

Abstract
Background and purpose Hyperperfusion (HP) is a devastating complication associated with carotid artery stenting (CAS) or endarterectomy. The efficacy and safety of staged angioplasty (SAP) in patients with CAS at high risk of HP remains unclear. We sought to determine whether SAP is superior to regular CAS in patients with high risk of HP.
Methods A randomised, multicentre open-label clinical trial with blinded outcome assessment (STEP) was conducted. Patients with severe carotid stenosis at high risk of HP were randomly assigned (1:1) to the SAP or regular CAS group. The primary endpoint was hyperperfusion syndrome (HPS) and intracerebral haemorrhage (ICH) within 30 days after the procedure.
Results From November 2014 to January 2017, a total of 64 patients were enrolled in 11 centres. 33 patients were allocated to the SAP group and 31 to the regular CAS group. At 30 days, the rate of primary endpoint was 0.0% (0/33) in the SAP group and 9.7% (3/31) in the regular CAS group (absolute risk reduction (ARR), 9.7%; 95% CI −20.1% to 0.7%; p=0.11). As one of the secondary endpoints, the incidence of HP phenomenon (HPP) was lower in the SAP group than the regular CAS group (0.0% vs 22.6%, ARR,−22.6%; 95% CI −36.8% to −10.2%; p=0.04).
Conclusion The rate of HPS and ICH was not significantly lower in SAP group; the extended secondary endpoint of HPP, however, significantly reduced, which suggested that SAP may be a safe and effective carotid revascularisation procedure to prevent HP.
Trial registration number NCT02224209.
Introduction
Hyperperfusion (HP) is one of the most devastating complications associated with carotid artery stenting (CAS) and endarterectomy.1 2 HP is caused by excessively increased cerebral blood flow (CBF) above the metabolic needs of the brain tissue. Patients may have no symptoms (hyperperfusion phenomenon, HPP) or may present with ipsilateral headache, seizure and focal neurological deficit (hyperperfusion syndrome, HPS) and even intracerebral haemorrhage (ICH).1 The mortality rate of ICH is as high as 50%, and the majority of survivors suffer from severe disability. Even the relatively less severe manifestations such as cerebral dysfunction or seizures can lead to permanent morbidity and mortality.3 4
Although HP is normally considered a rare complication, the incidence ranges from 14.1%–18.9% in patients at high risk.5 6 Efforts to prevent HP are limited to identifying patients with a high risk before the procedure and vigilantly monitoring and controlling systemic blood pressure after the procedure. However, evidence that such preventive measures actually reduce the incidence of HP is lacking.7 8
Staged angioplasty (SAP) was proposed by Yoshimura et al,9 as a potential method to reduce HP after carotid revascularisation. Patients underwent primary angioplasty with an undersized balloon as the first stage (Stage 1), followed by stenting 1–2 months later as the second stage (Stage 2). As HPS is a result of rapidly increased CBF in excess of metabolic demands, the rationale for SAP is to restore blood flow in a stepwise manner.10
According to a questionnaire survey in Japan in 2014 (JSNET), SAP was either attempted or performed in 27.1% of the participating centres for patients at high risk of HP.11 Several reports have also discussed the potential benefits of SAP compared with regular CAS.12–16 However, these studies were case series or retrospective analyses; therefore, randomised controlled clinical trials are needed to examine the efficacy and safety of SAP for the treatment of carotid artery stenosis. The aim of this randomised trial was to examine whether SAP was superior to regular CAS in patients with carotid artery stenosis at high risk of HP.
Methods
Study design and patients
Comparison of Staged Angioplasty and Routine Single-stage Stenting in the Treatment of Carotid Artery Stenosis (STEP) was a prospective, randomised, multicentre, open-label trial performed at 11 high-volume interventional stroke centres in China (NCT02224209). Patients who met the following criteria were enrolled: (1) age 40–80 years old; (2) symptomatic carotid stenosis (defined as carotid stenosis associated with stroke or transient ischaemic attack within 90 days preceding randomisation); (3) stenosis degree ≥85% (measured according to NASCET method) or near occlusion on angiography; (4) insufficient collateral circulation in the culprit vessel supplying area, which was defined as American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR)<2 on DSA,17 (5) hypoperfusion of the culprit vessel supplying area on cerebral CT perfusion (CTP) (CBF of the culprit side is of 20% lower than the contralateral side) or haemodynamic ischaemic lesion on MRI; (6) lesion length at the narrowest part <25 mm. Patients were excluded if they had (1) intracerebral haemorrhage at the culprit vessel surrounding area within 6 weeks preceding randomisation; (2) potential thrombus from the heart; (3) diffuse intracranial artery stenosis and (4) functional dependence because of cerebral infarction in the culprit vessel supplying area (modified Rankins Scale score ≥3). Detailed protocol was available in the supplement.
