

Abstract
Background The Catfish stent retriever is a newly developed mechanical thrombectomy device for rapid recanalisation in emergent large vessel occlusion (ELVO) stroke. The current trial aimed to assess whether the Catfish stent retriever is non-inferior to the Solitaire stent retriever in terms of outcomes in ELVO stroke.
Methods This was a randomised, prospective, parallel-group, multicentre, open-label, non-inferiority study conducted at 18 sites in China. The primary outcome was the proportion of cases with successful recanalisation (modified thrombolysis in cerebral infarction score of 2b or 3) following the procedure. Secondary efficacy outcomes included the National Institutes of Health Stroke Scale scores at 24 hours and 7 days or discharge if earlier, time from artery puncture to successful recanalisation and good clinical outcome (modified Rankin scale score ≤2) at 90 days. Safety outcomes included symptomatic intracranial haemorrhage, all cause-death and severe adverse events at 90 days.
Results Between 3 March 2019 and 5 June 2021, 118 and 120 patients were randomly allocated to the Catfish and Solitaire groups, respectively. The primary endpoint after all endovascular procedures was non-inferior in the Catfish group (88.5%, 100/113) than in the Solitaire group (87.7%, 100/114), with a rate difference (RD) of 0.78% (95% CI –7.64 to –9.20; p=0.001). Sensitivity analysis only considering the per-protocol set also yielded similar results, with an RD of 0.83% (95% CI –7.03 to –8.70; p<0.001). Additionally, the proportions of cases with good clinical outcomes (47.8% vs 50.0%, p=0.739) and all-cause death rates (17.7% vs 18.8%, p=0.700) were similar in both groups at 90 days.
Conclusions The Catfish stent retriever is an effective and safe device for endovascular recanalisation in ELVO stroke.
Trial registration number NCT03820882.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Mechanical thrombectomy with stent retriever is considered the standard of care for emergent large vessel occlusion (ELVO) stroke.
WHAT THIS STUDY ADDS
The Catfish stent retriever is a novel mechanical thrombectomy device obtained by modifying material composition and structural design for endovascular recanalisation of ELVO stroke.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
There are many distinct kinds of stent retrievers on the international and domestic markets. However, independently developed stent retrievers are relatively limited. The study provides an alternative option for the operator with an independently developed stent retriever when facing an ELVO stroke case, especially in China.
Introduction
Mechanical thrombectomy (MT) using a stent retriever is considered one of the most efficacious therapies for emergent large vessel occlusion (ELVO) stroke.1–7 Therefore, the applied technique uses stent retriever embolectomy and is advocated as the main endovascular technical strategy for successful recanalisation in ELVO stroke.8 9 The Trevo (Stryker Corporation, Kalamazoo, Michigan) and Solitaire (Medtronic, Minneapolis, Minnesota) were the initial stents approved by the Food and Drug Administration for recanalisation in ELVO stroke. In recent years, newer generation stent retrievers have been designed, and various technical therapies have been refined for ELVO stroke. Concurrently, various stent retrievers are available for performing MT, each with different materials, configurations and clinical outcome profiles.
The Catfish stent (Catfish, JSSK Neurocare Medical Company, Beijing, China) is a self-expanding laser-cut nitinol device with closed cells and open-ended design. The device has a 0.018-inch push wire with a length of 1900 mm, and its proximal side (10 mm) is tapered for easy resheathing. The 0.021-inch microcathetre, which is produced with diameters of 3 mm (length, 20 mm), 4 mm (length, 20 mm), 5 mm (length, 30 mm) or 6 mm (length, 40 mm), is recommended for stent delivery. A major difference between Catfish and other stent retrievers is that the latter device is cylindrical with a variable diameter of stent struts oriented around the longitudinal axis of the stent alternately in a helical fashion, thus strengthening a radial force and wall apposition in the centre of the device. In addition, the large cell design of the Catfish stent retriever allows for integration into the thrombus. Moreover, the device enables full-length visibility via braiding of three radiopaque platinum wires into the stent struts, thus allowing the visualisation of the device’s clot integration. Furthermore, it has one proximal and three distal markers to indicate device expansion (figure 1). In animals, the Catfish stent retriever effectively achieved swift reperfusion of occluded arteries with no clinically meaningful adverse event.

