

Abstract
Background Stroke aetiology remains cryptogenic in a relevant proportion of patients with acute ischaemic stroke (AIS). We assessed whether enhanced diagnostic workup after AIS yields a higher rate of prespecified pathological findings compared with routine diagnostic care in-hospital.
Methods Hospitalised patients with AIS were prospectively enrolled in the investigator-initiated observational HEart and BRain Interfaces in Acute Ischaemic Stroke (HEBRAS) study at the Charité, Berlin, Germany. Patients with AIS without known atrial fibrillation (AF) underwent cardiovascular MR imaging (CMR), MR-angiography of the aortic arch and prolonged Holter-ECG monitoring on top of routine diagnostic care.
Results Among 356 patients with AIS (mean age 66 years, 37.6% female), enhanced workup yielded a higher rate of prespecified pathological findings compared with routine care (17.7% vs 5.3%; p<0.001). Consequently, fewer patients were classified as cryptogenic after enhanced diagnostic workup (38.5% vs 45.5%, p<0.001). Routine care included echocardiography in 228 (64.0%) patients. CMR was successfully performed in 292 (82.0%) patients and revealed more often a prespecified pathological finding compared with routine echocardiography (16.1% vs 5.3%). Furthermore, study-related ECG monitoring (median duration 162 hours (IQR 98–210)) detected AF in 16 (4.5%) patients, while routine monitoring (median duration 51 hours (IQR 34–74)) detected AF in seven (2.0%) patients.
Conclusions Enhanced diagnostic workup revealed a higher rate of prespecified pathological findings in patients with AIS compared with routine diagnostic care and significantly reduced the proportion of patients with cryptogenic stroke.
Trial registration number NCT02142413.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Routine diagnostic care in-hospital does not allow a definite conclusion on stoke aetiology in a relevant proportion of patients with acute ischaemic stroke. Cardiovascular MRI and prolonged Holter-ECG are not part of clinical routine, but might be useful to improve aetiological classification after stroke.
WHAT THIS STUDY ADDS
In this prospective observational trial, enhanced cardiac workup led to a more than threefold increase in pathological findings and significantly reduced the rate of cryptogenic strokes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
More accurate assessment of stroke aetiology may improve secondary prevention strategies in the future and thus help to reduce cardiovascular disease burden.
Introduction
The efficacy of secondary prevention after acute ischaemic stroke (AIS) depends on accurate and early determination of stroke aetiology.1 Despite its well-known shortcomings, the long-established TOAST (Trial of ORG 10172 in Acute Stroke Treatment) criteria remain the most widely used aetiological classification system in clinical routine.2 3 Dating back to 1993, the classification is essentially based on then-available diagnostic means, mainly cerebral CT and ultrasound of the brain-supplying arteries.2 Since then, additional diagnostic techniques have evolved, and the concept of embolic stroke of undetermined source (ESUS) was introduced to facilitate clinical research in the field of cryptogenic strokes with presumably (cardio)embolic origin.4 Yet, to date, there is no universal consensus regarding the recommended diagnostic procedures and the extent of cardiovascular evaluation to determine stroke aetiology,5 6 even in healthcare systems with standardised nationwide stroke unit systems.7 8 For example, a recent investigation has found transesophageal echocardiography (TEE) to yield a higher number of treatment-relevant findings compared with transthoracic echocardiography (TTE) in patients with undetermined cause of stroke, most often due to detection of patent foramen ovale (PFO).9 However, TEE is a semi-invasive procedure and is typically provided only to a small proportion of patients with AIS.10 11 With adequate assessment of the left atrium and the aortic arch being necessary to rule out high-risk sources of cardioembolism,6 cardiovascular MR imaging (CMR) has been found feasible in selected patients with AIS and has become a complimentary diagnostic method to the clinical gold standard echocardiography.12–14 With regard to the detection of arrhythmias, prolonged ECG monitoring has been found to increase the rate of patients diagnosed with atrial fibrillation (AF) after AIS.5 15 However, there is no randomised controlled trial demonstrating a benefit of prolonged ECG monitoring in secondary stroke prevention.16 17
