

Abstract
Objective Sacral dural arteriovenous fistula (SDAVF) is a rare spinal vascular malformation and often misdiagnosed or even mistreated. This study delved into the clinical characteristics, vascular architecture and treatment results of SDAVF, with the goal of enhancing upcoming diagnostic and therapeutic methodologies.
Methods From March 2014 to March 2022, consecutive patients with SDAVF were retrospectively analysed. The data on demographics, symptom resolution, angioarchitectural features and postoperative course were studied. Spinal cord function was evaluated by modified Aminoff–Logue scale.
Results A total of 36 patients with 36 SDAVFs were enrolled, 12 of whom were misdiagnosed on their initial visit. The SDAVFs were located at S1 in 24 (66.7%), S2 in 10 (27.8%) and S3 in 2 (5.6%) cases, respectively. The primary feeding arteries included lateral sacral artery (LSA) of internal iliac artery (31/36, 86.1%), the branches of external iliac artery (2/36, 5.6%) and median artery (3/36, 8.3%), most of which are straight. Venae terminalisis is the sole drainage vein, flowing back into perimedullary venous network. Endovascular embolisation is the main therapy method for 30 cases, while the other 6 cases were treated with microsurgical fistulectomy. MRI tests showed that the abnormal vascular signals around the medulla disappeared, and the spinal cord oedema was alleviated in the majority of cases (32/36, 88.9%). Six patients, who all were treated by endovascular embolisation at first time, had residual or recurrent and two of them were performed by microsurgical fistulectomy again. All patients by microsurgical fistulectomy had no residual or recurrent during follow-up. According to the spinal cord functional assessment, the Aminoff-Logue score was significantly decreased (Z=−3.449, p=0.001) postoperatively.
Conclusion The misdiagnosis rate of SDAVF is very high. The most feeding artery of SDAVF came from the LSA, which was thicker and more straight, making it easier for microcatheters to reach the fistula site. So, endovascular embolism has become the first choice of treatment with minimal invasion, and safe and effective results.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Sacral dural arteriovenous fistula (SDAVF) with very low incidence was misdiagnosed and mistreated frequently.
WHAT THIS STUDY ADDS
The most feeding artery of SDAVF came from the lateral sacral artery, which made microcatheters easily reach the fistula.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
So, endovascular embolism has become the mainstream treatment.
Introduction
Spinal dural arteriovenous fistula (SDAVF) is the most common spinal vascular malformation, accounting for about 70% of all spinal cord diseases1 2; however, arteriovenous shunts in the sacral region were rarely reported.3 4 The symptoms from SDAVFs are often subtle and non-specific; thus, the following clinical course is often slowly progressive, causing a high rate of misdiagnosis and serious spinal cord dysfunction.5 6 Even if the diagnosis is clear, the different individual in experience and preferences among surgeons make the treatment plan varies considerably. This is a retrospective study that analysed the clinical information of patients with SDAVF at our centre over the past 10 years and proposed the overall treatment plan.
Methods
General data
From March 2012 to February 2022, patients with SDAVF were collected. This was a retrospective observational study. All patients were informed of details of this study, including allowing anonymous disclosure of clinical data and images, and signed an informed consent. Inclusion criteria: (1) SDAVFs were confirmed by digital subtraction angiography (DSA). (2) Endovascular embolisation and/or microsurgery were performed. (3) Received at least 6 months of follow-up. Exclusion criteria: (1) Other pathogens associated with impairment of brain and/or spinal cord function. (2) Received radiation therapy, such as Gamma knife, CyberKnife and other radiation therapy.