Illustration of the Catfish stent-retriever device. (A) The thinner strut of the proximal-third segment and distal-third segment which was equal to 0.7-fold diameter of strut at middle-third segment, three distal radio-opaque markers. A2: large clot catching cell. A3: radiopaque platinum wire integration into the stent strut. A4: One Proximal radio-opaque marker. (B) The Catfish (B2) have a larger stent cells compared to the competitive stent (B1). (C) The Catfish have a optimal coverage and wall apposition peculiarity in tortuous anatomical model. (D) Fluoroscopic visibility of the deployed Catfish stent retriever device.
This trial aimed to compare the Catfish stent retriever and the Solitaire stent retriever for MT efficacy and safety in patients with acute intracranial ELVO stroke.
Methods
Study design and patients
This study was a randomised, prospective, parallel-group, multicentre, open-label, non-inferiority trial conducted at 18 comprehensive stroke centres in China. This trial was registered before patient enrolment. Inclusion criteria were: (1) 18–80 years of age; (2) acute ischaemic stroke with occlusion of a proximal intracranial artery that could undergo endovascular therapy within 8-hour following the onset of stroke symptoms. Non-contrast CT or MRI was carried out for the identification of individuals with a small infarct core, that is, cases with an Alberta stroke program early CT score (ASPECTS) or posterior circulation Alberta stroke programme early CT score (pc–ASPECTS) of 6–10 and a baseline National Institutes of Health Stroke Scale (NIHSS) score of 8–25 (range: 0–42; the higher the score, the severer the neurologic deficits). However, participants were required to show functional independence prior to the stroke (modified Rankin scale (mRS) score of 0–2; range: 0 (normal)–6 (death)). Exclusion criteria were: a large ischaemic core on imaging (ASPECTS <6 or pc–ASPECTS <6), intracranial haemorrhage (ICH) on imaging, hypertension (systolic blood pressure)>185 mm Hg and/or diastolic blood pressure >110 mm Hg) after treatment with drugs, baseline platelet count <30×109 and utilisation of anticoagulants with International Normalised Ratio >3.0.
Randomisation and masking
Patients were randomised into groups in a 1:1 ratio to receive Catfish or Solitaire devices for the initial thrombectomy using a central web-based system. Immediate availability of randomisation assigned to investigators prevented any treatment delays.
Due to the procedure’s nature, assignment to the treatment group was known to the neurointerventionalist and the patient. However, an independent central core imaging laboratory was used, and the independent clinical outcome committee was unaware of study group assignment and the categorised adverse events associated with the study device and procedures.
Endovascular thrombectomy
Once patients were allocated to either the Catfish or Solitaire group, they were administered intravenous alteplase (tPA) as a bridging therapy within 4.5 hour after stroke onset, with a maximum dose of 0.9 mg/kg if they had no contraindication to intravenous thrombolysis. Then, they were transferred to the angiography unit rapidly for immediate thrombectomy. Endovascular access and anaesthesia administration were carried out based on the local practices of the study centre. Before MT, baseline digital subtraction angiography (DSA) was carried out for defining vascular occlusion. The assigned stent retriever was required to make at least three attempts to achieve maximal recanalisation before switching to another endovascular procedure. Aspiration using an intermediate catheter close to the stent retriever’s proximal end was allowed in both arms. However, aspiration combined with the stent retriever was not allowed in both groups on the first pass. In case of successful reperfusion, that is, modified thrombolysis in cerebral infarction (mTICI) grade 2b (50%–89% reperfusion) or greater was not achieved by the third or last pass, additional or adjunctive contact aspiration, intra-arterial thrombolysis or angioplasty with/without stenting was allowed to be performed. The use of these rescue techniques was at the operator’s discretion. When the balloon rescue permanent stenting was performed, tirofiban was administered for 24 hours in case of no obvious ICH revealed on the follow-up CT scan. Then, tirofiban was terminated after dual antiplatelet and tirofiban treatment for 4 hours, and dural antiplatelet was continued for 3 months. Subsequently, daily oral antiplatelet therapy was adjusted based on blood examination results at 90 days postprocedure. The mTICI score was recorded after each attempt.
