

Abstract
Background Prehospital delay in acute ischaemic stroke (AIS) remains prevalent in China. We aimed to assess the status of the onset-to-door time (ODT) in AIS and analyse its influencing factors.
Methods Data were collected from a prospective multicentre hospital-based registry (China National Cerebrovascular Disease Prevention and Control Project Management Special Database) of patients with AIS involving 21 hospitals across different economic and geographical regions in China in 2022. The Mann-Whitney U test or t-test was used for between-group comparisons. Factors influencing ODT ≤3 hours were analysed using a binary logistic regression model.
Results Of the included 12 484 patients (attended middle school or below, 69.2%), females had a higher illiteracy rate (13.1%) than males (4.8%); 94.8% were living with others at illness onset; 22.5% of patients/family members were aware of the stroke emergency map (SEM, but only 7.3% were transported by SEM; 76.8% lived within 20 km of the first visited hospital. Significant differences occurred in modes of arrival at hospitals among cities of different sizes (χ²=74.882, p<0.001). Being in a medium-sized (OR 0.65, 95% CI 0.50 to 0.86); large (OR 0.61, 95% CI 0.47 to 0.79) or extralarge city (OR 0.60, 95% CI 0.46 to 0.78); experiencing cardiogenic embolism (OR 0.65, 95% CI 0.50 to 0.86) or stroke of undetermined aetiology (OR 0.69, 95% CI 0.52 to 0.92); stroke onset between 18:00 and 23:59 (OR 0.71, 95% CI 0.60 to 0.85); distance <20 km from onset location to the hospital (OR 0.47, 95% CI 0.41 to 0.54); being transported by SEM (OR 0.31, 95% CI 0.26 to 0.36) and having initial National Institutes of Health Stroke Scale scores of 5–15 (OR 0.63, 95% CI 0.57 to 0.71) or 16–42 (OR 0.32, 95% CI 0.27 to 0.39) were independent factors favouring ODT ≤3 hours. Conversely, being transferred between hospitals during transportation (OR 3.31, 95% CI 2.66 to 4.14); experiencing wake-up stroke (OR 2.00, 95% CI 1.67 to 2.38); symptom-onset including dizziness (OR 1.28, 95% CI 1.10 to 1.47) and prestroke modified Rankin scale (mRS) score of 2–3 (OR 1.58, 95% CI 1.30 to 1.92) or 4–5 (OR 1.48, 95% CI 1.02 to 2.15) tended to indicate ODT >3 hours.
Conclusions Urban scale, stroke type, onset time, distance from initial location to the first hospital visit, transportation method, stroke symptoms, prestroke mRS score and stroke severity significantly influenced prehospital delay. Our findings can facilitate the development of targeted policies.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prehospital delay in acute ischaemic stroke is a serious public health concern and is prevalent in developing countries.
WHAT THIS STUDY ADDS
To our knowledge, this is currently the largest multicentre prospective study in China on the status and influencing factors of onset-to-door time, covering cities with different economic and cultural characteristics, making the research results broadly representative. Our findings reveal that urban scale, stroke type, onset time, distance from the initial location to the first hospital visit, transportation method, stroke symptoms, prestroke modified Rankin scale score and stroke severity are significant factors influencing prehospital delay.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study provides valuable guidance for stroke emergency treatment, which can help develop targeted policies, improve treatment outcomes and enhance patient prognosis.
Background
Acute ischaemic stroke (AIS), a significant health concern, affects >800 000 adults in the USA annually.1 Prehospital delay in AIS—the duration between the recognition of stroke-related symptoms and patient arrival at the emergency department (ED)2—significantly affects the timely administration of reperfusion therapies and subsequent patient outcomes.3 However, multicentre, large-sample prospective studies concerning the current prehospital delay situation in China are lacking.
