

Abstract
Rationale The effect of the head position as a non-pharmacological therapy on acute ischaemic stroke (AIS) remains inconclusive. Our recent Head dOwn-Position for acutE moderate ischaemic Stroke with large artery atherosclerosis (HOPES 2) suggested the safety, feasibility and potential benefit of the head-down position (HDP) in AIS.
Aim To investigate the benefit of HDP in acute moderate ischaemic stroke patients with large artery atherosclerosis (LAA).
Sample size estimates Based on a two-sided 0.05 level of significance, 600 patients are expected to yield the superiority hypothesis with 80% power, stratified by age, sex, history of diabetes, baseline systolic blood pressure, location of index vessel, National Institutes of Health Stroke Scale Score at randomisation, onset to randomisation time, progression to moderate neurological deficit due to early neurological deterioration and degree of responsible vessel stenosis.
Design Head dOwn-Position for acutE moderate ischaemic Stroke with large artery atherosclerosis(HOPES 3) is a prospective, randomised, open-label, blinded endpoint and multicentre study. Eligible patients who had an ischaemic stroke will be randomly assigned (1:1) into the HDP group receiving −20° Trendelenburg plus standard medical care in compliance with national guidelines, or control group only receiving standard medical care in compliance with national guidelines.
Outcome The primary outcome is favourable functional outcome, defined as modified Rankin Scale 0–2 at 90 days. Safety outcomes are HDP-related adverse events. All outcomes will have blinded assessment and will be analysed on the intention-to-treat basis.
Conclusions The results of HOPES 3 will provide evidence for the effect of HDP in acute moderate ischaemic stroke patients with LAA within 24 hours of onset or in patients with progression from mild neurological deficit within 24 hours.
Trial registration number NCT06010641.
Introduction and rationale
The effect of head position (lying flat vs sitting up) as a non-pharmacological therapy for stroke has been widely investigated,1–4 but the results remain inconclusive, which has led to ambiguous recommendations by current guidelines.5–7 Compared with the sitting-up position, the supine or lying-flat position can increase blood flow and improve oxygenation,1–3 8–10 but it may increase the risk of intracranial pressure, cardiopulmonary dysfunction and aspiration pneumonia.11–14 The Head Positioning in Acute Stroke Trial (HeadPoST) was the first large study to compare the effects of the lying-flat versus sitting-up position in patients who had an acute ischaemic stroke (AIS), and the results showed that the lying-flat position was safe, but ineffective.4 The neutral results may be attributed to the broad inclusion of patients who had a stroke. While patients with large artery atherosclerosis (LAA) aetiology could be a suitable target population,15 subgroup analysis of HeadPoST did not detect any evidence of heterogeneity of treatment effect across clinician-diagnosed stroke subtypes.16
In theory, compared with the supine or lying-flat position, the steeper head-down position (HDP) (ie, fully supine with Trendelenburg17) could significantly increase blood flow to the ischaemic penumbra and improve oxygenation of the brain in the first hours or days after stroke.18 The proposal was further supported by animal experiments showing that HDP with −15° or −30° could improve neurological function and reduce infarct volume.19–22 Moreover, observational studies also found that the HDP may increase cerebral perfusion and improve clinical outcomes without an increased risk of aspiration pneumonia.23 24 Remarkably, our phase 2 Head dOwn-Position for acutE moderate ischaemic Stroke with large artery atherosclerosis (HOPES 2) randomised trial suggested that the HDP seems safe and feasible, did not improve 90-day favourable functional outcome as primary outcome, but a direction of benefit was present with the potential to improve secondary outcomes.25
In this context, given the safety profile and potential benefit of HDP, this phase 3 HOPES 3 randomised trial is designed to confirm the benefit of the HDP in acute moderate ischaemic stroke patients with LAA.
Methods
Design
HOPES 3 is a prospective, randomised, open-label, blinded endpoint and multicentre study in China assessing the benefit of HDP in acute moderate ischaemic stroke patients with LAA. The HOPES 3 trial is registered on www.clinicaltrial.gov (NCT06010641).