All patients underwent neurological examinations, including NIHSS score assessments at baseline, 24 hours and 7 days (or discharge if earlier) and mRS score evaluation at 90 days after randomisation. In addition, repeat brain CT or MRI was performed 24 hours postprocedure to assess haemorrhagic transformation.
Outcomes
The primary outcome was the rate of cases who underwent successful recanalisation (mTICI score of 2b or 3) after angiography as assessed at the central core imaging laboratory. Secondary efficacy outcomes were NIHSS scores at 24 hours and 7 days or discharge if earlier; time elapsed between artery puncture and successful recanalisation (mTICI score of 2b or greater) and good clinical outcomes at 90 days (mRS score≤2).
Safety outcomes were symptomatic ICH (sICH; defined as intracerebral haemorrhage on CT or MRI at 24 hours, which is reflected by a 4-point elevation of neurological deterioration of the NIHSS score based on the European Cooperative Acute Stroke Study 3 classification),10 all-cause mortality and serious adverse events (SAEs) at 90 days.
The subjective experience of interventionalists with the MT device was surveyed using an ordinal 5-point scale, with 1–5 reflecting very easy, easy, neutral, hard and very hard, respectively.11
Statistical analysis
The study design targeted a power of 80% and a two-sided α=0·05 to demonstrate the non-inferiority of the Catfish stent retriever over the Solitaire stent retriever in achieving successful revascularisation. The sample size was determined with the assumption the proportion of cases with successful recanalisation using the Catfish retriever would be approximately 87.9%, which was non-inferior to the revascularisation rate of the Solitaire stent retriever based on published data.2 12 A clinically relevant non-inferiority margin of 12.5% was applied as acceptable difference between the two groups, with a proximal 10% loss to follow-up. Therefore, 119 cases were required in each group.
