

Several randomised controlled trials (RCTs)1–5 have established 3-month efficacy and safety of endovascular thrombectomy (EVT) in treating patients with acute ischaemic stroke (AIS) with a large infarct core and low Alberta Stroke Program Early Computed Tomographic Scores (ASPECTS), between 3 and 5. Despite EVT, these patients have a higher rate of mortality and unfavourable outcomes at 3 months, delayed recovery or secondary deterioration.6 The long-term outcomes for these patients remain largely uncertain and unexplored.
Recently, the SELECT-2, TESLA and TENSION trials have reported 1-year follow-up outcomes. The SELECT-2 study recruited patients (age 18–85) who presented with AIS resulting from occlusion of the internal carotid artery or the first segment of the middle cerebral artery. Participants had a large ischaemic core and an ASPECTS between 3 and 5. The size of the ischaemic core on CT or MRI perfusion was at least 50 mL. These patients were treated with EVT in conjunction with medical management (MM) versus MM alone within 24 hours of stroke onset. At the 1-year follow-up, the mortality rate was 45% (77 out of 170 patients) in the EVT group compared with 52% (83 out of 159 patients) in the MM-only group, yielding a relative risk of 0.89 (95% CI 0.71 to 1.11). However, the EVT group had better functional outcomes.7 TESLA trial presented its 1-year follow-up findings at the 2024 International Stroke Conference.8 This study enrolled 300 patients with AIS from anterior circulation large vessel occlusion (LVO) with large infarcts (ASPECTS of 2–5) within 24 hours of onset in 47 hospitals in the USA. The 1-year follow-up showed that the EVT group demonstrated a significantly higher utility-weighted modified Rankin Scale score compared with the MM group (3.654±0.217 vs 2.776±0.172). Additionally, quality of life, assessed by the EuroQol Five Dimensions Five Level Questionnaire (EQ-5D-5L), was notably superior in the EVT group relative to the MM group (60.3±28.7 vs 49.3±24.2, p=0.0031). The proportion of patients achieving a mRS of 0–2 at 1 year was significantly greater in the EVT group compared with the MM group (OR 3.49; 95% CI 1.74 to 7.00). This is in comparison to the study’s findings at 90 days, which showed no difference between the two groups, suggesting a delayed recovery.9 The 1-year mortality rates were 43% in the EVT group and 46.6% in the MM group (p=0.418). The TENSION trial included 253 large core patients (ASPECTS 3–5) from LVO in the anterior circulation within 12 hours of onset from 40 hospitals in Europe and one in Canada. Results showed that the EVT group had a better functional outcome indicated by quality of life at 1 year compared with MM only (0.7 (IQR 0.4–0.9) vs 0.4 (0.2–0.7)), with the mortality rate remaining unchanged between the EVT and MM groups (43.3% vs 49.4%).10
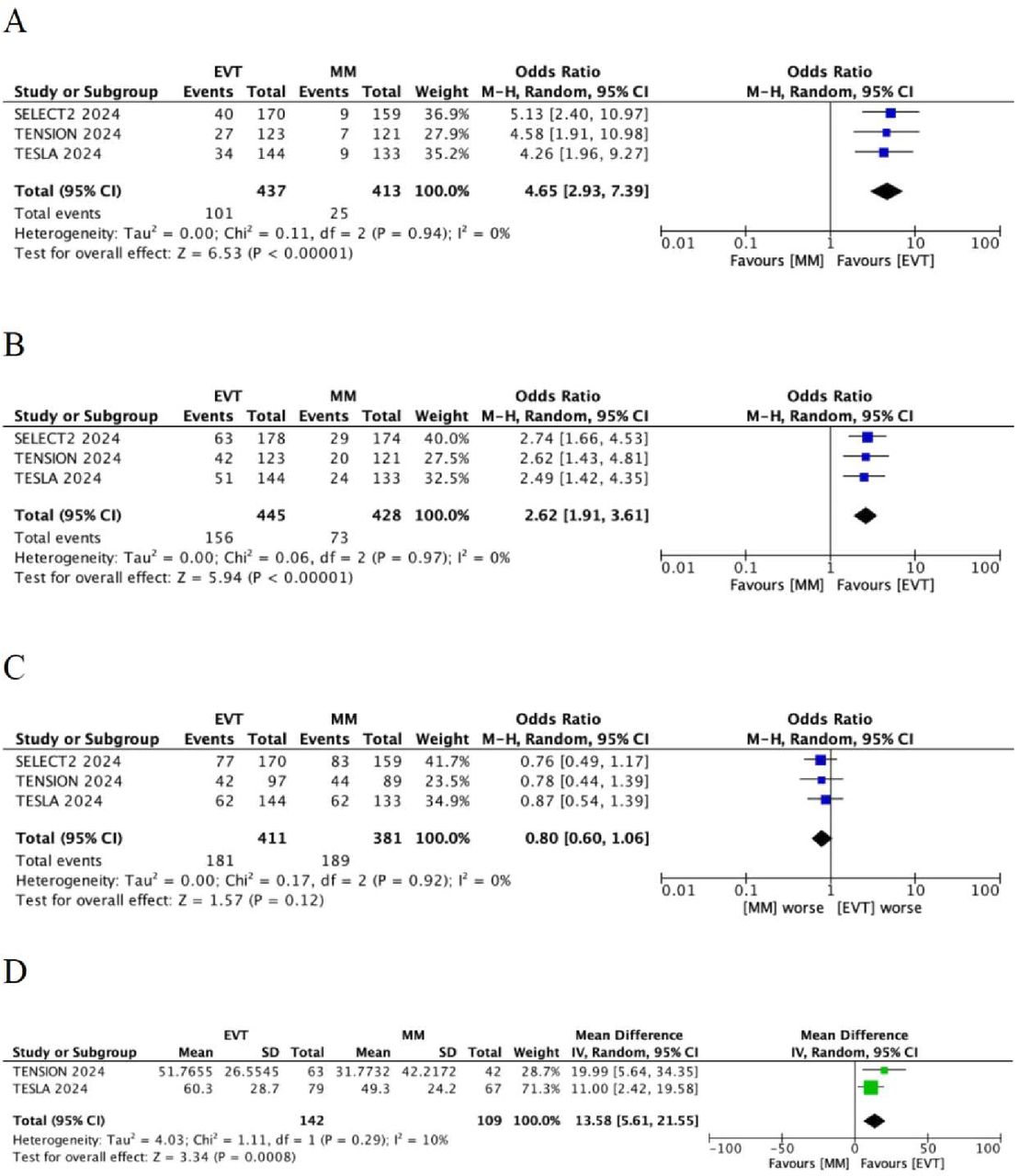
In this meta-analysis of pooled data from the SELECT-2, TESLA and TENSION trials, we found that the OR for 1-year functional independence (mRS 0–2) was 4.65 (95% CI 2.93 to 7.39) and 1-year independent ambulation (mRS 0–3) was 2.62 (95% CI 1.91 to 3.61). Furthermore, EQ-5D analysis pooled from TENSION and TESLA studies revealed a 13.58-fold increase (95% CI 5.61 to 21.55) in quality of life at 1 year favouring EVT. There was no difference in mortality at 1 year (OR 0.80, 95% CI 0.60 to 1.06, figure 1).