The protocol was approved by the institutional review board of each participating centre. Written informed consent was obtained from the participants or their legal representatives. An independent data-monitoring committee had access to all study data and monitored the safety of participants on a quarterly basis throughout the trial.
Randomisation and masking
Patients were randomly allocated 1:1 to the SAP arm or the regular CAS arm. The randomisation sequence was generated using an online system. The interventional neuroradiologist received the randomisation number and assigned the result by messaging the patient after enrolment.
Patients were assessed at baseline, and 4 days and 30 days after each procedure (Stage 1, Stage 2 or regular CAS) by a neurologist who was unaware of the treatment assignments. If an endpoint was suspected during the follow-up period, the patient was examined by the Endpoint Determination Committee, which was responsible for analysing and coding all study-related major clinical outcomes and identifying adverse events. All possible primary and secondary endpoints were independently analysed and determined by two members of the Committee by referring to established standards. If the two members had unanimous opinions, the event was confirmed and correspondingly coded. If the members’ opinions differed, the possible endpoint was analysed by all members of the Endpoint Determination Committee.
Procedures
For patients assigned to the SAP arm, an embolic protection device and semicompliant balloon with a small diameter of 2–3 mm was used in Stage 1. The balloon was inflated to a nominal pressure for 20 s before deflation. If angiogram after the inflation showed a residual stenosis of <70%, the procedure was considered successful. The operators could determine to perform stenting or other rescue treatments during Stage 1 if any complications occurred, such as dissection, recoil or occlusion. Stage 2 of SAP was performed 2–4 weeks after Stage 1. An embolic protection device was also used. A semicompliant balloon with a diameter of 4–6 mm was chosen based on the lumen diameter that was distal to the stenotic lesion. The balloon was used to predilate the lesion before the deployment of a self-expanding stent. Additionally, postdilation was performed after the stenting if necessary. For patients assigned to the regular CAS arm, CAS was performed according to the published guidelines.18
Perioperative management
All patients underwent continuous blood pressure monitoring for at least 72 hours after the procedure. The goal was to control systolic pressure of no more than 120 mm Hg. Patients were given aspirin (100 mg/day) and clopidogrel (75 mg/day) for at least 5 days prior to the procedure (regular CAS or Stage 1 of SAP) or a loading dose of 300 mg 24 hours (aspirin) or 6 hours (clopidogrel) before the procedure. The dual antiplatelet medication was used for 90 days before being changed to aspirin alone. Management of risk factors (hypertension, high low-density lipoprotein (LDL), diabetes, smoking, overweight and lack of exercise) were recommended. For major risk factors, we defined target blood pressure as systolic blood pressure (SBP) <140 mm Hg (or for patients with diabetes, <130 mm Hg); LDL <70 mg/dL (1.81 mmol/L) or decreased by 50%.
Endpoints
The primary endpoint was HPS and ICH within 30 days after the regular CAS, Stage 1 or Stage 2 of SAP.9 14 HPS was defined as ipsilateral temporal, frontal or retro-orbital throbbing headache with or without nausea, vomiting, ipsilateral focal seizures, confusion or focal neurological deficit without evidence of infarction. ICH was defined as hyperdensities that were consistent with blood in the parenchyma of the culprit hemisphere on CT.
The secondary endpoints within 30 days included HPP which was defined as an increase of CBF >100% than the baseline detected by transcranial Doppler (TCD) or CTP; procedure-related adverse events; myocardial infarction; major non-stroke haemorrhage (eg, epidural haemorrhage, intradural haemorrhage or other major systemic bleedings); death; stoke resulting in deformity.16
Statistical analysis
We assumed a sample size of 150 (75 SAP: 75 regular CAS) were required, to account for an estimated 5% dropout rate, approximately 158 patients were planned to be enrolled. Because of the difficulty in recruitment and lack of funds, our study stopped ahead of the schedule. According to previous studies,12 14 the rate of HPS and ICH was expected to be 16% for patients with high risk of HP in the regular CAS arm, and 2% for patients with high HP risk during the procedure in the SAP arm. In this condition, based on two-tailed superiority test α 0.05, the power of primary endpoint will be more than 85%. The sample size calculation was performed using SAS software, V.9.3 (SAS Institute).
