treated with antihypertensive medications before admission. The detailed inclusion and exclusion criteria are presented in the online supplemental material, section S2. A flow diagram delineating how the included patients were derived from the source population is presented in figure 1.

Flow diagram delineating how the study population was derived from the source population. A total of 10 817 patients with intracranial aneurysms were reviewed initially. Finally, a total of 4545 patients with aneurysmal subarachnoid haemorrhage (aSAH) were enrolled in this study, of whom 1959 patients (43.10%) had premorbid hypertension. During the step 2 analysis, 1238 patients with hypertension with aSAH, including 290 renin-angiotensin-aldosterone system (RAAS) inhibitor users (23.42%) and 948 non-RAAS inhibitor users (76.58%), were included.
Exposure assessment
Data for all enrolled patients were systematically gathered using a standardised form containing predefined variables, as detailed in our prior description.7 8 In evaluating exposure, a set of prospectively ascertained variables, each with predefined definitions, were employed. These variables encompassed age, sex, ethnicity, body mass index (BMI), smoking habits, alcohol consumption, premorbid comorbidities, prescribed medications and aneurysmal indices.
Besides, for patients with hypertension with aSAH, the control of hypertension and the preadmission use of antihypertensive medications were also assessed. In accordance with established coding rules, hypertension is defined as systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg, measured in the sitting position on at least three different occasions in the office (referred to as office blood pressure), following the guidelines.15 Additionally, diagnostic criteria for out-of-office blood pressure were considered valid. In delineating the hypertension status, patients with hypertension were classified into three categories: controlled, uncontrolled and unmonitored hypertension. Controlled hypertension is characterised by regular blood pressure monitoring, coupled with the successful attainment of target blood pressure through the administration of appropriate antihypertensive medications. Conversely, uncontrolled hypertension is delineated by the consistent monitoring of blood pressure without reaching the target levels, despite the use of suitable antihypertensive medications. The target blood pressure is defined as an average blood pressure of ≥140/90 mm Hg (office blood pressure) and/or 135/85 mm Hg (out-of-office blood pressure). It is noteworthy that in specific hypertension-related conditions, such as diabetes or among elderly individuals, adaptations were made in accordance with the European Society of Cardiology guidelines.15 Unmonitored hypertension refers to patients with hypertension undergoing antihypertensive treatment but neglecting regular blood pressure monitoring, thereby lacking sufficient data for a comprehensive assessment of their blood pressure control status. The detailed definitions regarding hypertension control have been described in our previous work.8 Moreover, according to the classes of preadmission antihypertensive medications, patients with hypertension were categorised as RAAS inhibitor users and non-RAAS inhibitor users. The RAAS inhibitor users were defined as patients with hypertension with aSAH who were prescribed RAAS inhibitors for at least 3 months before admission, encompassing both monotherapy and combination therapy.
Outcome assessment
To fully evaluate the severity of aSAH, two commonly used clinical grading scales,1 including the Hunt-Hess scale and the World Federation of Neurological Surgeons (WFNS) scale (online supplemental material, section S3), were assessed for all patients on admission and set as the primary outcomes. In this study, poor Hunt-Hess scale and poor WFNS scale were defined as grade ≥4 (ie, grades 4 and 5), whereas good Hunt-Hess scale and good WFNS scale were defined as grade <4 (ie, grades 1–3).
Statistical analysis
Descriptive statistics
Continuous variables were expressed as the mean (SD) or median (IQR), and the differences between the two groups were analysed using Student’s t-test or the Mann-Whitney test, as appropriate. Categorical variables were expressed as numbers (frequencies), and the differences between the two groups were analysed using χ2 test or Fisher’s exact test. All data were handled and analysed using SPSS Statistics V.25.0 (SPSS) and R programming environment (R Foundation for Statistical Computing, Vienna, Austria). All statistical significance was defined as p<0.05.
Multiple imputation and multivariable logistic regression model
To cope with the missing data, a multiple imputation approach was performed following the relevant guidelines.16 The details of the multiple imputation approach are presented in the online supplemental material, section S4. Based on the 25 imputed datasets, we constructed multivariable logistic regression models to detect the impact of hypertension control and antihypertensive medication choice on the severity after aSAH. Initially, univariable analysis was performed to select the potential covariates. The variables that were theoretically thought to be related to the severity of aSAH, such as age, sex, BMI, smoking, hypertension status, and number, location, size and shape irregularity of the ruptured intracranial aneurysm, as well as those who had a p value <0.1 in univariable analysis were included in the multivariable logistic model. During the process in SPSS, the pooled analysis of the results would be automatically generated based on the 25 imputed datasets. We set the pooled results as the final results of multivariable analysis.