The primary data analysis followed the per-treatment analysis principle; sensitivity analysis used the per-protocol population to assess the efficacy endpoint in both groups. Descriptive statistics was applied to present the data. The Wilcoxon rank sum test or two-sample t test was applied to compare continuous variables, while categorical variables were compared by the Fisher exact test. SAS V.9.4 was used for statistical analysis, with two-sided p<0.05, indicating statistical significance.
Results
Baseline characteristics and randomisation
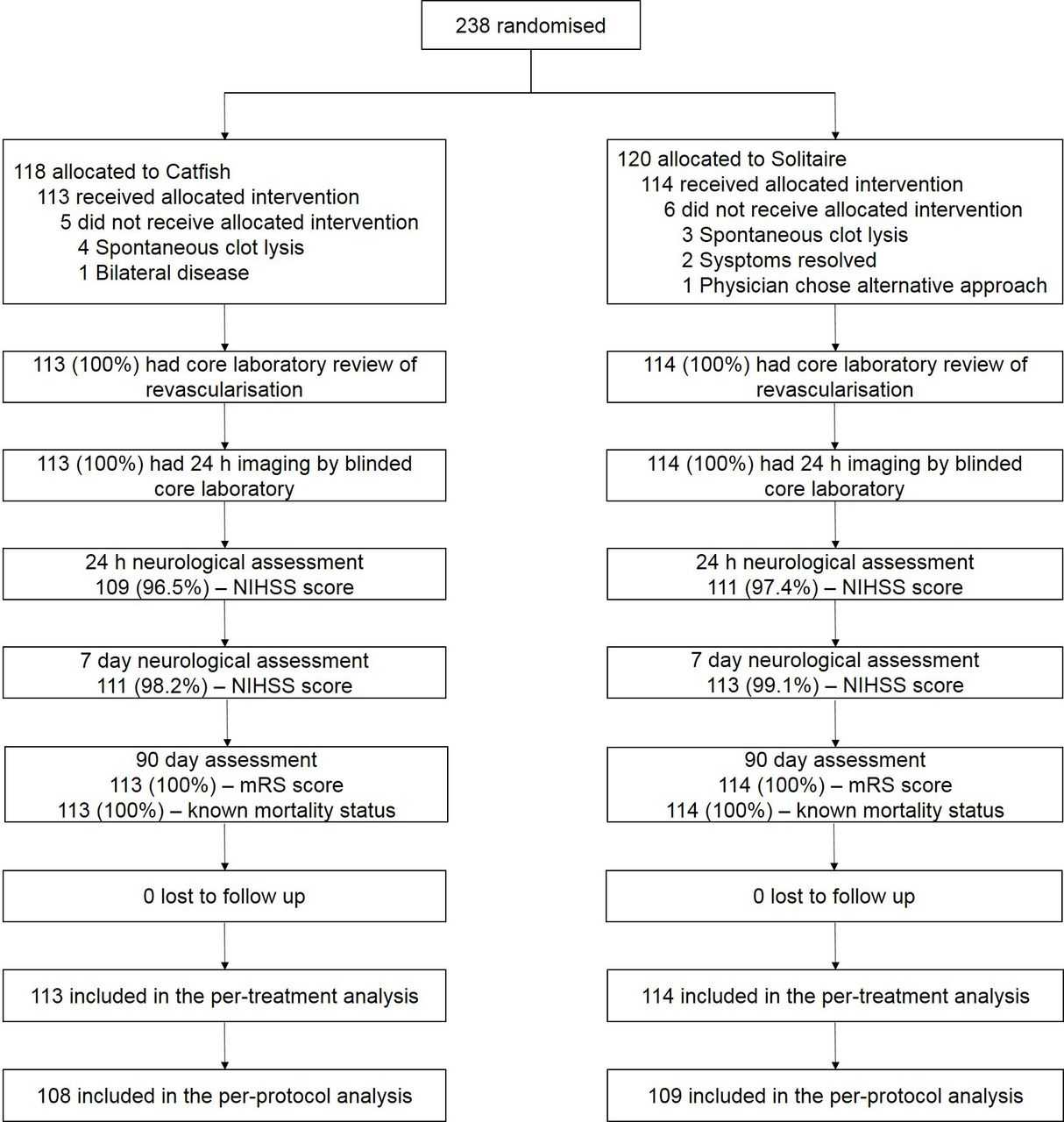
Figure 2 shows patients’ enrolment, screening and follow-up profiles. Between 3 March 2019 and 5 January 2021, 238 cases in 18 comprehensive stroke centres in China underwent randomisation into the Catfish (n=118) and Solitaire (n=120) groups. Eleven patients did not receive the assigned intervention, mainly because the symptoms were relieved before the stent retriever procedure (n=2), the majority of the thrombus showed spontaneous lysis on DSA images before MT (n=7), bilateral disease revealed by MRI (n=1) and use of an aspiration-first approach only for thrombectomy (n=1). In addition, no patients crossed over to the contralateral group. Therefore, the per-treatment population had 227 cases, with 113 and 114 patients allocated to the Catfish and Solitaire groups, respectively. The patients averaged 62.1 years old (SD 12.8) and 57.7% were men. Median time elapsed between symptom onset to main hospital arrival was 184.8 min (IQR, 114.6–240 min), median baseline NIHSS score was 16 (IQR, 12–19) and intravenous tPA was administered to 40.5% (92/227) of the patients. The demographic characteristics were balanced between the Catfish and Solitaire groups, including age, sex, NIHSS score, ASPECT score, pc–ASPECT score, medical history, blood pressure at admission, mRS score before the stroke and site of occlusion (table 1).
