

Abstract
Background Medical complications strongly affected the mortality of patients with stroke. However, only limited research has studied the effect of in-hospital medical complications on the mortality of patients with spontaneous intracerebral haemorrhage (ICH) globally. Using the China National Stroke Registry, the effect was prospectively and systematically investigated in patients with spontaneous ICH during their hospitalisation, at 3, 6 and 12 months after disease onset.
Methods This study collected data on patients over 18 years old with spontaneous ICH from 132 Chinese clinical centres across 32 provinces and four municipalities (Hong Kong included), from September 2007 to August 2008. Data on patient complications, death and other information were acquired through paper-based registry forms. Using multivariable logistic regression, the association of medical complications with stroke outcomes was evaluated.
Results Of 3255 patients with spontaneous ICH, 878 (26.97%) had in-hospital medical complications. In-hospital medical complications were independent risk factors for death during the hospitalisation (adjusted OR 4.41, 95% CI 3.18 to 6.12), at 3 months (adjusted OR 2.18, 95% CI 1.70 to 2.80), 6 months (adjusted OR 1.84, 95% CI 1.45 to 2.34) and 12 months (adjusted OR 1.59, 95% CI 1.26 to 2.01) after spontaneous ICH.
Conclusion The results revealed that the short-term and long-term mortality of patients with spontaneous ICH in China was significantly associated with their in-hospital medical complications.
Introduction
Spontaneous intracerebral haemorrhage (ICH) is strongly related to the increased rate of mortality and long-term disability worldwide.1–3 ICH accounts for 20%–30% of stroke in Asia.4 5 The overall annual incidence of ICH is about 25 per 100 000 persons.6 Previous studies suggested that approximately 40% of patients with ICH died within 3 months following a stroke.7–9 In addition, previous studies demonstrated that increased mortality and disability of patients who had a stroke were associated with the in-hospital medical complications.10–16 This association has been confirmed in the China National Stroke Registry (CNSR) cohort.17–19 However, only limited studies investigated the effect of in-hospital medical complications on the mortality of patients with spontaneous ICH worldwide. We therefore prospectively analysed a cohort of 3255 patients with spontaneous ICH in CNSR and investigated whether in-hospital medical complications affected risk of mortality of patients during hospitalisation, at 3, 6 and 12 months after stroke onset.
Methods
Data collection and study population
The CNSR is a national, multicentre, prospective observational study designed to investigate patient characteristics, the stroke care system, risk factors and outcomes of patients with acute stroke in China. Additional details regarding study design have been presented previously.20 In general, this prospective registry study enrolled patients with acute stroke, including acute ischaemic stroke, ICH, subarachnoid haemorrhage and transient ischaemic attack (TIA). Patients with spontaneous ICH were included in this study. Patients were excluded if they had an ischaemic stroke, subarachnoid haemorrhage, secondary haemorrhage, or TIA and were lost to follow-up. Patient data were collected at baseline, discharge and at 3, 6 and 12 months after the index event. At baseline, a trained investigator interviewed and evaluated each patient and recorded their demographic information, medical history, family history of stroke, baseline National Institutes of Health Stroke Scale (NIHSS) scores, Glasgow Coma Scale (GCS) scores at admission, haematoma volume at admission, haematoma location at admission and other clinical characteristics. The baseline NIHSS score21 and GCS score22 were used to determine the baseline severity of neurological impairment. Patients’ complications and other related information were recorded during their hospitalisation. Usually, data for the follow-up were obtained from the patients; in some cases, the information was obtained from their caregiver or surrogates. In this study, all patients with ICH were divided into two groups: those presented with in-hospital medical complications and those without complications.
Definition of medical complications
In-hospital medical complications were defined as non-neurological complications which occurred during hospitalisation and needed intervention, including pneumonia, decubitus ulcer, gastrointestinal bleeding, deep vein thrombosis and pulmonary embolism, as recorded in the paper-based registry forms. The diagnostic criteria for in-hospital medical complications were explicitly defined to all participating centres. In general, pneumonia was diagnosed with the following criteria: fever, chest symptoms, coarse breathing or crackling sounds in the chest, and was confirmed by a chest X-ray. Deep vein thrombosis was diagnosed if there was: any occurrence swelling in the legs, redness, warmth, and pain, and presence of a deep vein thrombosis by venous Doppler, but cellulitis or infection of the leg had been ruled out. Pulmonary embolism was diagnosed according to the following criteria: chest pain and shortness of breath, sinus tachycardia (heart rate >100 beats per minute) as determined by ECG. Urinary tract infections were defined as having: pain or burning during urination, the urge to urinate, cloudy urine and abnormal counts of white and red cells in urinalysis. Gastrointestinal bleeding was defined as having: coffee ground emesis, haematemesis, blood in the nasogastric tube, melena or blood in the rectum. Decubitus ulcer was defined as a skin sore caused by pressure from prolonged lying in bed during hospitalisation.