Sensitivity analyses and subgroup analyses
Sensitivity analyses comparing complete data and multiply imputed data were performed. Based on the multivariable model, interaction and stratified analyses were conducted. The p value for interaction was estimated during this process.
Results
Comparisons of baseline characteristics between patients with and without hypertension
The comparative analysis of baseline characteristics between patients with and without hypertension is shown in online supplemental table S1. Notably, disparities were observed in preadmission anti-platelet (PLT) medications and irregular aneurysms, with all comparisons displaying statistical significance (p<0.05).
Effect of preadmission blood pressure control on the two poor clinical grading scales of aSAH
Table 1 shows the impact of preadmission blood pressure control on the adverse clinical grading scales of aSAH. In comparison to individuals with normal blood pressure, those with premorbid hypertension exhibited a significant and independent association with an elevated risk of poor outcomes on both the Hunt-Hess and WFNS scales in patients diagnosed with aSAH. Notably, when examining the controlled status of hypertension, only uncontrolled hypertension demonstrated a significant and independent correlation with an increased risk of poor Hunt-Hess scale (OR=1.799, 95% CI 1.413 to 2.291, p<0.001) and poor WFNS scale (OR=1.721, 95% CI 1.425 to 2.079, p<0.001). In contrast, the effects of controlled hypertension and unmonitored hypertension did not reach statistical significance.
Impact of preadmission hypertension statuses on the two poor clinical grading scales of aSAH
Comparisons of baseline characteristics between RAAS inhibitor and non-RAAS inhibitor users
In the course of the second step analysis, a cohort of 1238 patients with hypertension with aSAH underwent examination. Among them, 290 individuals (23.42%) were identified as users of RAAS inhibitors, while the remaining 948 patients (76.58%) did not use RAAS inhibitors. A detailed scrutiny of baseline characteristics between RAAS inhibitor users and non-users is delineated in online supplemental table S2. Notably, substantial disparities were observed in the distribution of ethnicity, the controlled status of hypertension, the quantity of antihypertensive drugs, preadmission anti-PLT medications and the presence of irregular aneurysms between these two cohorts (all p<0.05).
Treatment effect of RAAS inhibitors on the two poor clinical grading scales of aSAH
Table 2 shows the treatment impact of RAAS inhibitors on the two adverse clinical grading scales of aSAH. In contrast to the preadmission use of non-RAAS inhibitors, the preadmission utilisation of RAAS inhibitors exhibited a significant and independent association with a diminished risk of poor outcomes on the Hunt-Hess scale (OR=0.653, 95% CI 0.430 to 0.992, p=0.046) and the WFNS scale (OR=0.656, 95% CI 0.469 to 0.918, p=0.014) among patients with hypertension with aSAH. Furthermore, there was an inclination for favourable clinical grading scales with varied cut-offs when RAAS inhibitors were used before admission, as indicated in online supplemental table S3.
Treatment effect of RAAS inhibitors on the two poor clinical grading scales of aSAH
Sensitivity analyses
In the initial phase of analysis (step 1), 2925 complete cases underwent thorough examination, while in the subsequent phase (step 2), 806 complete cases were scrutinised. The findings of sensitivity analyses, exploring the influence of blood pressure control and RAAS inhibitors on the severity of aSAH, are meticulously presented in tables 1 and 2, correspondingly. The impact of both hypertension control and RAAS inhibitors remained consistent across diverse datasets employed for analysis.
Subgroup analyses and tests for interaction for the treatment effect of RAAS inhibitors on the severity of aSAH
Interaction and subgroup analyses regarding the treatment effect of RAAS inhibitors on the severity of aSAH are depicted in figure 2. The beneficial impact of RAAS inhibitors on disease severity was notably pronounced within the subgroup characterised by controlled hypertension, combination therapy and irregular aneurysms. Particularly, the results of the interaction test revealed that hypertension control and age exhibited a significant interaction effect with the use of RAAS inhibitors on outcomes.

Interaction and subgroup analyses for the treatment effect of renin-angiotensin-aldosterone (RAAS) inhibitors on the severity of aneurysmal subarachnoid haemorrhage (aSAH). The beneficial impacts of RAAS inhibitors on Hunt-Hess scale (A) and World Federation of Neurological Surgeons (WFNS) scale (B) were notably pronounced within the subgroup characterised by controlled hypertension, combination therapy and irregular aneurysms. Particularly, the results of the interaction test revealed that hypertension control and age exhibited a significant interaction effect with the use of RAAS inhibitors on outcomes. ‘posterior’ denotes posterior circulation (including the vertebral artery, basilar artery, cerebellar arteries and posterior cerebral artery). ACA, anterior cerebral arteries (including the anterior cerebral artery, anterior communicating artery and pericallosal artery); BMI, body mass index; ICA, internal carotid artery; MCA, middle cerebral artery; PCoA, posterior communicating artery; PLT, platelet.