Globally, stroke was the second-leading cause of death and the third-leading cause of death and disability in 2019. The annual stroke incidences and mortality have increased substantially.4 Ischaemic stroke accounts for approximately 4/5th of all stroke cases.5 Intravenous thrombolysis (IVT) in AIS effectively improves neurological outcomes in patients with stroke who have moderate-to-severe neurological deficits.6 The sooner IVT is administered, the greater its benefits.7 An onset-to-door time (ODT) ≤4.5 hours is crucial for better clinical outcomes.8 Despite the availability of thrombolytic and endovascular therapies for AIS, due to prehospital delay, in-hospital delays and hesitancy in treating or receiving treatment, <1%–8% of patients with stroke receive IVT.9 The efforts to decrease door-to-needle times in stroke treatment have yielded positive advancements. However, prehospital delays are common among stroke patients in Chinese communities, with only 24.8% of patients being transferred to the ED or hospital within 2 hours.10 Prehospital delays are the main factor preventing patients from receiving IVT. The median ODT and proportion of patients with stroke arriving within the crucial 3-hour window have shown minimal progress over the last 20 years.3 Prehospital delays are influenced by various factors, including patient behaviour, decision-making processes and healthcare system inefficiencies.11 Major factors influencing prehospital time include emergency medical pathways, stroke symptoms, patient and bystander behaviours, patient health characteristics, and awareness of stroke treatment.3 Prehospital delay occurs at different phases—time from symptom onset to decision to seek medical attention, from decision to seek medical attention to the first medical contact, and from the first medical contact to arrival at the ED.12 Regional variations in prehospital delay may be significant, and identifying the factors associated with delayed hospital arrival may uncover potential intervention targets for decreasing prehospital delays and enhancing access to time-critical reperfusion therapy.
Methods
Study design
This large-scale, prospective, multicentre, hospital-based registry study collected data from patients with AIS (China National Cerebrovascular Disease Prevention and Control Project Management Special Database) who were admitted to 21 hospitals across different economic and geographic regions in China from 1 January 2022 to 31 October 2022. The 21 hospitals were geographically distributed across China as follows: Northeast Region: Shenyang, Chaoyang; North China Region: Handan; East China Region: Bengbu, Linyi, Yantai, Suzhou, Hangzhou; Central China Region: Wuhan, Jiaozuo, Yichun; South China Region: Heyuan, Shenzhen, Nanning, Wuzhou, Yunfu; Northwest Region: Baiyin, Xi'an and Southwest Region: Luzhou, Yibin. All participating hospitals were level I tertiary hospitals and qualified to perform IVT and endovascular thrombectomy. All the relevant cities also released stroke emergency maps (SEM).13
Study participants
Patients aged ≥18 years, diagnosed with AIS and with stroke onset ≤7 days before admission were included. Those who were diagnosed with transient ischaemic attack, in-hospital AIS, cancer-related stroke, iatrogenic AIS or cerebral venous sinus thrombosis; with a life expectancy of <3 months; and diagnosed with severe mental disorders, dementia, or severe heart, liver, kidney, or lung failure were excluded. AIS was diagnosed based on findings from head CT or MRI and diagnostic criteria in relevant guidelines.10 The stroke subtype was based on the Trial of Org 10 172 in the Acute Stroke Treatment (TOAST) classification.14
Patient and public involvement
We conducted a needs analysis by gathering concerns from patients and the public about AIS through interviews. In designing the case report forms, we invited several patients and their families to participate, ensuring that the survey content accurately reflected their experiences and perspectives. During the research implementation phase, we encouraged participating hospitals and patients to provide feedback throughout the data collection process.
In our research, the research question and outcome measures were developed by prioritising patient experiences. An extensive literature review to identify factors related to hospital delays in AIS was first performed. To ensure our research questions reflected real patient experiences, we conducted communication with patients. From the feedback, we reassessed, ultimately determining the research indicators.
We developed a patient recruitment strategy by collaborating with the subcentres to effectively recruit eligible patients with AIS. Throughout the study, we facilitated communication between the medical team and patients, ensuring participants had a comfortable experience and understanding their rights and obligations. Additionally, during the data collection and analysis phase, we established a feedback mechanism that allowed patients and their families to provide comments and suggestions.
This observational research project primarily focused on observing and recording the healthcare-seeking process of patients with AIS. The patients did not receive any interventions; hence, issues related to the burden of intervention and participation time were not addressed. To disseminate our research findings to participating patients and the broader patient community, we plan to release these results soon after completing the research. We will use a variety of formats for dissemination, including concise summaries, infographics, patient manuals and online webinars.
Data collection and auditing
Data collection process
Case registration: A specialised online stroke case registration system was used with all eligible patients registered by dedicated stroke teams at the hospitals.