Analyses were performed on all randomised patients in the assigned groups according to the intention-to-treat principle. Categorical variables are described as frequencies and percentages. Continuous variables are described as means (SD) and compared with student’s t test for normally distribution, medians (IQR) and Wilcoxon test for skewed distribution. Categorical variables, rates of the primary and secondary endpoints were described as frequency (percentage) and compared between the two groups using χ² test or Fisher’s exact test. A sensitivity analysis was conducted in the per-protocol population.
Results
Randomisation and baseline characteristics
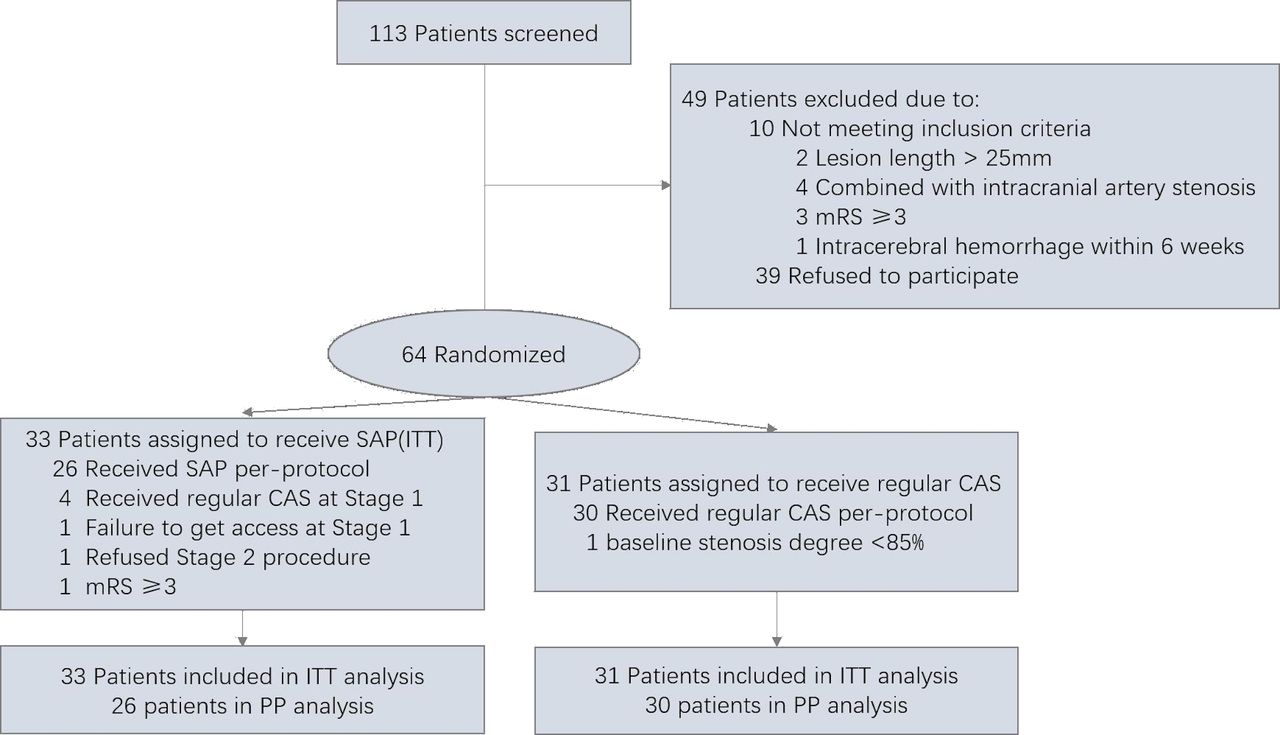
Of the 113 screened patients, 64 patients (52 men (81.3%) and 12 women (18.8%); mean age: 66±7.4 years) were enrolled and allocated to the SAP group (n=33) or the regular CAS group (n=31) between November 2014 and January 2017. The enrolment was halted because of the difficulty in recruitment and lack of funds (figure 1). Of the 33 patients in the SAP group, we excluded seven patients in the process; among these excluded patients, four changed SAP to regular CAS at Stage 1 because of dissection or recoil; one patient failed to get accessed at Stage 1; one patient rejected the Stage 2 operation after the Stage 1 procedure was performed and one with modified Rankin Scale (mRS) >3. Of 31 in the regular CAS group, one patient was excluded due to baseline stenosis degree less than 85%. The two groups were balanced regarding the baseline characteristics (table 1).