In the prospective HEart and BRain Interfaces in Acute Ischaemic Stroke (HEBRAS) study, we aimed to investigate whether an enhanced approach for diagnostic workup after AIS, consisting of CMR, contrast-enhanced MR-angiography of the aortic arch, and prolonged Holter-ECG (for up to 10 days) (1) increases the rate of pathological findings relevant for stroke aetiology compared with routine diagnostic care and (2) leads to a significant reduction in the proportion of patients with cryptogenic stroke aetiology.18
Methods
Study design
The design of the study including primary and secondary outcomes, and a definition of cardiac pathologies regarded relevant for stroke aetiology were published before completing recruitment.18 Adult patients admitted to the Campus Benjamin Franklin of the Charité with imaging-proven AIS and without a history of AF or AF detection prior to study enrolment were eligible to participate after providing written informed consent. Enhanced diagnostic workup consisted of additional CMR (including cardiac MRI and contrast-enhanced MR-angiography of the aortic arch) and an additional Holter-ECG for up to 10 days (starting immediately after enrolment in-hospital and including up to 5 days after hospital discharge). CMR examinations were assessed centrally by radiologists, being aware of patients’ sex, age and the participation in the HEBRAS study. Echocardiography was performed as part of the clinical routine by indication of the treating neurologists and was conducted and assessed by cardiologists regularly unaware of CMR results. The study protocol with a detailed description of all inclusion and exclusion criteria, MRI (3 Tesla MR scanner TIM TRIO, Siemens, Erlangen, Germany) and MRI parameters, study ECG (CardioMem®4000, GETEMED AG, Teltow, Germany), core lab analysis (German Centre for Cardiovascular Research (DZHK), Partner Site Göttingen, Germany) and study follow-up (conduced at three and twelve months after the index stroke) was published before.18 A summary of respective information can be found in the online supplemental file.
Supplementary data
Study outcomes
The primary outcome measure of the HEBRAS study was the rate of pathological findings relevant to stroke aetiology in patients with AIS obtained by enhanced diagnostic workup in comparison to findings obtained by routine diagnostic care in this cohort of patients.18 The primary hypothesis was that the detection rate of pathological findings can be increased by undergoing enhanced diagnostic workup. The key secondary outcome of HEBRAS was the potential benefit of prolonged continuous ECG-monitoring in patients with AIS by assessing the proportion of patients with first detected paroxysmal AF by prolonged Holter-monitoring in-hospital and for up to 5 days after discharge. For primary and secondary analyses, results of routine diagnostic care and results of enhanced diagnostic care were evaluated in the same cohort of patients.
Definition of stroke aetiology
Stroke aetiology was determined according to TOAST and ESUS criteria.2 4 Stroke subtype classification was performed by two investigators (SH, CHN). The following cardioaortic sources of embolism were prespecified as relevant based on the original publications for TOAST and ESUS criteria2 4: paroxysmal, persistent or permanent AF, sick-sinus-syndrome, bacterial or non-bacterial endocarditis, left-sided intracardiac thrombus or tumour, prosthetic heart valve, higher-grade mitral valve stenosis, left ventricular akinetic segment(s), aortic plaque of ≥4 mm or left ventricular ejection fraction (LVEF) <45% according to TTE or CMR (see online supplemental file for details of LVEF assessment). Myocardial segmentation and nomenclature followed the recommendations of the American Heart Association.19
Sample size calculation and statistical analysis
A sample size of 475 patients was initially assumed to provide a power of 79% to detect a difference in the number of strokes classified as cryptogenic (from 30% after routine diagnostic care to 25% after enhanced diagnostic workup with an assumed 13% of discordant pairs and an expected drop-out rate of about 20%) using a McNemar’s Test and a two-sided significance level of α=0.05.18 The prespecified interim analysis after the inclusion of 264 patients led to a readjustment of the sample size (368 patients).
The analysis of the primary hypothesis was tested in all HEBRAS patients (‘whole cohort’), following the ‘intention to diagnose’ principle. Furthermore, we tested the study hypothesis following a ‘per-protocol’ approach in the subgroup of patients who underwent all diagnostic procedures to be qualified as ESUS patients (‘ESUS cohort’). This required brain imaging (CT or MRI), Holter-ECG >20 hours (stroke unit and/or Holter-ECG monitoring), imaging of brain-supplying arteries and echocardiography (TTE and/or TEE) in routine diagnostic care as well as enhanced diagnostic workup (including study-specific Holter-ECG and CMR).20 21 A sensitivity analysis was carried out defining an LVEF <30% (instead of <45%) as a relevant pathological finding.