Ascertainment of outcomes
In this analysis, the death of a patient was considered a clinical outcome. The outcomes of interest were modified Rankin Scale 6 scores from in-hospital duration to 12-month follow-up. The clinical outcomes of all subjects were assessed by telephone follow-up at 3, 6 and 12 months.
Statistical analysis
Categorical variables were presented as numerical proportions, and continuous variables were presented as means with SD or medians with IQR. Differences between subjects with and without in-hospital complications were tested using a Student’s t-test for continuous variables and the χ2 test for categorical variables. To determine the associations between in-hospital medical complications and mortality in patients with spontaneous ICH, univariate logistic regression analyses and multivariate logistic regression analyses were conducted and expressed as unadjusted or adjusted ORs with their corresponding 95% CIs. Multivariate logistic regression analyses were performed and adjusted for potential covariates including sex, age, NIHSS at baseline and GCS scores, haematoma volume, haematoma location, diabetes mellitus, hypertension, hyperlipidaemia, history of coronary heart disease (CHD), history of TIA, family history of stroke, atrial fibrillation (AF), heavy alcohol intake, current smoking status, dysphagia, anticoagulant treatment, thrombolytic treatment and health insurance type. Missing values were treated as the most categories or categories based on clinical perspectives. For data analysis, SAS V.9.4 statistical software (SAS Institute) was used. A two-tailed probability value <0.05 is considered to be statistically significant.
Standard protocol approvals and patient consents
Written informed consent was obtained from all participants or their surrogates.
Data availability
Only anonymised data would be shared upon request from the corresponding author.
Results
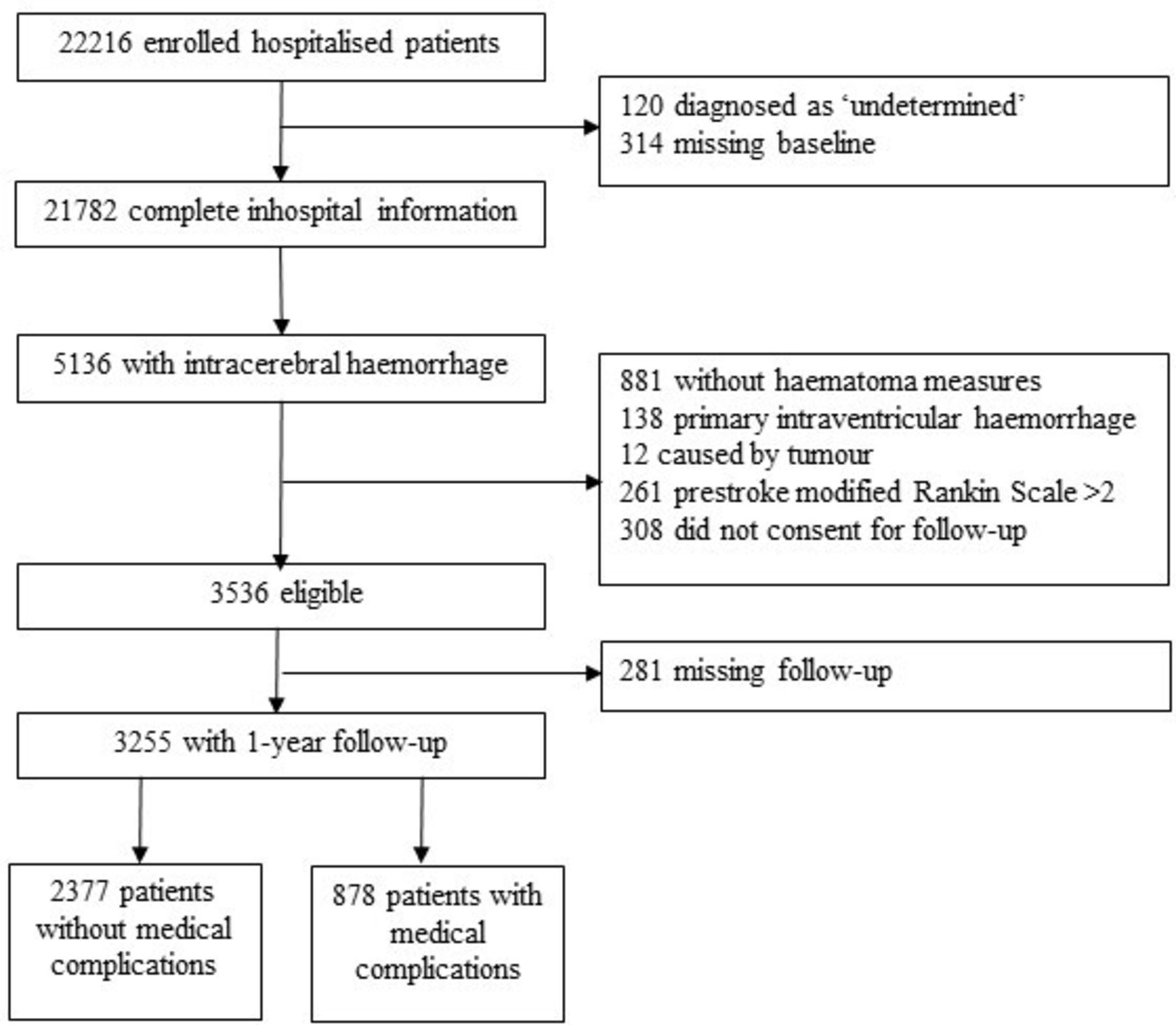
This study included 5136 patients with spontaneous ICH. We excluded 1600 individuals with primary ICH (138 patients), ICH of other causes (1462 patients) and those lost to follow-up (281 patients). Finally, 3255 subjects with initial ICH participated until the conclusion of the study (figure 1). The in-hospital prevalence of pneumonia, urinary tract infection, gastrointestinal bleeding, decubitus ulcer, deep vein thrombosis and pulmonary embolism was 17.97%, 5.96%, 5.50%, 0.95%, 0.68% and 0.34%, respectively. Of 3255 patients, 878 (26.97%) had at least one in-hospital medical complication.

Flow diagram of the study population.