Study population
In the HOPES 3 trial, eligible patients are adults with acute anterior circulation moderate ischaemic stroke (initial National Institutes of Health Stroke Scale (NIHSS) 6–16, presenting within 24 hours of onset, or progressing from mild stroke (NIHSS≤5) to moderate stroke (NIHSS 6–16) within 24 hours). Patients who are candidate for reperfusion therapy or planned carotid or intracranial artery revascularisation within 3 months are excluded. Vessel stenosis will be determined by Computed Tomography Angiography(CTA) or Magnetic Resonance Angiography(MRA) before or after randomisation. Moderate stenosis will be estimated as 50% to 69% stenosis and severe stenosis as 70% stenosis or greater according to the Warfarin Aspirin Symptomatic Intracranial Disease(WASID) method of measurement. Patients will be enrolled at approximately 50 sites in China between November 2023 and June 2025. The detailed inclusion and exclusion criteria are shown in box 1.
The inclusion/exclusion criteria
Inclusion criteria:
Age ≥18 years old.
Acute ischaemic stroke confirmed by NCCT or MRI.
Moderate neurological deficit (6≤NIHSS≤16) within 24 hours of onset, or progressing from mild (NIHSS≤5) to moderate neurological deficit (NIHSS 6–16) within 24 hours, requiring ≥4 point increase in NIHSS Score when the onset time of stroke symptom is beyond 24 hours.
Probable large artery atherosclerosis aetiology based on the Trial of Org 10 172 in Acute Stroke Treatment criteria (responsible artery stenosis ≥50% or occlusion).
Anterior circulation stroke (internal carotid artery, M1 or M2 of middle cerebral artery).
First stroke onset or past stroke without obvious neurological deficit (mRS≤2).
Signed informed consent.
Exclusion criteria:
Prestroke disability (mRS≥3).
Patients with disturbance of consciousness.
Patients who plan to undergo or have completed thrombolysis or mechanical thrombectomy.
Haemorrhagic stroke or combined ischaemic and haemorrhagic stroke.
Serious comorbidity, such as liver or kidney insufficiency, malignant tumour, etc.
Other stroke aetiologies, such as cardiogenic embolism, arteritis, arterial dissection, moyamoya disease, etc.
History of intracerebral haemorrhage within 1 year.
Any contraindication to head-down position (eg, active vomiting, pneumonia, uncontrolled heart failure).
Planned carotid or intracranial revascularisation within 3 months.
Severe uncontrolled hypertension (systolic blood pressure over 180 mm Hg or diastolic blood pressure over 100 mm Hg).