Meta-analysis of the efficacy and safety outcomes of three randomised trials. (A) 1-year functional independence (mRS 0–2); (B) 1-year independent ambulation (mRS 0–3); (C) 1-year mortality; (D) 1-year quality of life assessed by EQ-5D. EVT, endovascular thrombectomy; MM, medical management. mRS, modified Rankin Scale; EQ-5D, EuroQol Five Dimensions Questionnaire.
The meta-analysis reveals a significant and consistent efficacy of EVT in patients with AIS with a large infarct core. The pooled ORs for achieving functional independence (mRS 0–2) and independent ambulation (mRS 0–3) at 1 year post-EVT remarkably favoured those who received EVT. Furthermore, the findings indicate that EVT significantly enhanced patients’ quality of life at the 1-year follow-up. EVT not only improved motor recovery but also the overall quality of life for survivors.
In comparison, the analysis revealed no statistically significant difference in 1-year mortality rates between the EVT and MM groups. The benefit of EVT did not improve the rate of survival. Its primary advantage lies in facilitating functional recovery among survivors. This observation aligns with the natural progression of severe stroke, where many patients experience higher mortality rates irrespective of the interventions employed. Nevertheless, for those who do survive, EVT appears to enhance the likelihood of achieving greater independence.
Despite these encouraging findings, several critical considerations must be addressed. First, the variability in infarct size and location, along with the difference in defining a ‘large core’ across various studies, may restrict the applicability of these results. Second, although EVT has demonstrated functional benefits, its effects on secondary complications, such as haemorrhagic transformation or the progression of disability, require further exploration in a larger patient population with standardised long-term follow-up. Third, the cost-benefit ratio of providing EVT to a broader AIS patient population with a large core infarction necessitates further investigation, particularly in places with limited stroke care resources. Lastly, the three trials included in this meta-analysis did not include patients with ASPECTS of 0–2, constraining the applicability of our findings to this specific subgroup, which may demonstrate distinct risk profiles and recovery trajectories.
In summary, the available evidence indicates that EVT may improve 1-year functional outcomes in those patients with AIS with a large infarct core. Such treatment did not improve or worsen the mortality. These results perhaps offered enough evidence for stroke centres to revise their acute treatment protocols. Future investigations should prioritise the identification of patient subgroups that are likely to benefit the most from EVT, optimisation of post-thrombectomy care and exploration of strategies aimed at reducing mortality among high-risk populations.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors YS was responsible for the study concept and design. YZ, DW and YS collected and analysed the data. YZ and YS contributed to drafting the initial manuscript. DW and YS critically revised the manuscript for important intellectual content. YS provided supervision throughout the project. All authors reviewed and approved the final manuscript. YS serves as the guarantor for this work, taking full responsibility for the integrity of the study and the accuracy of the data analysis.
Funding This study was funded by Shenyang Science and Technology Bureau (22-321-33-55, L190082 and L230149).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.





{kind=link}