Baseline clinicodemographic features

Trial profile. mRS, modified Rankin scale; NIHSS, National Institutes of Health Stroke Scale.
Primary outcomes
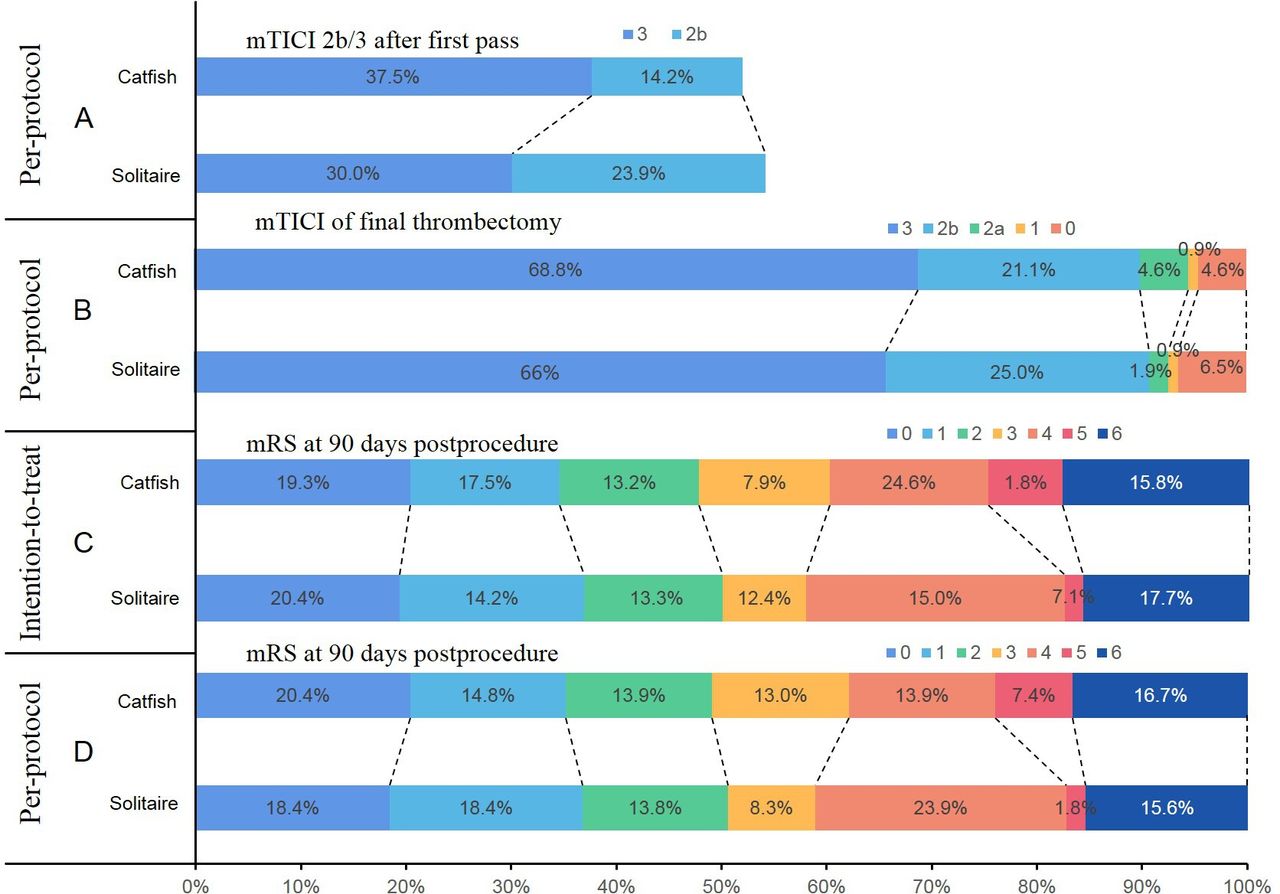
The primary angiographic efficacy outcome in the 227 patients in the per-treatment analysis was assessed at the core laboratory, showing that patients achieved an mTICI score of 2b/3 and recanalisation after all endovascular procedures in the Catfish group (88.5%, 100/113), which was non-inferior to the Solitaire group (87.7%, 100/114). The rate difference (RD) was 0.78% (95% CI –7.64 to 9.20; p=0.001). Sensitivity analysis exclusively considering the per-protocol set also yielded similar results, and the RD was 0.83% (95% CI –7.03 to 8.70; p<0.001) (table 2 and figure 3).