Results are reported as frequencies and percentages for categorical variables. In the case of continuous variables, mean and SD are reported for sufficiently normally distributed data or median and limits of IQR for quantitatively skewed variables. In the case of categorical variables and independent samples, Pearson’s χ2 test was used, whereas the Mann-Whitney U test was implemented as a rank-sum test for ordinal variables. McNemar’s test was used for the comparison of paired samples with dichotomised variables. Data were analysed using SPSS statistics V.27 (IBM). To visualise changes in aetiological stroke classification based on routine diagnostic care and enhanced diagnostic workup, respectively, we created a Sankey diagram using the web-based tool SankeyMATIC.
Results
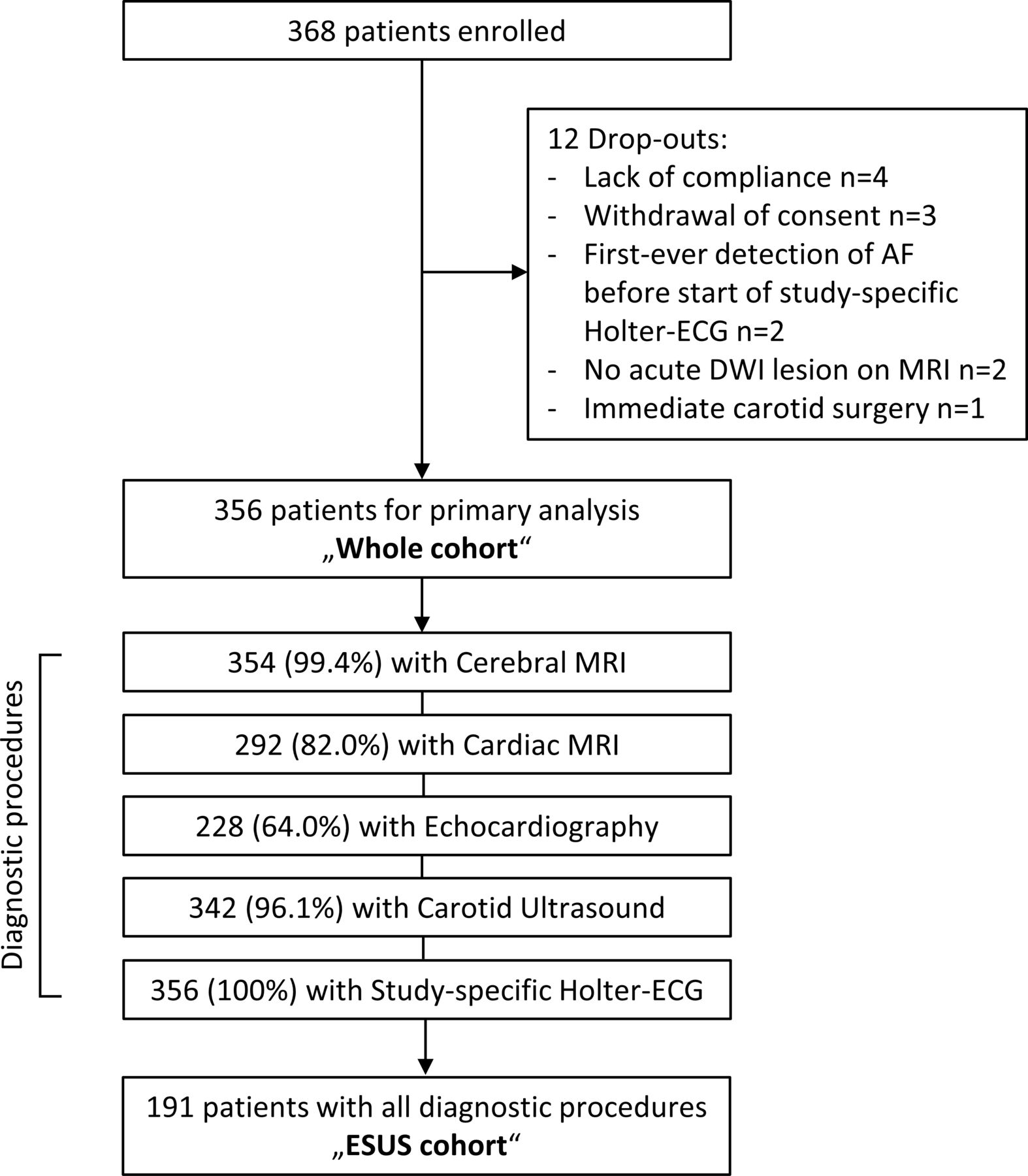
Between May 2014 and February 2017, 368 patients with AIS provided written informed consent for participation in the HEBRAS study. Excluding 12 drop-outs (3.3%), 356 patients were included in the primary analysis (‘whole cohort’, figure 1). Mean age was 66 years (SD 12, range 24–91) and 134 (37.6%) patients were of female sex. Median National Institutes of Health Stroke Scale score on admission was two points (IQR 1–4). Median mRS on admission was two (IQR 1–3). Intravenous thrombolysis was administered in 66 (18.5%) patients and mechanical thrombectomy was performed in three (0.8%) patients. A detailed description of baseline characteristics can be found in table 1.