Characteristics of patients at baseline

Study flowchart for patients with carotid artery stenosis at high risk of hyperperfusion. CAS, carotid artery stenting; ITT, intent-to-treat; mRS, modified Rankin Scale; PP, per-protocol; SAP, staged angioplasty.
The characteristics of patients during the perioperative period were also well balanced, except the patients in SAP group had higher postprocedural SBP, smaller max balloon diameter and larger postprocedural minimum lumen diameter (table 2).
Characteristics of patients during perioperative period
Primary endpoint
Among the 64 enrolled patients, HPS occurred in two patients and ICH in one patient, all in the regular CAS group. The clinical manifestations of the three patients were detailed in table 3. The rates of primary endpoint of HPS or ICH within 30 days after each operation in the intention-to-treat population were 0/33 (0%) in patients of the SAP group and 3/31 (9.7%) in patients of the regular CAS group (absolute risk reduction, 9.7%; 95% CI −20.1% to 0.7%; p=0.11). Eight patients were excluded from the per-protocol analysis due to the following major protocol violations: not receiving allocated treatment (n=6), mRS >3 (n=1), carotid artery stenosis degree <85% (n=1). There were no statistically significant between-group differences in the primary endpoint in sensitivity analyses restricted to the per-protocol population (0% vs 10.0%, SAP vs regular CAS group, absolute risk reduction, 10.0%; 95% CI −22.5% to 1.1%; p=0.24) (online supplemental table S1).
Supplementary data
Characteristics of patients with hyperperfusion syndrome or intracerebral haemorrhage
Secondary endpoints
TCD or CTP data were available for 30 patients (90.9%) in the SAP arm and 27 patients (87.1%) in the CAS arm. The incidence of HPP was lower in the SAP group than in the regular CAS group (0.0% vs 22.6%, respectively; absolute risk reduction, −22.6%; 95% CI −36.8% to −10.2%; p=0.04). Procedure-related adverse events occurred in one patient (3.0%) in the SAP group and two patients (6.5%) in the regular CAS group (relative risk, 0.64; 95% CI 0.13 to 3.21; p=0.61). Myocardial infarction was observed in one patient (3.0%) in the SAP group, and one patient (3.2%) in the regular CAS group (relative risk, 0.97; 95% CI 0.24 to 3.96; p=1.00). No major non-stroke haemorrhage, death or stroke resulting in deformity occurred in any participant (table 4), and we found the same pattern of results for the postprocedure data (online supplemental table S1).
Outcomes of primary endpoint and secondary endpoints from the treatment groups in ITT population
Discussion
The findings of STEP showed that in patients with carotid artery stenosis at high risk of HP, the rate of HPS and ICH in the SAP group seemed to be lower than the regular CAS group, although the difference was not statistically significant. As one of the secondary endpoints, the incidence of HPP was significantly reduced in SAP group. To our knowledge, this is the first randomised trial to compare SAP and regular CAS in patients with high risk of HP.
In this study, HPS or ICH occurred in three patients in the regular CAS group and no patients in the SAP group, but the difference was not statistically significant. Hayakawa et al 16 conducted a retrospective study in 44 Japanese centres to compare the efficacy of SAP and regular CAS. Among the 525 patients included in the analysis, the rate of cerebral hyperperfusion syndrome was lower in the SAP group than in the regular CAS group (4.4% vs 10.5%, respectively; p=0.047). One possible reason that our results did not demonstrate the superiority of SAP might be the small sample size. We planned to recruit 158 patients according to the protocol, but only 64 patients were enrolled because of difficulties in patient enrolment and lack of funds. As there was a potential trend towards a lower rate of HPS in the SAP arm, if the study could be completed according to the protocol, a potentially significant difference cannot be completely excluded. Although evaluating patients for the primary outcome did not reach the expected purpose, results from our study and many other multicentre studies showed the advantages of SAP in preventing HP and ICH complications;12 15 16 therefore, it is still reasonable to consider SAP as a safe treatment for patients with carotid artery stenosis at high risk of HP. Furthermore, our experience suggested that the admission criteria for patients prone to high-risk complications should be widened in future studies to include prevention of high-risk complications by staging treatment in patients with carotid stenosis.