Collection methods
Standardised questionnaire: A validated standardised questionnaire was used to collect basic patient information, onset time, symptoms and other related data. Trained healthcare professionals filled out the questionnaire.
Interviews: Within 24 hours of patient admission, the research team interviewed patients and their families to gather information regarding symptoms before onset, location and mode of transportation to the hospital.
Data review
Review standards: Completeness: All registered cases must include all key data items.
Consistency: Answers recorded in the questionnaire were cross-checked with data in electronic medical records to ensure information accuracy.
Validity: Data were examined for outliers or logical inconsistencies.
(2) Outliers included:
Timing errors: The recorded onset time of illness or medical visit exceeded reasonable limits.
Location data anomalies: Errors in inputting patients’ addresses, leading to unreasonable geographical placements (eg, in the ocean).
Incorrect demographic information.
Logically inconsistent clinical assessment results, such as inaccurate National Institutes of Health Stroke Scale (NIHSS) scores resulting in unusually high or low ratings.
Duplicate entries of the same patient’s data.
Personnel and timing for review
Review team: Data review was conducted by a fixed team of researchers with clinical backgrounds and data management experience. All review team personnel received relevant training and were familiar with review standards and procedures.
Review timeline: Review period: Data review was conducted within 1 month after completing data collection. Phased review: During data collection, the research team performed preliminary data reviews regularly.
ODT calculation
ODT was defined as the time from stroke symptom onset to admission to the hospital ED or outpatient clinic. We typically documented the precise time when the patient or witness first noticed stroke symptoms, such as sudden hemiplegia and speech difficulties. When the symptom-onset time was unclear, the following methods were used: (a) When the patient awoke with symptoms, the time before sleep when the last symptom-free period was confirmed was considered the symptom-onset time.15 16 (b) When the exact symptom-onset time could not be determined, the time at the last confirmed symptom-free period was considered the symptom-onset time.15 16 Subsequently, the outpatient department or ED arrival time, specifically at the triage entrance,17 was documented.
Defining city size in China
A megacity, super-large city, large city, medium-sized city and small city were defined as having a population of over 10 million, 5–10 million, 1–5 million, between 500 000 and 1 million, and <500 000, respectively.18
Study variables and groups
The study variables included age, educational level, residence status, distance between onset location and first-visit hospital, method of arrival, interhospital transfer, wake-up stroke, preonset modified Rankin scale (mRS) score, stroke severity after onset according to the NIHSS score (5–15, moderate; 16–42, severe19), TOAST classification of cerebral infarction, urban scale, first AIS symptom and stroke onset time. Division of patients based on ODT is crucial for stratifying stroke care and predicting outcomes.20 Accordingly, patients with AIS were categorised into ODT ≤3 hours and ODT >3 hours groups. The modes of transportation to the hospital are categorised as self-transported, emergency medical services (EMS) and other forms. ‘Other forms’ refers to instances where patients arrived neither by their own means nor through EMS. This primarily includes situations where individuals are transported by family members or bystanders instead of seeking help themselves, such as in the case of comatose patients.
Statistical analyses
Statistical analyses were performed using R V.4.3.1 (The R Project, Vienna, Austria). Normally and non-normally distributed continuous variables are presented as mean±SD and median (IQR), respectively. Categorical variables are presented as numbers (percentages). Between-group comparisons of measurement data were conducted using the Mann-Whitney U test (non-normally distributed data) or t-test (normally distributed data); between-group count data were compared using the χ2 test. Factors influencing an ODT ≤3 hours were analysed using a binary logistic regression model. A p<0.05 was considered statistically significant.