Study flow chart. AF, atrial fibrillation; DWI, diffusion-weighted imaging; ESUS, embolic stroke of undetermined source.
Baseline characteristics of all 356 patients with AIS included in the HEBRAS study (‘whole cohort’) and the subgroup of 191 patients undergoing brain imaging, stroke unit or Holter-ECG monitoring >24 hours, imaging of extracranial and intracranial brain-supplying arteries and echocardiography (TTE and/or TEE) according to routine diagnostic care as well as completed enhanced diagnostic workup (‘ESUS cohort)
Routine diagnostic care in-hospital
In total, 354 (99.4%) of 356 patients underwent brain MRI and had an acute DWI lesion corresponding to AIS-related clinical deficits. In the remaining two patients, ischaemic stroke was proven by brain CT. A 12-lead ECG was performed in the emergency department or immediately on admission to the stroke unit in 353 (99.2%) patients. Overall, 352 (98.9%) patients were admitted to the stroke unit and underwent monitor-based ECG recording of 52 hours (IQR 35–74). Four patients not admitted to the stroke unit received 24-hour Holter-ECG monitoring according to clinical routine. Taken together, the median duration of ECG monitoring during routine diagnostic care was 51 hours (IQR 34–74). In total, 355 (99.7%) patients received imaging of the extracranial brain-supplying arteries (using duplex sonography in 344 (96.6%), MR-angiography in 90 (25.3%) and CT-angiography in 29 (8.1%) patients). Imaging of the intracranial brain-supplying arteries was performed in all MRI examinations as part of the routine protocol. All patients also received transcranial duplex sonography. Echocardiography was performed in 228 (64.0%) patients, including 127 (35.7%) receiving TTE, 195 (54.8%) receiving TEE and 94 (26.4%) patients receiving both. A comparison of baseline characteristics between study patients who underwent echocardiography and those who did not can be found in the online supplemental material and in online supplemental table 1. Taken together, 228 (64.0%) patients underwent diagnostic workup including echocardiography, brain imaging, ECG monitoring for at least 24 hours and imaging of brain-supplying arteries.
Results of routine diagnostic care in-hospital
Routine diagnostic care in-hospital led to the detection of 103 pathological findings (a priori defined as relevant for stroke aetiology) in 96 (27.0%) of 356 patients. Echocardiography detected 13 relevant pathological findings in 12 (3.4%) patients. In detail, TTE detected at least one akinetic left ventricular segment in 5 (1.4%) of 356 patients, and an LVEF <45% in 2 (0.6%) patients. TEE detected an aortic plaque >4 mm in 5 (1.4%) patients and a type-A aortic dissection in 1 (0.3%) patient. Moreover, although not defined as a relevant pathological finding at the time the study was designed, a PFO was detected in 41 (11.5%) patients, an atrial septal defect in 2 (0.6%) patients and an atrial septal aneurysm in 1 (0.3%) patient. Routine imaging of the brain supplying arteries showed ≥50% ipsilateral arterial stenosis or occlusion in 83 (23.3%) patients. Routine cardiac monitoring revealed a first-ever episode of AF in seven (2.0%) patients.