As a secondary endpoint, the incidence of HPP was higher in the regular CAS group than in the SAP group. Although HPP was not as devastating as HPS or ICH, HPP could deteriorate and convert to ICH or HPP, even with treatment. Yoshimura et al,9 who were the first to demonstrate SAP, also used HPP as a sign of HP. Our study demonstrated that SAP effectively reduced the rate of HPP compared with regular CAS.
Our results suggested that angioplasty with an undersized balloon alone was associated with a higher risk of complications, such as dissection, recoil or even occlusion, compared with regular CAS. Such complications were likely to lead to technical failure of SAP. Our early experience with SAP was that the strategy was safe. We (Mo et al)12 reported previously that three patients requiring stenting at the angioplasty stage for carotid dissections suffered no complications, in the retrospective 44 cases who accepted staged CAS. Recoil and occlusion also did not occur in the other cases.12 In a multicentre study, Yoo et al 15 found no cases of severe recoil during the interval between balloon angioplasty and delayed definitive stenting in their 53 cases. In the current study, technical failure caused by these complications at Stage 1 was a potential drawback of SAP, and these complications occurred in four patients (12.1%); however, rescue treatment with stenting was successfully performed in all four patients. Another concern with SAP was that an additional operation may increase the risk of periprocedural complications, such as distal embolism or vascular perforation. Yoshimura et al 9 found no significant difference in the rate of distal embolism between the SAP group and regular group, in patients who accepted postoperative diffusion-weighted imaging. In our trial, one procedure-related adverse event occurred in the SAP group, which was similar to the rate in the regular CAS group. Among patients who underwent the Stage 1 procedure successfully, none experienced reocclusion or other complications during the two stages. Therefore, a lack of safety might not be a concern regarding SAP.
Our experience in this study suggested that it is necessary to be highly vigilant regarding individuals with a higher probability of HP and ICH after conventional stent implantation in patients undergoing CAS in clinical practice. It may be better for primary hospitals to evaluate patients’ cerebrovascular reactivity (CVR). If CVR is seriously decreased, SAP may be a safe and more effective strategy to prevent the complications of HP and cerebral haemorrhage.19–21
SAP requires two operations, and the interval between the two operations required in this study was 2–4 weeks. This interval likely requires patients to be admitted to hospital twice, leading to increased medical expenses. The ideal treatment staging interval is unclear, but most experts believe that the most appropriate interval is 2 weeks.16 19–21 Therefore, it is feasible to shorten the staging interval to 2 weeks or to within 2 weeks and strive to complete the two procedures in one hospital to reduce medical costs.
Our study has limitations. First, the small sample size and the low event rate were major problems; furthermore, the power was only 0.45 calculated with the final sample size, which may have led to false negative results. Because HPS is a relatively rare complication, a larger sample size is warranted to confirm the results in future studies. Second, we did not use single-photon emission computed tomography (SPECT) to screen patients for high risk of HP, as in previous studies, because SPECT was not available in some participating centres. These limitations should be considered, when interpreting our results. Future studies should use more strict criteria to enrol patients who are most likely to benefit from SAP.
Conclusion
Among patients with carotid artery stenosis at high risk of HP, the rate of HPS and ICH was not significantly lower in SAP group. However, the extended secondary endpoint of HPP significantly reduced, which suggested that SAP may be a safe and effective carotid revascularisation procedure to prevent HP.
Footnotes
Twitter @yilong
DM and BJ contributed equally.
Contributors DM, YoW, YiW and ZM conceived and led the project. HS, YS, QL, CF, JD, JY, WW, CJ, GZ, HD, LL and GP performed data collection and analysis. FG, NM, XS and LS performed quality control of the data. DM and BJ cowrote the manuscript with input from all coauthors.
Funding The work was supported by National Key Research and Development Program of China (2016YFC1301501) and Abbott Medical Devices Trading (Shanghai) Co., Ltd (no grant number).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by Institutional Review Board of Beijing Tiantan Hospital, Capital Medical University. Patient’s information, including name, initial, or hospital numbers is not mentioned in this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Requests for access to the data used in this report will be considered by the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}