Efficacy endpoints and procedure details

Treatment outcomes. (A) Immediately mTICI grade after first pass thrombectomy; (B) mTICI grade at the end of the procedure, the successful recanalisation rate at the end of the precedure in the Catfish group was non-inferior to that in the Solitaire group for per-protocol population analysis (rate difference, 0.83; 95% CI –7.03 to 8.70;). (C) and (D) Modified Rankin Scale at 3 months. mTICI, modified thrombolysis in cerebral infarction.
Secondary outcomes
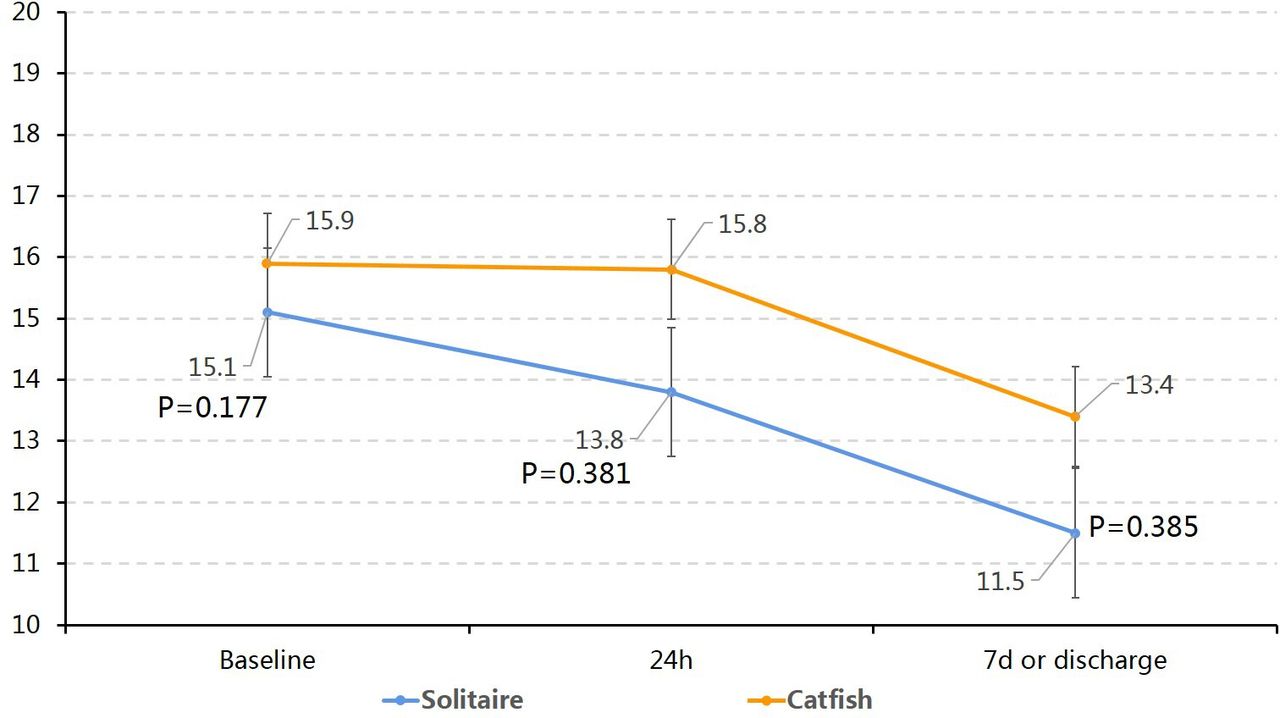
Secondary outcomes were comparable between the Catfish and Solitaire groups in the per-treatment set, with no differences in the time elapsed between arterial puncture to final successful reperfusion, NIHSS scores at 24 hours and 7 days or discharge, and the rate of cases with successful recanalisation after the first pass (table 2). Additionally, angiographic outcomes following the first pass alone showed a higher mTICI 3–grade reperfusion rate in the Catfish group (37.5%, 42/112) in comparison with the Solitaire group (30.0%, 34/113) (figure 3). Successful recanalisation (mTICI ≥2 b) rates using the assigned clot retriever devices alone were also not significantly different between the Catfish (88.8%, 87/98) and Solitaire (89.5%, 85/95) groups, and further per-protocol analysis yielded data corroborating those of the per-treatment analysis, in which successful recanalisation using the Catfish stent retriever alone showed non-inferiority versus using the Solitaire stent retriever alone (p=0.709), with 86 patients (91.5%, n=94) in the Catfish group and 84 (92.3%, n=91) in the Solitaire group. Rescue techniques after first-line therapy were performed in 15 (13.3%) and 19 (14.2%) cases of the Catfish and Solitaire groups, respectively, indicating a difference with no statistical significance. As shown in figure 4, early neurological outcome improvement had no significant difference between the two groups, with NIHSS score changes averaging –0.2 (SD 9.9) and –1.2 (SD 7.8) points in the Catfish and Solitaire groups at 24 hours, respectively, and –2.6 (SD 11.0) and –3.6 (SD 9.2) points at 7 days or at discharge, respectively. Additionally, clinical efficacy outcomes based on 90-day mRS 0–2 score rates showed no differences between these groups in the per-treatment or per-protocol analysis.

Categorised whisker plots of mean NIHSS scores at admission, at 24 hours, and at 7 days or discharge in both groups. NIHSS, National Institutes of Health Stroke Scale.
Safety outcomes
Device-associated and procedure-associated SAEs showed comparable frequencies in both groups (table 3); however, embolisation into new territory was more commonly detected in the Solitaire group than the Catfish group. sICH was found in 9 (8.0%) and 9 (7.9%) cases in the Catfish and Solitaire groups, respectively (p=0.984). All-cause death at 90 days occurred with a slightly higher rate in the Catfish group compared with the Solitaire group (20/113, 17.7% vs 18/114, 15.8%); however, the difference was insignificant.
Safety endpoints
The delivery of the stent retriever system was rated ‘very easy’ by 36.3% (41/113) and 36.8% (42/114) of cases in the Catfish and Solitaire groups, respectively, ‘easy’ in 61.1% (69/113) and 61.4% (70/114), respectively, and ‘neutral’ in 2.6% (3/113) and 1.8% (2/114), respectively. Meanwhile, neither group’s procedures were rated as ‘hard’ or ‘very hard’.