Results
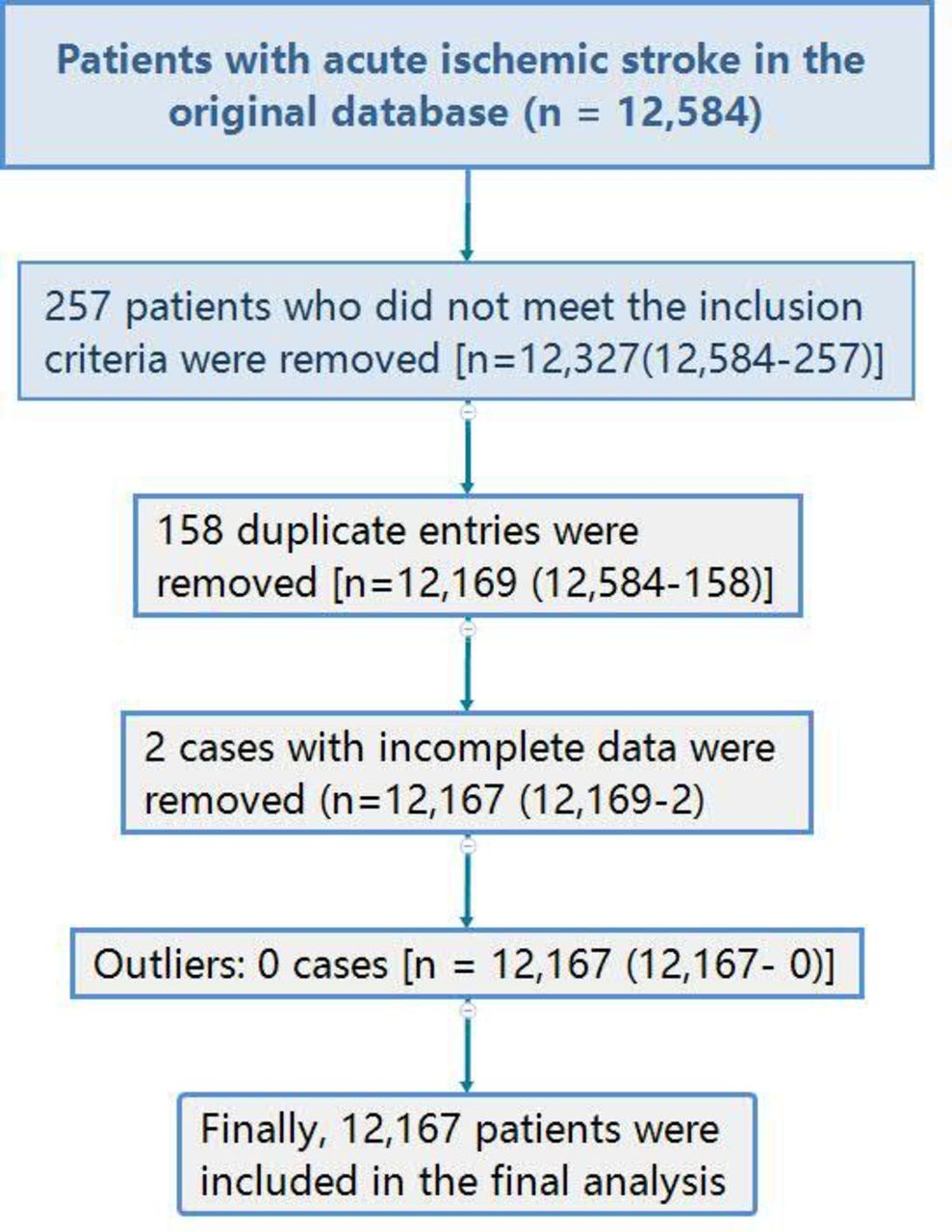
Of 12 584 included patients with AIS, those with incomplete data, who failed to meet the inclusion criteria, and outliers were excluded. Finally, 12 167 patients were included (figure 1).

Flow chart of the screening process for research subjects.
The patients had a mean age of 66.1±11.79 years, 96.3% were aged >45 years, and males were younger than females (p<0.001). Most patients (69.2%) had an education level of middle school or below. The illiteracy rate was higher among female patients (13.1%) compared with males (4.8%) (p<0.001). Nearly all patients (94.8%) were living with others at the time of illness onset; 22.5% of patients or their family members were aware of SEM and 76.8% lived within 20 km of the first hospital they visited. Only 7.3% were transported by SEM. Further details are presented in online supplemental table 1. Significant differences were found in the modes of arrival at hospitals among cities of different sizes (table 1).