Stroke aetiology according to routine diagnostic care in-hospital
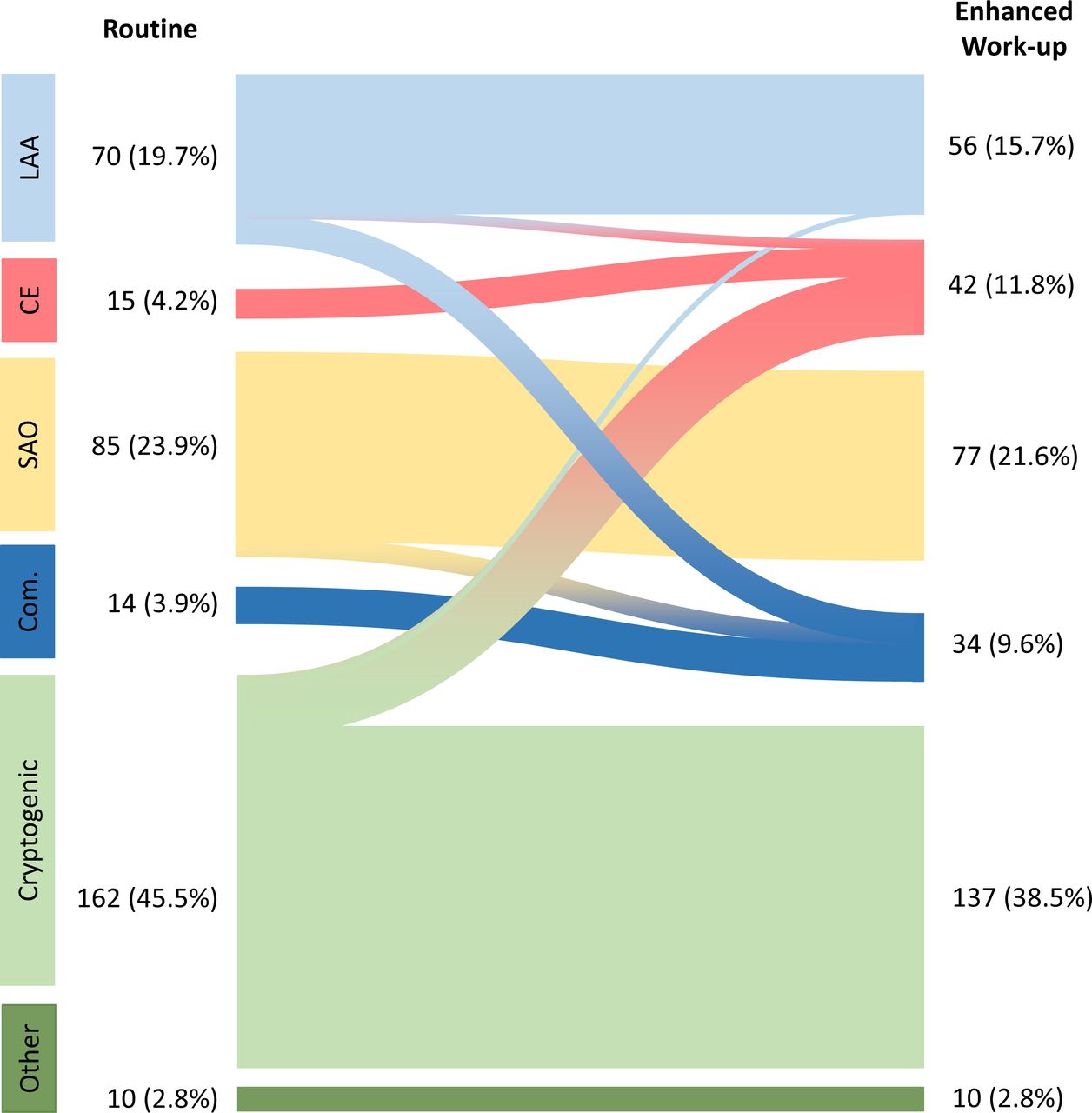
Aetiology of AIS was categorised as ‘large-artery atherosclerosis’ in 70 (19.7%) of 356 patients, as ‘cardioembolic’ in 15 (4.2%) patients, as ‘small-artery occlusion’ in 85 (23.9%) patients and 10 (2.8%) patients were found to have another determined aetiology according to routine diagnostic care. The remaining 176 (49.4%) patients were classified as ‘cryptogenic’ at hospital discharge (‘stroke of undetermined aetiology’).2 Of those, 14 (3.9%) patients were found to have competing aetiologies, leaving 162 (45.5%) patients with cryptogenic stroke.2 As 45 of these 162 patients did not receive echocardiography in clinical routine, 117 (32.9%) patients fulfilled the ESUS criteria. A detailed description of the subcategories can be found in the online supplemental file.
Feasibility of enhanced diagnostic workup
In total, 292 patients (82.0%) underwent CMR, of which 6 examinations had to be terminated prematurely according to the patients’ will. Individual reasons not to undergo CMR are described in the online supplemental material. Likewise, baseline characteristics of those patients who received CMR and those who did not are presented in online supplemental table 2. Contrast agent was administered in 247 (69.4%) CMR examinations. In total, 239 (67.1%) of 356 patients completed CMR including MR-angiography of the aortic arch. Median examination time for the complete CMR protocol (including contrast-enhanced sequences) was 41 min (IQR 35–48). Median time from stroke onset or time last seen well to CMR was 82.5 hours (IQR 58–112) and median time from admission to CMR was 67 hours (IQR 44–92).