Cardiac insufficiency (NYHA class ≥II).
Pregnant or lactating women.
Comorbidity with other serious diseases.
Participating in other clinical trials within 3 months.
Patients not suitable for the study considered by researcher.
mRS, modified Rankin Scale; NCCT, non-contrast CT; NIHSS, National Institutes of Health Stroke Scale.
Randomisation and treatment
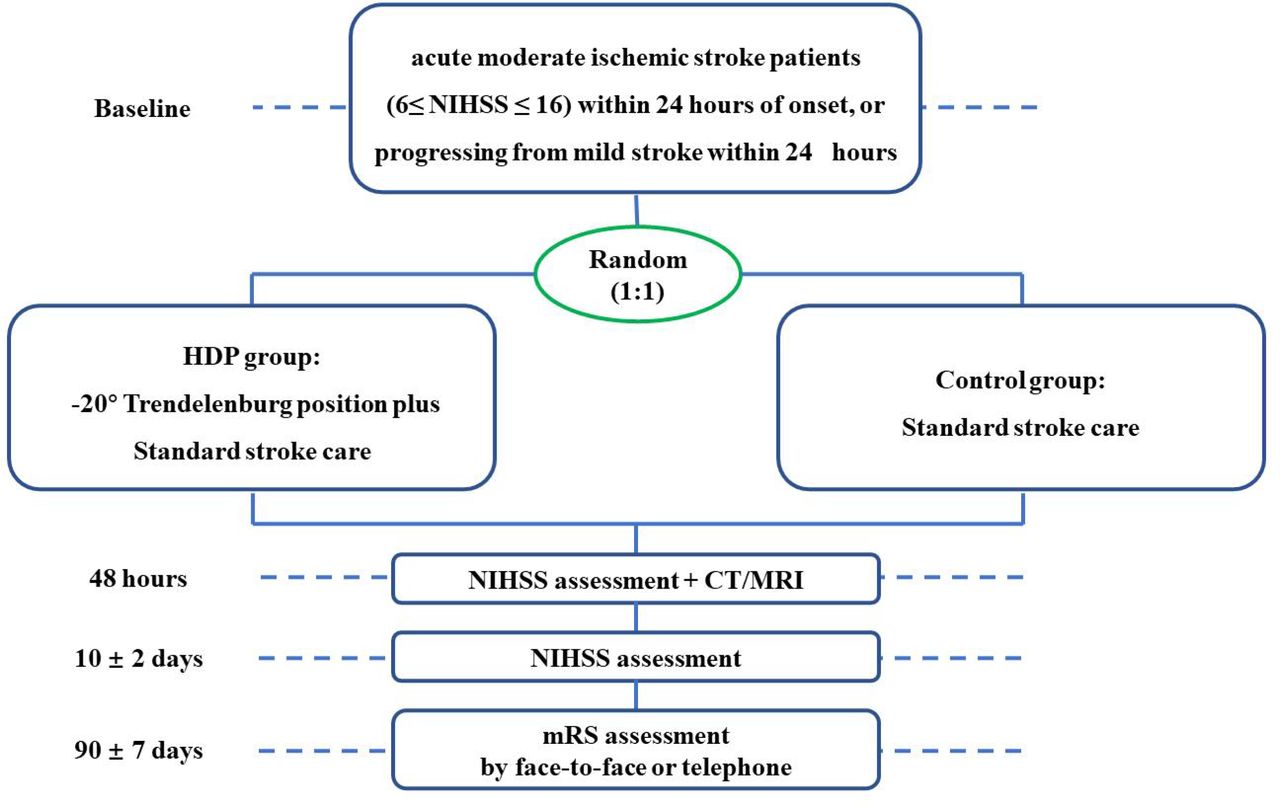
As shown in figure 1, patients are randomised 1:1 into the HDP group or control group by using a central and computerised random sequence generation stratified by centre. Consistent with the HOPES 2 trial,25 in the HDP group, patients will be positioned to −20° Trendelenburg position from 8:00 to 22:00 within the first 24 hours after randomisation. During this period, they are instructed to report any discomfort. If this position is not tolerated by the patient, they are slowly repositioned to a horizontal level for 10–30 min, followed by a return to −20°. Repeated position adjustments could be made during HDP intervention. After 24 hours, the patient is positioned at a −20° Trendelenburg for 1–1.5 hours three times a day, 9:00–11:00, 15:00–17:00 and 20:00–22:00, respectively. The treatment will continue for 10 days. During HDP, the patient can be placed in the side-lying position with −20° Trendelenburg if local investigators suspect a high risk of aspiration. In addition, all patients in the intervention arm will receive standard medical care as per national stroke guidelines.7 The control group patients will receive standard medical care in compliance with national guidelines for AIS without any intervention of head position (supine or sitting position to be determined by local investigator).7

Study flowchart. HDP, head-down position; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale.
Outcomes
The primary endpoint is favourable functional outcome, defined as modified Rankin Scale (mRS) 0–2 at 90 days.
The secondary endpoints include: excellent functional outcome (mRS score, 0–1) at 90 days; ordinal distribution of mRS at 90 days; early neurological deterioration (END), defined as more than 4-point increase in NIHSS within 48±12 hours, but not due to intracerebral haemorrhage; early neurological improvement (ENI), defined as more than 4-point decrease in NIHSS within 48±12 hours; change in NIHSS Score from baseline at 48±12 hours and 10±2 days; change in infarct volume from baseline at 48±12 hours; new stroke or other vascular event(s) within 90±7 days; all-cause mortality within 90±7 days.