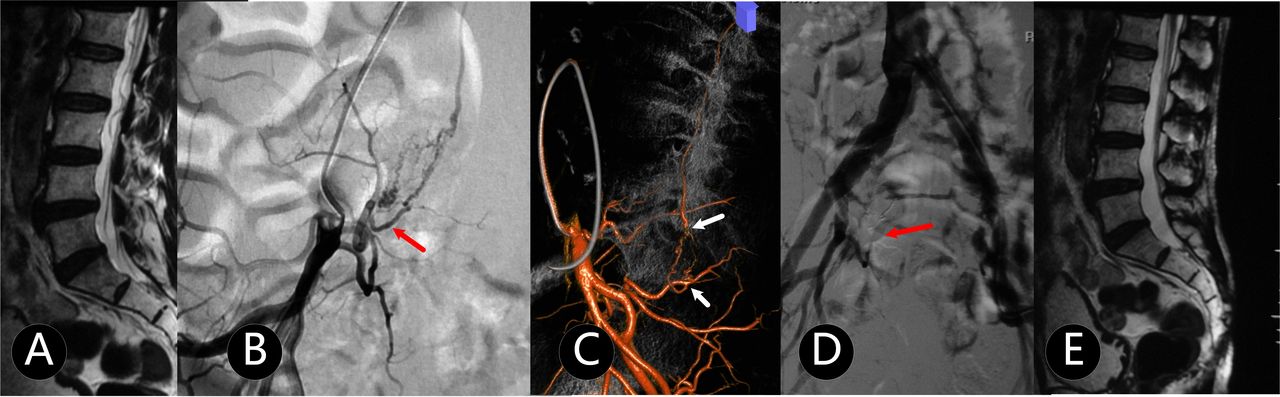
MRI: Abnormal vascular flow vacuum signals in lumbosacral canal were displayed, accompanied by different degrees of spinal cord oedema and perimedullary veins (figure 1A).

A patient in 60s with incontinence urine and faeces for 5 months and aggravating for 1 month in bilateral lower limbs with numbness (mALs=5 points, mild disorder). (A) Abnormal vascular signal was tested in spinal canal by MRI-T2. (B) and (C) DSA and 3-D reconstruction images showed that SDAVF was fed by lateral sacral artery of internal iliac artery. (D) The DAVF system, including fistula, feeding artery and draining vein, was eliminated completely. (E) There was no abnormal blood flow signal after 6 months postoperation. 3-D, three-dimensional; DAVF, dural arteriovenous fistula; DSA, digital subtraction angiography; mALs, modified Aminoff–Logue scale; SDAVF, sacral dural arteriovenous fistula.
DSA examination
If initial MRI findings were suspicious for SDAVF, DSA examinations on whole spine should be performed. Superselective arteries included thyrocervical trunks, thoracolumbar and the arterial feeders of the sacral region. Imaging was anterioposterior projection, two frames/second. Oblique, lateral and rotary views were added to elucidate the morphology of SDAVF as well as the intradural course of drainage veins. Film sequences of at least 15 s were obtained. The SDAVF system, including shunts, feeding arteries and drainage veins, was defined by DSA or 3-D reconstruction (figure 1B,C).
Endovascular embolisation procedure
6 Fr Flexor Check-Flo Introducer Set (Cook Medical, USA) was generally adopted from contralateral femoral artery to affected iliac artery. Marathon flow directed microcatheter (Medtronic, USA) or Echelon 10 microcatheter (Medtronic, USA) was placed as far as possible close to shunt through feeding artery. After handled angiography was confirmed, the goal was to make the Onyx-18 (Micro Therapeutics, Inc., Irvine, CA, USA) flow into draining vein about 1 cm in length (figure 1D,E). Anticoagulation therapy and rehabilitation training were usually arranged on the second day after surgery.
Surgical treatment
The patients were placed in the prone position, and the corresponding segmental lamina was opened according to DSA result. The aberrant vascular structure was exposed under microsurgery and further confirmed by intraoperative Doppler and/or indocyanine green angiography (IGA). The draining vein was cut with electrocoagulation (figure 2). Anticoagulation therapy was usually started on the third day after surgery.

An adult patient with both lower limbs weakness and dysuria for more than 50 days, aggravating for 4 days. (A) The feeding artery was not visualised at arterial stage of angiography. (B) SDAVF was shown at S1 level at capillary stage of angiography. (C) The draining vein was eliminated by microsurgery totally. SDAVF, sacral dural arteriovenous fistula.
Neurological functional assessment and follow-up
The patient’s spinal cord function was evaluated by modified Aminoff–Logue scale (mAL)—excellent: normal or normal, ≤2 points; mild disorder, 3–5 points; moderate disorder, 6–8 and severe disorder, ≥9 points. The improvement or degradation of neurological function was defined when the score was changed at least one grade; and in the excellent group, the improvement was defined by patients’ subjective feeling or lower limb muscle strength improving.
All patients underwent spinal cord MRI before discharge and 6 months after operation, and the whole spinal cord angiography was performed at 6 months after operation, if possible, patients undergoing surgical treatment needed to be re-examined before discharge.
Statistical methods
SPSS 23.0 software was used for statistical analysis. Kolmogorov–Smirnov normality test was performed for continuous variables, and the normal distribution was expressed as the mean±SD. The data without normal distribution were represented as median (IQR) (M(Q)), and the numerical value of mAL score at preoperational test and last follow-up after operation was compared by Mann–Whitney U test. P<0.05 was considered statistically significant.