Study-specific Holter-ECG was performed in-hospital in all 356 patients for up to 5 days (median duration 72.5 hours (IQR 47–116)), and in 241 (67.7%) patients after hospital discharge starting in-hospital (median duration 120 hours (IQR 96–120)). The total duration of study-specific Holter-monitoring was 162 hours (IQR 98–210). Median time from stroke onset or last seen well to start of Holter-ECG monitoring was 51 hours (IQR 32–75), and median time from admission to Holter-ECG monitoring was 30 hours (IQR 20–52). In total, 182 (51.1%) of 356 patients completed CMR including MR-angiography of the aortic arch and underwent Holter-ECG monitoring in-hospital and after hospital discharge.
Results of enhanced diagnostic workup
Enhanced diagnostic workup led to the detection of 73 pathological findings in 67 (18.8%) of 356 study participants. CMR detected 60 pathological findings in 47 (13.2%) patients. In detail, at least 1 akinetic left ventricular segment was detected in 14 (3.9%) patients, an LVEF <45% in 40 (11.2%) patients, an intraventricular thrombus in 3 (0.8%) patients, a dilated cardiomyopathy in 2 (0.6%) patients and an intracardiac tumour (intraventricular lipoma) in 1 (0.3%) patient. With regard to the sensitivity analysis implementing an LVEF <30% as a high-risk cardioembolic source, an LVEF <30% was present in 8 (2.2%) patients. Study-specific contrast-enhanced extracranial MR-angiography of the brain supplying arteries including the aortic arch detected a severe aortic plaque ≥4 mm in 1 (0.3%) patient (who was not examined by TEE). Routine echocardiography was performed in 27 of those 47 patients with prespecified pathological findings in CMR, revealing an akinetic left ventricular segment in 5 patients, an LVEF <45% in 2 patients, a severe aortic plaque ≥4 mm in 5 patients and a type-A aortic dissection in 1 patient.
The study-specific Holter-ECG detected a first episode of AF in 16 (4.5%) patients, 6 of which were also detected during routine diagnostic care. Taken together, enhanced diagnostic workup led to a detection of relevant pathological findings in an additional 35 (9.8%) patients compared with routine diagnostic care alone.
Primary and secondary outcomes of the HEBRAS study
Verifying the primary hypothesis, the rate of prespecified pathological findings relevant to classification of stroke aetiology was increased after enhanced diagnostic workup compared with routine diagnostic care in the whole cohort (103 findings (28.1%) in routine diagnostic care vs 161 findings (45.2%) according to enhanced workup). In total, a first episode of AF was detected in 16 patients by study-specific Holter-ECG vs 7 patients according to routine diagnostic care (4.5% vs 2.0%; p=0.01). Out of those seven patients with AF according to routine diagnostic care, one was not detected by study-specific Holter-ECG. On the other hand, study-specific Holter-ECG detected paroxysmal AF in 10 patients without AF detection according to routine diagnostic care. This corresponds to a proportion of 10 (2.8%) out of 356 patients with first detected paroxysmal AF by study-specific Holter-ECG.
Stroke aetiology according to routine diagnostic care and enhanced workup
Enhanced diagnostic workup led to a change in aetiological classification in 48 (13.5%) of all study patients (see figure 2 and online supplemental file for details). The proportion of patients categorised as cryptogenic at hospital discharge was significantly reduced by enhanced diagnostic workup (38.5% vs 45.5% according to routine diagnostic care, p<0.001). This observation remained significant in the ESUS cohort (42.9% vs 50.8% according to routine diagnostic care, p<0.001). A sensitivity analysis using LVEF <30% as a pathological finding (instead of <45%) resulted in a 4.5% reduction of the proportion of patients classified as ‘cryptogenic’ in the whole cohort by enhanced diagnostic workup (41.0% vs 45.5% according to routine diagnostic care, p<0.001) and in a 5.3% reduction of the proportion of patients classified as ‘cryptogenic’ in the ESUS cohort (45.5% vs 50.8% according to routine diagnostic care, p=0.001).