The exploratory endpoints include: change in cortical oxygen saturation determined by near infrared spectroscopy at 24±8 hours and 48±12 hours; change in serum biomarkers at 48±12 hours and 10±2 days compared with baseline.
In agreement with HOPES 2,25 the safety endpoints include any adverse event (AE) or serious AE during HDP, such as patient fear, headache, anxiety, intracranial haemorrhage (European Cooperative Acute Stroke Study [ECASS] definition),26 cardiopulmonary events and pneumonia,27 which were not present at the beginning of the study.
Follow-up procedure
All patients will be visited at 48±12 hours, 10±2 days and 90±7 days after randomisation (table 1). We will record demographic data, laboratory results, neuroimaging data and neurological scoring such as NIHSS and mRS at baseline; repeat non-contrast CT or MRI at 48 hours and NIHSS scoring at 48 hours and 10 days; assess mRS at 90 days. All clinical evaluations, including NIHSS and mRS will be performed by qualified investigators in accordance with standardised protocol brochures in each site. The primary efficacy outcome (90-day mRS) is assessed by trained and certified investigators without knowledge of randomised treatment assignment at each site, either in person or by telephone interview (if in person interview is impossible). The investigators will record concomitant medications and AEs within 90 days after randomisation in detail, which will be judicated by certified assessors. The study period is estimated to be approximately 24 months.
Timing of all procedures in Head dOwn-Position for acutE moderate ischaemic Stroke with large artery atherosclerosis(HOPES 3)
Quality control
The data and safety monitoring committee (DSMC) will conduct data verification for safety every 6 months in this trial. After finishing follow-up of 50% of the participants, an interim analysis will be conducted by an independent statistician of the DSMC who will not be in the management of the trial. The main purpose of the stopping is to protect the patients’ rights and interests and to avoid unwanted financial losses. The DSMC has the right to terminate the study unconditionally, if there is a statistically significant difference in the efficacy and/or safety of one therapy compared with another. Neuroimaging data will be collected centrally and analysed by two independent neuroradiologists.
Data management and monitoring
All patient’s data will be recorded on MedSci (http://HOPES3.medsci.cn), which is able to store the patient case report form. The enrolled participants will be randomised in a 1:1 ratio into either the HDP or control group. Data will be downloaded from MedSci and statistically analysed by dedicated staff. An independent DSMC is set up to assure continuous monitoring of data safety, for example, haemorrhagic events and other AEs. Stopping or sample size modification rule will be prespecified by the DSMC. Based on the results of the analysis, the DSMC will be able to recommend sample size adjustments or early termination of the study to the steering committee of the HOPES 3 trial.
AE monitoring
An AE refers to any adverse medical event that occurs during the trial. All information regarding AEs will be documented on the AE page(s) of the case report, a further determination will be made by the principal investigator as to whether the unexpected AE is related to the HDP treatment.
Sample size estimates
According to our recent HOPES 2 trial,25 the prevalence of favourable functional outcome at 90 days (mRS 0–2) was 50% in the control group and 65.2% in the HDP group, with a 15.2% absolute difference. An absolute 12% increase in primary outcome in the HDP group is conservatively estimated, which translates into primary outcome of 62% in HDP group. A one-sided test with a power of 80% and α set at 0.025 calculated a sample size of 540 patients to test the hypothesis of superiority. The sample size is readjusted to 600 patients given a loss to follow-up rate of 10% and alpha consumption by interim analysis (O’Brien-Fleming method). This study will therefore include 600 patients, 300 in each group.
Statistical analysis
An intention-to-treat analysis is applied to determine the treatment effect between two groups. Normally distributed data will be expressed as mean±SD, and non-normally distributed data will be expressed as median and IQR. For binary outcomes including favourable functional outcome, excellent functional outcome, ENI, END and occurrence of all-cause death in 90 days, treatment effects will be analysed using binary logistic regression. Ordinal logistic regression will be used to analyse mRS distribution at 90 days between treatment groups. A general linear model will be used to analyse change in NIHSS Score or infarct volume between treatment groups, while Cox regression for time to event of stroke recurrence and other vascular events. All data are analysed with SPSS V.23.0 Software. Statistical significance will be achieved if the p value is <0.05.