Supplementary data
Pathways and number of patients with acute ischaemic stroke arriving at hospitals in cities of different sizes
Factors affecting ODT ≤3 hours
Using ODT ≤3 hours as the dependent variable, age, urban scale, residential status, patient or family awareness of SEM, TOAST classification, time of stroke onset, distance from onset location and first-visit hospital, mode of transportation to the hospital, interhospital transfer, wake-up stroke, limb weakness, dizziness, prestroke mRS score and initial NIHSS score on hospital arrival were included as independent variables in the binary logistic regression analysis. The time of stroke onset, distance from the onset location to first-visit hospital, transport to hospital by EMS, history of interhospital transfer, wake-up stroke, dizziness/vertigo as initial symptom, prestroke mRS score and initial NIHSS score after onset were independent influencing factors for ODT ≤3 hours (table 2).
Binary logistic regression analysis of factors influencing onset-to-door time ≤3 hours
Moreover, we compared the modes of arrival at the hospital and effectiveness of emergency 218 stroke treatment during and after the COVID-19 pandemic, specifically between 1 January 2022 and 31 October 2022, and 1 January 2023 and 31 October 2023 (see online supplemental table 2).
Supplementary data
Discussion
In medium-sized, large and super-large cities; cardiogenic embolism, stroke of undetermined aetiology, stroke onset between 18:00 and 23:59, distance ≤20 km from onset location to first-visit hospital, transport to hospital by EMS and initial NIHSS scores of 5–15 and 16–42 were independent factors indicating an ODT ≤3 hours. A history of interhospital transfer, wake-up stroke, dizziness/vertigo as the initial symptom and preonset mRS scores of 2–3 and 4–5 indicated an ODT >3 hours. To our knowledge, this is the largest multicentre prospective study in China on the status and influencing factors of ODT, covering cities with different economic and cultural characteristics, rendering the results broadly representative.
China’s stroke emergency response system: the ‘Green pathway’ model
The ‘Green pathway’ widely implemented in China refers to a prioritised pathway designed to accelerate the diagnosis and treatment of patients with acute stroke.21 It can be divided into two parts: prehospital (stroke transfer) and in-hospital emergency stroke treatment. The key components include (1) emergency response system, (2) in-hospital emergency teams, (3) standardised diagnosis and treatment processes, (4) rapid imaging tests and (5) data management and monitoring.
In addition, China is promoting a nationwide SEM project. This map serves as an emergency response platform that integrates geographical information systems with the distribution of medical resources.13 ‘Green pathway’ improves stroke treatment by implementing standardised treatment protocols and clinical pathways, allowing doctors to adhere to evidence-based best practices, thereby enhancing the consistency and standardisation of care, such as increasing stroke education, dysphagia screening, smoking cessation and antithrombotics at discharge.21 Significant reductions in door-to-needle times for thrombolytic therapy after implementation of the ‘Green pathway‘ led to improved functional outcomes.22 Despite significant progress, challenges remain related to insufficient awareness of strokes among residents, lack of workforce in specialised stroke teams and inadequate professional skills. Additionally, there are issues with the coordination between prehospital and in-hospital emergency responses, especially in rural and less-developed areas. Future efforts should concentrate on providing ongoing education and training for community residents, EMS providers and hospital staff; implementing standardised referral processes and establishing a data-sharing system between prehospital and in-hospital services; and improving stroke registries to facilitate research and elevate care standards.
Current situation of prehospital delay in developing countries
Prehospital delay in AIS is prevalent in developing countries. This study indicates that only around 1/5 of AIS cases involve an ODT ≤3 hours, with an average of 11.6 hours. In Shanghai, China, 30.2% of individuals arrive at the hospital within 3 hours after stroke onset.23 A 2006 study in China revealed that 25% of patients arrived within 3 hours, with a median ODT of 15 hours (IQR 2.8–51.0).24 Compared with the aforementioned, the ratio of an ODT ≤3 hours has slightly decreased, possibly influenced by the COVID-19 pandemic; however, the median ODT has slightly improved. Despite >10 years having passed, prehospital delays in China have not significantly improved. In Nepal, only 20.17% of patients arrive within the time frame for thrombolysis.25 Regarding prehospital delays, developed countries have substantially better rates than developing countries. In the USA, approximately 50% of patients with AIS arrived at the hospital within 4.5 hours.26 In Spain, 48.7% of patients experience a prehospital delay of ≤3 hours.27 Prehospital delay is more common in developing countries owing to lower levels of stroke awareness, influence of traditional beliefs, inadequate emergency response systems, heavy economic burden on residents and poor transportation conditions.25 Here, we identified further factors that influence ODT.