Discussion
In this extensive nationwide population-based cohort study, we have demonstrated a significant association between uncontrolled hypertension and an increased risk of a poor clinical condition following aSAH. More importantly, the preadmission utilisation of RAAS inhibitors exhibited a significant association with a favourable clinical condition after aSAH, with a more pronounced beneficial effect observed in the subpopulation with controlled hypertension. To the best of our knowledge, this study stands as the inaugural and largest exploration to date, investigating the advantageous impact of preadmission use of RAAS inhibitor in mitigating the severity of aSAH.
Our findings reveal a significant correlation between premorbid hypertension and a compromised clinical condition among patients with aSAH. Broadly, the pathogenesis of intracranial aneurysm development centres around haemodynamic-mediated vascular endothelial dysfunction and subsequent inflammatory cascades within the vascular wall. Various explanations elucidate the pathogenic mechanisms through which hypertension augments clinical severity after aSAH. Notably, the pressure-induced tension, arising from the heightened haemodynamic stresses in hypertension, likely exceeds the strength of the aneurysmal wall.17 In this scenario, elevated stress levels may result in a greater volume of aneurysmal bleeding following an aneurysm rupture. Supporting this assertion, De Marchis et al5 illustrated that patients with SAH and pre-existing hypertension exhibited heightened severity during the initial bleeding episode on admission. On the contrary, sophisticated structural damage to blood vessels resulting from atherosclerotic disease is frequently observed in individuals with hypertension. Consequently, heightened vascular injuries are likely to impede the natural healing processes associated with ruptured aneurysms.18 For example, premorbid hypertension has been identified as a significant factor associated with a twofold increase in the incidence of aneurysm rebleeding.5 This risk factor demonstrates a robust correlation with the severity of aSAH.
While a substantial correlation exists between premorbid hypertension and the severity of aSAH, the prior study did not investigate whether the clinical condition after SAH could be improved through blood pressure control.5 In the present study, we established that inadequately controlled hypertension exhibits a more substantial impact on the severity of aSAH compared with well-controlled hypertension. This outcome concurs with the findings of Zheng et al, indicating that individuals with uncontrolled premorbid hypertension in SAH cases suffered more amount of aneurysmal bleeding.19 A plausible explanation for this phenomenon may be that inadequately managed hypertension often signifies a poor grade of hypertension or resistant hypertension, thereby introducing unstable and increased haemodynamic stress on the aneurysmal wall.17 The reduction in blood pressure commonly serves to stabilise haemodynamic stress within the vessel and mitigate inflammation in the aneurysmal wall. As previously highlighted, both these factors potentially play a role in ameliorating the severity following aSAH. Primarily, the reduction in blood pressure may alleviate moderate pressure-induced tension, thereby reducing the extent of aneurysmal bleeding in the event of rupture. Consequently, this could result in a less severe clinical condition. Second, the amelioration of inflammation attributed to the decrease in blood pressure may have a favourable impact on the healing process of a ruptured aneurysm. To mitigate the severity of aSAH, it is recommended to intensify efforts towards normalising blood pressure for patients with hypertension with intracranial aneurysms. In recent times, various implementation strategies have been proposed to enhance the management of blood pressure in patients with hypertension with intracranial aneurysms.20 First, precise blood pressure measurement contributes to superior blood pressure control and mitigates the risk of aneurysm rupture, as substantiated in our prior research.8 Second, a collaborative effort involving a minimum of two professionals from neurosurgery and cardiology, constituting team-based care, is imperative to achieve well-coordinated and high-quality healthcare for the patients. Lastly, the judicious use of appropriate antihypertensive medications is indispensable in realising the reduction in blood pressure for patients with intracranial aneurysms. Significantly, an excessive reduction in blood pressure may result in hypoperfusion subsequent to SAH. A plethora of studies have investigated the implications of hypoperfusion following SAH on the overall prognosis, with the majority yielding negative outcomes. Consequently, it is imperative to avert excessive decreases in blood pressure and ensure adequate perfusion in patients prior to admission.