Results
Clinical data
36 cases were included in our cohort, of which 12 cases (33.3%) had been misdiagnosed with non-spinal vascular diseases at the initial visit and 1 patient had even received a spinal decompression and internal fixation surgery. MRI showed spinal cord oedema and dilated cauda equina or filum veins in all cases. The rate of young and middle-aged patients (< 50 years old) is 52.8% (18/36). The median course from the symptoms' onset to diagnosis was 4 months, ranging from 5 days to 3 years. Eight cases (22.2%) suffered from acute sudden onset (< 1 month). According to mALs, 27 cases were at good grade, and the rest were moderate grade.
Angioarchitectural features
Based on the spinal vascular angiography, the rate of shunts located in S1, S2 and S3 was 66.7%, 27.8% and 5.6%, respectively, in 36 cases (table 1). The main feeding arteries included lateral sacral artery of internal iliac artery (31/36, 86.1%), the branches of external iliac artery (2/36, 5.6%) and median artery (3/36, 8.3%), most of which were straight. Venae terminalisis was only draining vein, flowing back perimedullary venous network.
Clinical data of 36 patients with SDAVF
Therapeutic strategy
Six patients were treated by microsurgery and the reasons included the microcatheter being difficultly placed in two cases (figure 2) and the surgeon’s decision (figure 3) in four cases. 30 cases were performed by endovascular embolisation successfully at first time, and Onyx thoroughly penetrated and cast the draining vein in 76.7% (23/30) cases (figure 4). The average length of stay of endovascular embolisation (6.1±1.3 days) was significantly shorter, compared with microsurgeries (13.5±2.4 days).

A patient in 20s with right lower limb numb for half a year. (A) and (B) SDAVF located at S1 level (red arrow). (C) and (D) The draining vein was cut under microsurgery (white arrow). SDAVF, sacral dural arteriovenous fistula.

An adult with incontinence urine and faeces (mALs=6 points, moderate disorder) for 10 days. (A) SDAVF in S1 level (white arrow) was fed by the branches of lateral sacral artery. (B) The draining vein extends at conus medullaris level. (C) Microcatheter reached at fistula (white arrow) through the branch of lateral sacral artery. (D) and (E) SDAVF was embolised completely. mALs, modified Aminoff–Logue scale; SDAVF, sacral dural arteriovenous fistula.
Follow-up
After 12 months of surgery, the mAL scores decreased significantly (Z=−3.449,p=0.001), and 21 (73.3%) patients had improved, compared with preoperative scores. The abnormal vascular flow in the spinal canal and extramedullary disappeared, and spinal angiography showed no residual or recurrent lesions on 30 patients’ postoperative MRI (figure 1D). All 23 cases with Onyx thoroughly penetrating the draining vein in endovascular embolisation had no recurrence; however, there were other six patients, treated by endovascular embolisation, had residual or recurrent shown on MRI or spinal vascular angiography. Of the recurrence/residual six, four had slight or no symptoms with a small amount of abnormal drainage vein signals by MRI and refused further treatment, and two patients with mild disorder received microsurgery again. All six patients performed by microsurgery had no residual or recurrent during follow-up, and the rate of residual or recurrent had no statistic difference between (20%, 24/30) endovascular embolisation group and (0%) microsurgery group (χ2=1.440, p=0.230).
Discussion
This study indicated that, first, patients with SDAVF have a very high misdiagnosis rate (33.3%, 12/36), suffering from a certain amount of risk of serious mistreated-related harms. Second, endovascular embolisation can be chosen as a priority treatment, which is safe and effective for most of the patients (77.8%, 28/36) because of special vascular architecture of SDAVF. Finally, microsurgery is also one of the important and necessary treatments (22.2%, 8/36).
Because of non-specific clinical presentation, including motor weakness, sensory disturbances and sphincter dysfunctions, DAVF is easily misdiagnosed with various myelopathy disorders, such as cauda equina syndrome, transverse myelitis, anterior spinal artery infarction, spinal cord neoplasms and other demyelinating and degenerative diseases at neurology department.5 7 11 patients (30.6%) had been treated as myelitis or other kinds of non-vascular disease in their community hospitals and our 1 patient had been even performed by decompression of laminectomy and internal spinal fixation by an orthopaedic surgeon.