The baseline characteristics of enrolled participants are listed in table 1. The study population was 38.71% female, and the mean age at onset was 62±13 years. Compared with patients without in-hospital medical complications, those with complications were significantly older, had a history of stroke, had higher NIHSS scores but lower GCS scores, had a larger haematoma volume, had higher proportions of being on antihypertension and hypoglycaemic treatment but lower use of lipid-lowering treatment. Additionally, more patients with in-hospital complications had brainstem or lobar haemorrhage. No significant differences were found in the proportion of hypertension, hyperlipidaemia, diabetes mellitus, history of TIA, history of AF, antiplatelet treatment and anticoagulant treatment.
Baseline clinical characteristics and outcomes of the study patients with intracerebral haemorrhage
The clinical outcomes of this study during hospitalisation, at 3, 6 and 12 months after spontaneous ICH were also demonstrated in table 1. The rate of mortality during the hospitalisation, at 3, 6 and 12 months after spontaneous ICH was 9.12% (297 patients), 19.97% (650 patients), 22.49% (732 patients) and 26.11% (850 patients), respectively. At all time points, the rate of death was notably higher in patients with complications than those without complications.
The univariate logistic regression analyses showed that in-hospital medical complications were significantly associated with death during hospitalisation, at 3, 6 or/and 12 months after spontaneous ICH (table 2). The multivariate logistic regression analyses showed that pneumonia was associated with a greater risk of death during hospitalisation, at 3 and 6 months after ICH; gastrointestinal bleeding was significantly associated with death at 12 months after ICH. The findings were adjusted for potential covariates including age, sex, baseline NIHSS and GCS scores, haematoma volume, haematoma location, hypertension, diabetes mellitus, hyperlipidaemia, history of TIA, history of CHD, family history of stroke, AF, current smoking status, dysphagia, heavy alcohol intake, anticoagulant treatment, thrombolytic treatment and types of health insurance (table 2).
Unadjusted and adjusted ORs for medical complications in relation to the mortality of patients with ICH during hospitalisation, and at 3 months, 6 months and 1 year
The unadjusted ORs of death were approximately 5.3-fold, 4.1-fold, 3.8-fold and 3.5-fold greater in patients with complication(s) when compared with those without complications during hospitalisation, at 3, 6 and 12 months, respectively. The adjusted ORs of death were approximately 4.4-fold, 2.2-fold, 2.0-fold and 1.9-fold greater in participants with complications when compared with those without complications during hospitalisation, at 3, 6 and 12 months, respectively (table 3).