Aetiological classification in 356 patients with AIS considering routine diagnostic findings (‘routine’) and considering enhanced diagnostic workup (‘enhanced workup’); including cardiac MRI, MR-angiography of the aortic arch and study-specific Holter ECG for up to ten days. AIS, acute ischaemic stroke; CE, cardioembolism; Com., competing aetiology; LAA, large-artery atherosclerosis; SAO, small-artery occlusion.
Discussion
The primary finding of the prospective, observational HEBRAS study is that enhanced diagnostic workup significantly improves the detection of pathological findings after AIS, proving the prespecified study hypothesis. Taken together, application of CMR and prolonged Holter-monitoring (in-hospital and up to 5 days after discharge vs routine monitoring in-hospital) increased the rate of prespecified pathological findings relevant to stroke aetiology by 17%. Subsequently, enhanced diagnostic workup led to a significant decrease of patients with AIS diagnosed with cryptogenic stroke according to TOAST criteria at hospital discharge.
In HEBRAS, CMR could be performed in 82% of the included patients who had a stroke, which is well in line with previously reported rates.14 CMR was able to detect more cardiac pathologies such as intracardiac thrombi or tumours, and revealed a higher rate of akinetic myocardial segments compared with routine diagnostic care. However, we cannot draw definite conclusions on implications for improved secondary stroke prevention. Future trials are needed to investigate a possible therapeutic relevance of an enhanced diagnostic approach. Moreover, assessing LVEF by CMR analysis found a significantly higher rate of reduced LVEF both according to the definition of the study protocol (LVEF <45%) and to define ESUS (<30%).18 Indeed, a reduced LVEF was the most frequent pathological finding using CMR (online supplemental table 3). It has been shown that both the presence of akinetic myocardial segments as well as reduced LVEF promotes intracardiac thrombus formation.22 However, there is no clear recommendation on the therapeutic consequences of these conditions in the absence of thrombus or AF.23 This might change in the future, as a subgroup analysis of the NAVIGATE ESUS trial found rivaroxaban to be superior to acetylsalicylic acid in reducing the risk of recurrent stroke or systemic embolism.24 Nevertheless, identification of an akinetic myocardial segment and/or reduced LVEF may already have therapeutic consequences in terms of additional diagnostics (ie, coronary angiography) or change of medication.25 From our perspective, the HEBRAS findings support the notion to consider advanced cardiac imaging like CMR in selected patients with stroke or TIA due to presumed cardioembolism and no identifiable cardioembolic source after routine diagnostic care.
In our analysis, the detection rate of a first AF episode in patients with AIS was more than doubled by the study-specific prolonged Holter-ECG monitoring. In detail, the study-specific Holter-ECG led to an absolute increase in AF detection after stroke of 2.5%. This is in line with the randomised MonDAFIS trial, which demonstrated an absolute increase in AF detection of 1.8% by prolonged Holter-monitoring in-hospital compared with routine monitoring.16 Notably, all first episodes of AF were detected by the study-specific Holter-ECG during the in-hospital stay. Therefore, one might argue that the more thorough the search for AF is performed in-hospital, the less likely might be an additional diagnostic benefit of out-of-hospital rhythm monitoring after AIS.
From a pathophysiological perspective, early assessment and better understanding of stroke aetiology may improve secondary stroke prevention and thereby help to reduce the rate of stroke recurrence. Overall, exclusive findings of HEBRAS would have warranted changes in antithrombotic medication (ie, indication for oral anticoagulation (OAC)) in accordance with current guidelines in 13 (3.7%) patients (due to detection of AF or intracardiac thrombi) and an intensified LDL target in one patient (due to a severe aortic plaque). Regarding AF, we are unable to answer the question whether AF first detected after the index stroke was causal for the index stroke, was present but unnoticed before the stroke or was induced by the index stroke itself.5 26 27 Whether or not enhanced diagnostic workup would translate into improved secondary stroke prevention and subsequent reduction of stroke recurrence was not an aim of the HEBRAS study,18 and deserves further investigation in a large prospective multicentre trial.
Of note, the proportion of patients with AIS classified as ‘competing aetiology’ increased following the enhanced workup in the HEBRAS study, as an additional stroke aetiology was identified in patients who had a stroke already diagnosed with a definite aetiology following routine diagnostic care. It has been repeatedly pointed out that the original TOAST classification comprises three very heterogeneous groups of patients with cryptogenic stroke, namely those with incomplete diagnostics, those with more than one identified cause of stroke and those with no identified cause despite complete investigation.2 28 Therefore, we differentiated between cryptogenic strokes with competing aetiology and cryptogenic strokes without an identified cause.