Urban scale and ODT
Medium-sized, large and super-large cities tend to have an ODT ≤3 hours because of the following: (1) Advanced medical resources: More medical resources, including efficient and well-developed emergency response systems and EMS services, allow for quick response and transport of patients with stroke. (2) Stroke awareness and education levels: Richer health education resources and more developed media channels facilitate wider dissemination of stroke-related knowledge information. These improve residents’ awareness of emergency treatment, making it easier to seek timely medical help.28 (3) Transportation convenience: High transportation convenience assists patients in reaching hospitals quickly.
Our study reveals that patients in the largest cities have the highest rate of self-transport to hospitals. Statistically significant differences exist in hospital arrival modes among cities of varying sizes. In major cities in China, particularly megacities, there is a well-developed public transport system, a high vehicle ownership rate, and comprehensive taxi services, including ride-hailing apps and traditional taxis. Many people in China are confident in driving themselves or taking a taxi to receive medical care, often underestimating the importance of getting to the hospital via EMS. This phenomenon is closely tied to traditional culture and social psychology, contrasting sharply with the situation in many Western developed countries.29
Stroke types and ODT
Cardiogenic embolism and stroke of undetermined aetiology tend to result in an ODT ≤3 hours, whereas wake-up stroke tends to result in an ODT >3 hours. The reasons are:
Cardiogenic embolism often has an acute onset with severe symptoms, which may prompt patients and bystanders to quickly recognise its seriousness and consequently seek medical attention promptly, shortening ODT. The higher the patient’s awareness of the importance of stroke, the shorter the delay in seeking treatment. Patients with AIS and atrial fibrillation arrive earlier at the ED.24 Decision delays represent 49% of prehospital delays, and atrial fibrillation contributes to shortened decision delays.30
Stroke of undetermined aetiology often occurs suddenly with severe symptoms. Patients may present with focal neurological deficits, convulsions, altered sensory function and aphasia,31 which may concern the patient and bystanders, prompting them to seek medical help quickly. The high prevalence of visceral infarcts in strokes of undetermined aetiology indicates that cryptogenic strokes may arise from embolic sources.32 Cardiogenic embolism is a crucial factor that motivates patients to seek prompt medical care.33
Onset time and ODT
Stroke onset between 18:00 and 23:59 typically leads to an ODT ≤3 hours. The reasons are as follows:
Bystanders present: Between 18:00 and 23:59, the patient is more likely to be accompanied by family members, colleagues or caregivers—bystander presence is associated with a shorter prehospital delay.28 These individuals can help identify abnormal symptoms and remind and assist patients in calling EMS or transporting them to the hospital, thereby reducing prehospital delay. Furthermore, adult offspring prefer a shorter delay in making a decision.27
Relatively smooth traffic: Compared with the peak traffic hours during the day, the traffic flow between 18:00 and 23:59 may be relatively smooth, shortening the travel time to the hospital and thereby reducing ODT. The study revealed that over half of delays are due to hesitation to seek EMS.34 Family member presence facilitates recognising stroke symptoms and improving patients’ decision-making in seeking medical care.
Distance from initial location to first-visit hospital and ODT
A distance ≤20 km from the onset location to the first-visit hospital tends to result in an ODT ≤3 hours, for the following reasons:
Shorter transportation time: A distance <20 km from the onset location to the hospital allows for faster arrival, reducing prehospital delay.35
Reducing interhospital transfers: A location of onset relatively close to a hospital allows patients to travel directly to the hospital and avoid transfer-related delays.
Boosting patient and family confidence: Knowledge of a nearby hospital can increase the confidence of patients and their families in seeking medical assistance, thereby reducing decision-making and action delays when stroke symptoms occur. Patients who live ≤10 km away tend to arrive at the hospital sooner.36 A distance ≤20 km between the location of symptom onset and the hospital is associated with early arrival.25 The more remote the location of stroke, the more likely the patient will experience a prehospital delay.
Stroke symptoms and ODT
Stroke that manifests primarily as dizziness/vertigo predisposes an ODT >3 hours. Dizziness, an atypical symptom of stroke, is independently associated with delayed arrival of patients. The reasons are:
Difficulty in identifying the cause: Dizziness/vertigo is a non-specific symptom caused by various factors, including vestibular dysfunction and low blood pressure. Dizziness/vertigo caused by stroke may be mistaken for other causes or attributed to a poor mental state, leading to neglecting the seriousness of the symptoms, often assuming that they will improve with rest or further observation.