Classically, RAAS inhibitors could exert multiple cardiovascular protective effects.21 In this study, we have further illustrated that the preadmission use of RAAS inhibitors is significantly linked to a diminished risk of unfavourable clinical grading scales in patients with hypertension with aSAH. Considering that the activation of RAAS due to systemic hypertension can induce vascular inflammation, injury and remodelling, subsequently contributing to the progression of intracranial aneurysm development,10 several explanations underpin our findings. First, RAAS inhibitors have the potential to curtail both local and systemic inflammatory responses, consequently contributing to the mitigation of aSAH severity. On the one hand, these inhibitors may induce a modest level of inflammation and promote vascular injury/remodelling in the aneurysmal wall. Subsequently, this intervention holds promise for cultivating a clinically favourable condition after aSAH. On the contrary, RAAS inhibitors possess the capacity to mitigate systemic inflammation by suppressing the activation of the systemic RAAS. Simultaneously, a heightened level of systemic inflammation response has been significantly correlated with an unfavourable Hunt-Hess scale and poorer Fisher score in the context of SAH.22–24 These findings suggested that the restrained systemic inflammation response facilitated by RAAS inhibitors was likely to contribute to a more favourable clinical condition following aSAH. Additionally, compelling experimental evidence supports the notion that RAAS inhibitors have the potential to impede the formation and growth of intracranial aneurysms.25 26 For instance, imidapril, a subclass of ACE inhibitors, showed a remarkable capacity to effectively inhibit the medial thinning of intracranial aneurysms in rat models.25 As is widely recognised, an intracranial aneurysm characterised by thinning of the medial layer indicates a weakened structural stability. Theoretically, such vulnerability could lead to a compromised clinical condition on rupture. Third, consistent with our result, a preceding clinical study19 revealed that patients with hypertension, who were prescribed RAAS inhibitors prior to admission, exhibited a reduced incidence of aneurysmal bleeding—an integral risk factor influencing the severity of aSAH. Interestingly, the favourable impact of RAAS inhibitors on disease severity manifested more prominently within the subgroup characterised by controlled hypertension. This outcome suggests that the positive effect of RAAS inhibitors is unrelated to blood pressure control. Put differently, the diminished risk of adverse clinical outcomes following aSAH in the context of RAAS inhibitors does not stem from blood pressure reduction. Nevertheless, the precise mechanism remains unknown, warranting further research with a heightened focus on this specific aspect.
This study carries significant implications for clinical practice. On the one hand, the study underscores the pivotal role of normalising blood pressure in the comprehensive management of hypertension among these patients. On the other hand, our findings, for the first time, shed light on the potential advantages of preadmission use of RAAS inhibitors in mitigating clinical conditions after aSAH.
Limitations
Despite the attractive findings of our study, several limitations should be taken into account seriously. First, the study design is retrospective rather than prospective and therefore the cause-effect is weak in this study. Second, the duration and the dose of antihypertensive medications were not recorded in the database. On the one hand, the distinct effect between the current use and former use of RAAS inhibitors could not be detected. On the other hand, we could not perform a duration–response analysis and a dose–response analysis to further assess whether the beneficial effect is duration dependent or dose dependent. Further studies, which take these variables into account, will need to be undertaken. Third, our study is based on the Chinese population, and replication of the results in other populations is suggested. Fourth, the exact level of blood pressure at the time of enrolment was not involved and the impact of the stratifications of blood pressure reduction on the outcomes was unknown. This is an important issue for future research. Fifth, although all included patients were strictly categorised according to the prescribed medication class, the lack of patient-specific data on medication compliance would influence the results.
Conclusions
In conclusion, our investigation reveals that uncontrolled hypertension markedly escalates the risk of adverse clinical outcomes following aSAH. Notably, the antecedent utilisation of RAAS inhibitors demonstrates a substantial correlation with a favourable clinical status subsequent to aSAH. The outcomes underscore the potential advantages associated with the preadmission use of RAAS inhibitors in mitigating the severity of aSAH. To address the severity of aSAH, heightened endeavours to achieve blood pressure normalisation through RAAS inhibitors are recommended for patients with hypertension with intracranial aneurysms. Nevertheless, it is imperative to acknowledge that a comprehensive prospective cohort study incorporating mechanistic insights is indispensable to corroborate our findings in the future.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the local institutional review board (IRB) from Changhai Hospital, Second Military Medical University (CHEC2017073). All methods were carried out in accordance with the Declaration of Helsinki. Due to the observational design of this study, the patient's informed consent was waived by the IRB.
Footnotes
Contributors ZLi and ZLu collected the data and performed the research. Data were analysed by PZ. PZ drafted the manuscript. SC, ZW and QH conceived and designed the research. LJ, LT, QL and QH initiated and organised this study. QH accepts full responsibility for the work and the conduct of the study as the guarantor, had access to the data, and controlled the decision to publish. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding This study was funded by the National Research and Development Project of Key Chronic Diseases (Grant No. 2016YFC1300703), the Fujian Provincial Natural Science Foundation of China (Grant No. 2021J011367 and No. 2021J011353), the Medical Project of Xiamen Municipal Bureau of Science and Technology (Grant No. 3502Z20214ZD1013), Xiamen Municipal Health Commission, Xiamen Municipal Bureau of Science and Technology (Grant No. 3502Z20209005), Fujian Provincial Clinical Research Center for Brain Diseases (Grant No. 2021FJSLCYX01) and Xiamen Clinical Research Center for Neurological Diseases (Grant No. 2021XMSLCYX01).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}