Discussion
In the current randomised, prospective, multicentre study, the Catfish stent retriever had an elevated rate of final successful reperfusion in clinical ELVO stroke, with non-inferiority to the Solitaire stent retriever. Our results demonstrated a recanalisation rate consistent with that in multiple randomised studies reported in 2015, with recanalisation rates of 59%–88%.1–5 Likewise, all secondary clinical results were comparable in both groups, including NIHSS scores at 24 hours and 7 days or discharge and good neurological outcome (mRS score ≤2) at 90 days. In addition, although the rates of cases with an mTICI score of 2b–three were similar while using assigned devices alone in both groups, the Catfish stent retriever showed favourable performance over the Solitaire stent retriever in several measures, including complete first-pass reperfusion (mTICI score of 3), faster successful recanalisation rate, and lower use of rescue treatment to achieve recanalisation. This might be attributed to several overlapping mechanisms. First, the Catfish stent retriever has a variable diameter of stent struts oriented around the longitudinal axis of the stent alternately in a helical fashion, which could strengthen an outward radial force of the middle segment of the device, resulting in higher rates of clot removal.13 Moreover, these unique characteristics of the device can also optimise the wall apposition of the stent and facilitate the capture of thrombus in tortuous vessels. Second, the device’s large cell design allows the clot to be embedded in the stent mesh other than ploughing the thrombus against the vessel wall. Third, previously reported data indicated stent retrievers with shorter lengths and smaller diameters are associated with adverse events in the MT procedure14 15; however, larger and longer stent retrievers can not only better capture the clots but also yield a higher rate of first-pass revascularisation than smaller and shorter stents.13 15 16 For small vessels occluded or more distal clots, correct positioning of the thrombectomy device is extremely challenging. The Catfish stent retriever is available in 3, 4, 5 and 6 mm diameters with lengths of 20–40 mm, with the intent of treating vessels with diameters of 1.5–5.5 mm. This wide selection of different stent sizes allows for navigation up to distal and smaller vessels to capture the target lesion. Furthermore, it can also enhance thrombectomy performance in removing high clot burden. Moreover, the Catfish stent retriever has three distal device markers that allow the visualisation of the device’s expansion and clot integration.17 The handling and navigability of the Catfish stent retriever are non-inferior to those of the Solitaire stent retriever, which was also indicated by the procedural time metrics. The median time interval from the arterial puncture to successful recanalisation showed a slight reduction with the Catfish retriever compared with the Solitaire counterpart; however, the difference was insignificant (81.6 min vs 82.2 min). In addition to these features of the Catfish stent retriever, as a new and completely independent development MT device, it was approved by the National Medical Products Administration of China in May 2022. Therefore, the catfish stent retriever is now easily available in the short term to operators in one-third of the provinces of China. Moreover, early postmarket experience suggests that the mean price of each Catfish stent retriever is approximately RMB 4000 cheaper than the control stent retriever in the postmarket provinces.
Furthermore, another advantage of the Catfish stent retriever to consider is its safety. Prespecified safety analyses of SAEs, sICH and all-cause death at 90 days revealed that the Catfish stent retriever was as safe as the Solitaire stent retriever, with rates consistent with those reported in previous studies.18–20 Notably, an already published early experience revealed a high radial force of the stent retriever, resulting in efficient clot incorporation and retrievability13; however, this feature could also lead to endothelial vessel injury.21 22 Our results showed that the rates of procedure-related complications, including vasospasm, arterial perforation and subarachnoid haemorrhage, were slightly elevated in the Catfish group compared with the Solitaire group, although not significantly. Furthermore, the rate of distal embolism was slightly reduced in the Catfish group owing to the longer stent design of the Catfish device, and the design could increase distal protection by reducing clot migration out of the stent.16
The current study had limitations. A major limitation was its unavoidably open-label design; however, the potential bias was mitigated using a blinded adjudication committee and a core laboratory. In addition, the study had strict inclusion and exclusion criteria for its randomised design; therefore, the results may have limited generalisability.
Conclusions
The Catfish stent retriever is effective and safe for endovascular recanalisation in ELVO stroke.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
All procedures were in accordance with the Declaration of Helsinki and approved by the Ethical Committee of our University Hospital. The number of the approved ethical statement number is 'QX2018-011-02'. Participants or their legally authorised representatives provided written informed consent. Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors GL and ZM participated in the design of the trial. GX, LW, NBJ, RM, WC, CF, ZZ, JW, YP, GZ, JZ, LL, HY, JW, BL, FZ, YC, FG participated in the data collection and interpretation. The statistical analysis was done by XY. GL wrote and revised the report. All authors provided review and approval of the final paper.
Funding The study is supported by grants from Beijing Hospitals Authority Youth Programme (Number QML20190505), National Key R&D Program (2018AAA0102600), Beijing Natural Science Foundation (Z220016), JSSK Neurocare Medical Co., Ltd.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}