Lack of awareness of stroke symptoms: People are more familiar with typical stroke symptoms (eg, limb weakness/numbness, language difficulties) than with atypical symptoms such as dizziness/vertigo; thus, dizziness as a symptom of stroke may not be promptly recognised, resulting in prehospital delays.37 Patients’ awareness of AIS symptoms significantly decreases hospital arrival delays.38
Dizziness misdiagnosis: Given the non-specific nature of dizziness, despite seeking medical attention promptly, patients may be initially misdiagnosed, leading to delayed diagnosis and treatment. On proper diagnosis, these patients might be referred to a hospital capable of treating stroke, thereby increasing the ODT.
Prestroke mRS score and ODT
Prestroke mRS scores of 2–3 and 4–5 lead to an ODT >3 hours. The mRS score reflects patients’ functional status and daily living abilities; the higher the score, the more severe the functional impairment and dependence in daily life. Patients with higher prestroke mRS scores were more likely to experience significant prehospital delays. The possible reasons include:
Difficulty in symptom recognition: Patients with higher mRS scores often have existing neurological deficits such as limb weakness or speech difficulties. Therefore, new stroke symptoms may be mistaken for worsening pre-existing deficits.
Communication barriers: Patients with higher mRS scores may have cognitive or language impairments that affect their ability to accurately express worsening symptoms or seek assistance, thus delaying the identification of stroke symptoms.
Decreased coping abilities: Patients with higher mRS scores may be highly dependent in daily life and cannot independently cope with recurrent symptoms by calling EMS or getting to the hospital by themselves, resulting in prehospital delay.
Transport barriers: Patients with higher mRS scores often have mobility issues or are bedridden, requiring specialised transportation equipment (including stretchers or wheelchairs) and workforce, complicating getting to the hospital and prolonging transportation preparation time. Caregivers may also delay decisions due to concerns about the patient’s difficulties in seeking medical care, further increasing ODT. The higher a patient’s preonset mRS score, the longer the prehospital delay.8
Severity of stroke and ODT
After stroke onset, initial NIHSS scores of 5–15 and 16–42 lead to an ODT ≤3 hours. A higher NIHSS score indicates more severe stroke and neurological deficits. Severe stroke is associated with reduced prehospital delays27 34 because of the following:
Clear and easily identifiable symptoms: Higher NIHSS scores typically indicate significant neurological deficits, such as hemiplegia, aphasia and consciousness disorders. Compared with mild symptoms, severe symptoms are more easily recognised by patients and bystanders, promoting the seeking of assistance and medical attention early. Unconsciousness at presentation accelerates presentation at the hospital.24
Enhanced crisis awareness of patients and bystanders: When faced with severe neurological deficits, patients/bystanders often realise the urgency of the situation and the need for immediate medical attention, which may prompt seeking EMS more actively. Patient awareness of stroke symptoms is vital for early hospital arrival. Bystanders also play a critical role in responding to stroke.27
Emergency response system prioritisation: When a patient or bystander calls for emergency assistance and describes severe stroke symptoms, the emergency dispatcher may assign high priority to the call. This can reduce the emergency response and arrival times at the scene, accelerate patient transfer and ultimately shorten the ODT. A lower NIHSS score is an independent predictor of late arrival.8
Existing strategies for reducing prehospital delays
Reducing prehospital delays requires various approaches, including:
Public education and awareness campaigns: Improved public awareness of AIS symptoms and the importance of early intervention can result in quicker help-seeking. The ‘FAST’ campaign for stroke awareness is a well-known example. The Stroke 1-2-0 programme in China aims to improve awareness and response to stroke symptoms.39 Population education, suggesting that educational interventions could help mitigate delays.40
Strengthening and optimising the EMS system: Using EMS has been emphasised as a key factor in reducing prehospital delay time and minimising delays to treatment on hospital admission.41 42 A well-organised regional triage and referral system is essential for reducing interhospital transfer and shortening prehospital delays.43 Optimising prehospital pathways through systems-based approaches has been suggested to reduce treatment delays and potentially enhance clinical outcomes.44 Efforts have been made to expand EMS coverage, improve work efficiency and enhance response times through better resource allocation and personnel training.