The rates of acute sudden onset (27.8%) and young patients were higher than in previous reports’.5 It is speculated that Foix–Alajouanine syndrome suddenly appears, leading to a non-compressive myelopathy and increasing venous hypertension may be the main reason for acute symptom in those patients,8 and misdiagnosis would cause disastrous results, such as spinal cord necrosis and paraplegia.9
Our neurosurgical centre is one of the most famous in China, to which the patients with ‘incurable syndrome’ in primary hospitals are recommended continually. It is our luck and responsibility to face so many difficult and complicated patients. It is suggested that if a dilated vein of the filum terminale was showed as a curvilinear flow void on T2WI or contrast-enhanced MR angiography,10 11 the patients should be highly suspected as SDAVF and confirmed by spinal vascular angiography.
Hong thought spinal arteriovenous shunts below the conus constitute three types of lesions, including filum terminale arteriovenous fistulae, radicular arteriovenous shunts and spinal dural arteriovenous fistulae,12 and we also believe determining that the feeding artery and/or cutting off arteriovenous connection are key for treating spinal arteriovenous shunts.8 It is a significant feature that SDAVF is far away from the spinal cord4 and endovascular embolisation could be achieved safer and more effective than in thoracolumbar segment.8 First, feeding arteries are tortuous and numerous in thoracolumbar segment, which is difficultly superselected; however, the microcatheter in sole and thick artery can be more easily placed near to orificium at sacral shunts, as the thick internal iliac artery is most common feeding artery.13 14 In our cohort, frontal, lateral, 3-D rotational, working position and hand push imagings were necessary before embolisation, and we did not found any cases where the supplying artery also supplied a radiculopial artery. Second, venae terminalis is far away from spinal cord and perimedullary venous network,15 so it is more comfortable and safer that the embolic agents can be flowed into the draining vein about 0.5–1 cm length at SDAVF.
The optimal management strategy to cure sacral AV fistulae seems to be controversial.16 The main therapeutic options consist of microsurgery17 18 and endovascular embolisation. Surgical disconnection has been reported as an effective choice, cutting off the draining vein, which effectively eliminates venous hypertension, without occlusion of the actual fistula itself.18 With the development of interventional techniques, endovascular embolisation has been becoming the mainstream treatment19 20 and preferred choice, especially in the past 5 years for our team. Onyx-18 was chosen as the embolic agent for all cases in our cohort because its polymerisation process occurs in a much slower, more controlled fashion.20 According to our hands-on experience, the precipitation process occurs in a cohesive, non-adhesive fashion at the leading edge of the flow of embolic material, from peripheral to central, and requires approximately 3 min to complete. This, in effect, enables our interventionalist to redirect the flow of embolic material cross over the fistulous shunt and to penetrate into the vein of terminale; meanwhile, it does not readily adhere to the delivery microcatheter.21
In our cohort, six patients treated by microsurgery had no recurrence or complications, even two of them were recrudescent after the first endovascular embolisation. For microsurgery, intraoperative ICG can help the surgeon to identify the engorged and tortuous intradural filum terminale vein.15 Determining the relationship between fistula and sacral canal location carefully and following the engorged and tortuous intradural filum terminale vein, we deem the surgery would not be too complicated. However, its complications, including operation trauma, the length of recovery wound infection and deep venous thrombosis, should cause alarm and attention.22 In our team, our endovascular embolisation brought less trauma and shorter hospital stays, compared with microsurgery, and also had a satisfying complete embolisation rate (80.0%, 24/30). Meanwhile, early anticoagulation and anticoagulation treatment and rehabilitation training can be carried out, usually on the second day after endovascular embolisation.
Conclusion
The rate of misdiagnosis of SDAVF is very high. The treatments, including endovascular embolisation microsurgical fistulectomy, are all safe and effective. A suitable treatment can significantly improve the spinal cord function in the short term.
Data availability statement
No data are available. All free text entered below will be published.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by ethics committee of Huashan Hospital (No. 20120327). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
All contributors are listed in the author list, and no additional acknowledgement needs to be given.
Footnotes
YD and XQ are joint first authors.
Contributors YD: draft a paper and study design; XQ: performing operation; QC: follow-up management; BX, QA, YL and YH: assisting operation and data collection; GC: performing operation and approve the final paper for publication and Guarantor: GC is responsible for the overall content as guarantor.
Funding Funding for this study was provided by the Natural Science Foundation of China (No. 82071313), China; The Innovation Foundation of Huashan hospital (NO.2024CX04).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}