The primary outcome will further be stratified by age (<60 years vs ≥60 years), sex (female vs male), history of diabetes (yes vs no), history of hypertension (yes vs no), baseline systolic blood pressure (>140 mm Hg vs ≤140 mm Hg), location of index vessel (internal carotid artery vs middle cerebral artery), NIHSS Score at randomisation (6–10 vs 11–16), onset to randomisation time (<12 hours vs ≥12 hours), progression to moderate neurological deficit due to END (yes vs no), degree of responsible vessel stenosis (moderate stenosis vs severe stenosis vs occlusion) and stroke mechanism (artery-to-artery embolism vs perforator infarct vs hypoperfusion). Differences in primary outcome in above-mentioned subgroups will be evaluated by detecting the interaction effect of the prespecified baseline variable on the primary outcome.
Study organisation and funding
The trial steering committee (TSC), made up of external scientific advisors, will regularly oversee the study and data. The TSC will host teleconference or physical meetings every 6 months to provide recommendations on the study. The trial is initiated and supported by the Cerebrovascular Disease Collaboration & Innovation Alliance of Liaoning.
Current status
At the initial submission of this paper, the patients have not yet to be recruited. Enrolment will remain open until the complete sample size is attained, which is anticipated to be in June 2025 at the latest.
Discussion
Based on the promising results of our phase 2 HOPES 2 study,25 HOPES 3 is designed to investigate the efficacy and safety of the HDP in acute moderate ischaemic stroke patients with LAA aetiology. As the first phase 3 study, the HOPES 3 trial has several distinct characteristics from prior studies.
First, the HDP at −20° is adopted in this study based on our phase 2 trial,25 while a horizontal supine versus sitting position was used in prior studies.1–4 9 10 The HDP is used in this trial, because the HDP may enhance cerebral blood flow and increase cerebral perfusion compared with the supine or sitting position due to the force of gravity,17 28 which was further supported by several animal19–22 and clinical23 24 studies, including the phase 2 HOPES 2 trial.25 Second, acute anterior circulation moderate ischaemic stroke patients (NIHSS: 6–16) with probable LAA aetiology are enrolled in this trial, while the HeadPoST study did not restrict inclusion by neurological deficit severity or stroke aetiology. We contend that stroke patients with moderate neurological deficit and LAA aetiology would be the target population most likely to benefit from HDP, given that hypoperfusion mechanisms dominate in this population who are at risk for recurrent events.29–31 Third, we implement different head position interventions over time, given that a longer duration of HDP intervention may result in more benefit of improved cerebral perfusion,25 while there may be the presence of a long-lasting penumbra in this population.32
We have to admit two potential limitations in the current study. One is the lack of an independent core lab auditing the imaging, although neuroimaging will be collected centrally and interpreted by two independent neuroradiologists. Another is a concern about the HDP protocol including non-standardisation of HDP duration within the first 24 hours given the potential risk as well as the arbitrary HDP after 24 hours.
In this trial, patients who had a posterior circulation stroke will be ruled out. One concern for this exclusion is because of the high risk of aspiration pneumonia due to active nausea and vomiting, which is common in this population. Another concern is the high probability of change of neurological deficit in this population, which may disrupt the effect of HDP.
Conclusion
The results of HOPES 3 will provide evidence for the potential benefit of the HDP in acute anterior circulation moderate ischaemic stroke patients with LAA within 24 hours of onset or in patients with progression from mild neurological deficit within 24 hours.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. This study was approved by the institutional review board of General Hospital of Northern Theater Command (Y (2023) 148). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to the steering committee and iDSMC for their contributions to this study.
Footnotes
Twitter @NguyenThanhMD
Contributors XL and ZG wrote the first draft of the manuscript. LW, YW and TN critically revised the manuscript. YY and H-SC designed the study and critically revised the manuscript. All the authors have carefully read and approved the article.
Funding The work was supported by grants from the Science and Technology Project Plan of Liaoning province (2022JH2/101500020).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note H-SC will take full responsibility for the article, including for the accuracy and appropriateness of the reference list.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}