Integrated prehospital and in-hospital care: Seamless communication and coordination between prehospital and in-hospital care can reduce handover delays and facilitate timely treatment. Studies have shown that prehospital notification by EMS can reduce delays in stroke evaluation.42 The integration of prehospital and hospital care is being promoted, with protocols established for seamless transfers and handovers.
Other measures: The implementation of telemedicine allows for quicker triage and decision-making by medical professionals before the patient arrives at the hospital. The use of mobile stroke units equipped with telemedicine capabilities allows for early diagnosis and treatment.
The impact of differing emergency medical policies on EMS performance
Notably, the low rate of EMS utilisation is a significant factor that may contribute to treatment delays. Differences in emergency medical policies between developed countries and China arise from various factors, including healthcare financing, system organisation and the prioritisation of emergency care within broader health policy frameworks. Developed countries generally have more established and better-funded EMS systems. Although China has made significant progress in developing its EMS, challenges remain in system integration and resource allocation. In developed nations, emergency medicine is a recognised specialty with dedicated training programmes and standardised protocols, resulting in improved patient outcomes and resource management.45 China’s rapidly developing EMS still faces challenges, including inadequate training for personnel and a lack of standardised protocols across regions.46 Healthcare financing models significantly impact the effectiveness of EMS policies. Developed countries often employ universal healthcare models, ensuring equitable access to emergency services crucial for timely intervention.47 China’s mixed public and out-of-pocket financing system can create access barriers for vulnerable populations,47 leading to disparities in the availability and quality of emergency care compared with developed nations. Furthermore, China’s EMS has been criticised for fragmentation, with varying service quality and accessibility between urban and rural areas.46 This fragmentation results in inefficiencies and delays that negatively affect patient outcomes.
Limitations
Although we included as many factors influencing ODT as possible, we cannot exclude the potential impact of factors not covered in this study, such as comorbidities. Future studies should evaluate these additional factors. Although this study included many cities in China and AIS patients, future research should compare the differences in ODT between different ethnic groups. While we have drawn on existing literature to examine why each factor was associated with ODT, some of the associations discussed may require further validation through additional research. This study, compared with a decade ago, represents the current state of ODT in China. Furthermore, progress in ODT improvement should be consistently monitored to illustrate its time trends.
Conclusions
Prehospital delay in patients with AIS is a considerable public health issue in China, with no significant progress observed over the past decade. Patients located in medium to extralarge cities and those with cardiogenic embolism or wake-up stroke, AIS onset between 18:00 and 23:59, distance ≤20 km from onset to hospital, severe neurological deficits at onset and who are transported via EMS are more likely to reach the hospital within 3 hours. Conversely, being transferred between hospitals, experiencing a wake-up stroke, presenting with dizziness, limited daily activities or having disabilities before onset may prolong the time to hospital arrival. These findings can be used to optimise stroke emergency strategies, reduce prehospital delays, improve emergency response efficiency, provide timely treatment and enhance patient outcomes.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethics committee of the First Affiliated Hospital of Shenzhen University (No: 20200727003-FS01-XZ202103). As this is a low-risk observational study, the requirement for informed consent was waived and approved by the ethics committee.
Footnotes
YS, WQ and YYu are joint first authors.
LC and LR contributed equally.
YS, WQ and YYu contributed equally.
Contributors LC and LR developed the protocol and framework and critically reviewed and revised the manuscript. They contributed equally to this work. YS, WQ and YYu drafted the manuscript and performed the statistical analysis. They contributed equally and share the first authorship. XS, XW and FC monitored the research and gave critical comments. JZ and RX conducted the literature searching. LQ conducted follow-ups with patients. YYa, QL, XP, GH, JC, YX, WG, DG and BY collected the data. LC is the guarantor.
Funding This study was funded by Shenzhen Second People’s Hospital Clinical Research Fund of Shenzhen High-level Hospital Construction Projects (20243357001),the Shenzhen Program for Integration Prevention and Cure of Nervous System Disease (None),the Research and Promotion Project on Appropriate Intervention Techniques for High-Risk Stroke Population (GN-2020R0002), Shenzhen Clinical Research Center for Neurological Diseases (LCYSSQ 20220823091204009), Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0504800, 2023ZD0504802).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}