Unadjusted and adjusted ORs of having one or more medical complications during hospitalisation for death in patients at various time points following intracerebral haemorrhage
Discussion
The CNSR is a nationwide prospective stroke registry that enrols high numbers of patients who had a stroke throughout China. In this prospective cohort study, patients with spontaneous ICH from the CNSR were included, and the impact of in-hospital medical complications on the mortality of participants was analysed. The study found that in-hospital medical complications were associated with a higher risk of death in patients with spontaneous ICH in the 12 months following a stroke.
In this study, a total of 878 patients (26.97%) had medical complications during their hospitalisation. We found that the frequencies of pneumonia, urinary tract infection, gastrointestinal bleeding, decubitus ulcer, deep vein thrombosis and pulmonary embolism during hospitalisation were 17.97%, 5.96%, 5.50%, 0.95%, 0.68% and 0.34%, respectively. The most common complication was pneumonia, followed by urinary tract infection, then gastrointestinal bleeding. The previously reported incidence of pneumonia varied from 3.5% to 31.1% in patients with only spontaneous ICH.9 23–25 Lord et al presented a retrospective cohort of 3550 readmitted patients from non-federal acute care hospitals in California with a primary diagnosis of ICH between 2006 and 2010 and found 124 (3.5%) patients with pneumonia.23 Nzwalo et al reported a retrospective cohort of 549 spontaneous ICH from south Portugal and found 171 (31.1%) patients with in-hospital pneumonia.9 Lindner et al prospectively collected a cohort of 229 patients with non-traumatic ICH from the neurocritical care unit (NICU) of a tertiary care hospital in Austria between 2011 and 2016.25 They found 64 (28%) patients with pneumonia, which was the most common complication in the study. Morotti et al retrospectively analysed a cohort of 2014 patients with spontaneous ICH from a single academic hospital from 1994 to 2015.24 They also confirmed that pneumonia was the most common complication, and the incidence of pneumonia was 18.4%. Our study showed similar results, confirming poor outcome of patients with spontaneous ICH was associated with in-hospital medical complications.
Previous studies mainly focused on 30-day and 3-month risk of death and its association with the medical complications.7–9 23 26 In CNSR, the risk of death was increased because of the medical complication(s) during hospitalisation, at 3, 6 and 12 months following spontaneous ICH, expanded the duration of observations. Until now, this study was the largest prospective study on the relationship between in-hospital medical complications and death of patients with spontaneous ICH.
Prevention of in-hospital medical complications is key to reduce future death in patients following spontaneous ICH. Such prevention is especially important for patients with vulnerable age, a history of stroke, a higher NIHSS score, a lower GCS score and a larger haematoma volume, who are more likely to have in-hospital medical complications.
Our study had limitations. Only six types of complications were included. In addition, information on the treatment of medical complications was not collected, which may affect the mortality. Finally, all recruited hospitals or centres were from urban areas in China; thus, our results may not be able to represent all levels of hospital care in China.
In conclusion, in patients with spontaneous ICH, pneumonia was the most common in-hospital medical complication. All six in-hospital medical complications were significantly associated with the 12-month mortality in patients with spontaneous ICH. Aggressive treatment and prevention of complications in these patients will prevent future death. Future studies on the mechanisms of complications affecting stroke outcomes are still needed.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data are available from XZ, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China. Tel: +86-10-59978350. Fax: +86-1059973383. Email address: zxq@vip.163.com. The data reuse is permitted under the corresponding author's permission.
Ethics statements
Ethics approval
Institutional Review Board (IRB) of Beijing Tiantan Hospital, Capital Medical University.
Acknowledgments
The authors would like to thank the patients who participated in this CNSR study and all investigators, nurses and imaging and laboratory staff in all participating centres. The details of the study design have been published previously.
Footnotes
Contributors Conception and design: YW (Yongjun Wang), XZ, PW, YZ. Administrative support: XZ, YW (Yilong Wang), LL, PW, RJ, ZY. Provision of study materials or patients: all authors. Collection and assembly of data: AW. Data analysis and interpretation: AW. Manuscript writing: all authors. Final approval of manuscript: all authors.
Funding This work was supported by grants from the National Key R&D Program of China (2016YFC0901002, 2017YFC1310901, 2018YFC1312903), grants from Beijing Municipal Science and Technology Commission (D171100003017002) and grants from the National Science and Technology Major Project (2017Z×09304018).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}