The following limitations have to be addressed and might mitigate the validity of our results. First, our findings cannot be generalised to all patients with AIS, as patients unable to provide informed consent or patients with previously detected AF were excluded. This indicates a selection bias and might have resulted in the inclusion of younger, less severely affected patients who had a stroke. In addition, 18% of all study participants did not receive CMR. Second, with a median time of 30 hours from hospital admission to the start of the study-specific Holter-ECG, there is a chance that we might have missed the diagnosis of AF in some patients. Third, not all study patients underwent TTE and/or TEE and we cannot exclude a respective selection bias. However, this reflects routine diagnostic care in clinical practice, even in developed countries with a nationwide stroke unit system like Germany.7 8 29 Notably, neither stroke unit certification requirements according to the German nor the European Stroke Organisation include specific recommendations on the use of echocardiography.30 31 Fourth, one might argue that the chosen LVEF threshold (<45% or even <30%) defining a high-risk cardioembolic source is debatable in the absence of a cardiac thrombus.32 Based on a risk model including history of ischaemic stroke, a recent meta-analysis including >20 000 heart failure patients with reduced LVEF and sinus rhythm identified a subgroup of patients with a similar stroke risk to AF patients without OAC.33 Nevertheless, there are no randomised controlled trials demonstrating a benefit of OAC in this population. The same holds true for left ventricular akinetic segments, despite the fact that this finding goes along with a higher chance of thrombus formation.34 However, the recently updated German guidelines on secondary stroke prevention recommend to consider OAC instead of antiplatelet therapy in patients who had an ischaemic stroke with an LVEF <35% and sinus rhythm.35 The relevance of an interatrial septal abnormality for secondary stroke prevention was low at the time the HEBRAS study was designed, as randomised controlled trials (like CLOSURE I, PC trial and RESPECT PFO) did not demonstrate a significant reduction of stroke recurrence in PFO patients and otherwise cryptogenic stroke.36 According to current guidelines, PFO closure should be considered in patients 18–60 years who do not have another identifiable cause of stroke after comprehensive workup. Therefore, TTE is essential in these patients.37 Fifth, besides feasibility, timing and cost-effectiveness are major considerations for CMR.12 14 Prolonged non-invasive ambulatory ECG monitoring for 14 as well as 30 days after cryptogenic stroke was estimated to be highly cost-effective based on data from the EMBRACE trial.38 However, as a cost–benefit analysis was not aim of the HEBRAS study, it is very difficult to draw definitive conclusions on that matter. To the best of our knowledge, no such analysis has been performed on the use of CMR in patients who had a stroke. CMR may be cost-effective in patients with AIS undergoing brain MRI and CMR immediately afterwards, subsequently shortening the in-hospital stay after AIS. Additionally, CMR might be reasonable in a subset of patients with AIS with a high presumed risk of cardioembolic stroke or (undetected) coronary heart disease.
Conclusion
Enhanced diagnostic workup including CMR and prolonged Holter-ECG monitoring resulted in a significant increase of pathological findings compared with routine diagnostic care in a specialised stroke centre. Enhanced diagnostic workup significantly reduced the proportion of patients with AIS categorised as cryptogenic stroke or ESUS. Whether enhanced diagnostic workup after AIS may lead to a reduction of cardiovascular endpoints by improving secondary stroke prevention has to be addressed in future studies.
Data availability statement
Data are available on reasonable request. Individual participant data that underlie the results reported in this article will be available to researchers who provide a methodologically sound proposal beginning at 12 months and ending 5 years after publication. Proposals should be directed to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the study was approved by the Ethics Committee of the Charité—Universitätsmedizin Berlin (EA1/045/14). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
SH is participant in the BIH Charité Clinician Scientist Program funded by the Charité—Universitätsmedizin Berlin, and the Berlin Institute of Health at Charité (BIH). We thank Kristin Simon (former CSB, now BIH) and Tatjana Wittenberg (CSB) for their outstanding support in conducting the study. In addition, we thank Michael Scherf (GETEMED AG, Teltow, Germany) for providing technical support and study ECGs.
Footnotes
CHN and KGH contributed equally.
Contributors CHN and KGH contributed to the design of the study. TK, JH and SH contributed to data acquisition. CHN, KGH, SH and UG performed statistical analysis. CHN, KGH and SH prepared the figures, wrote the first draft of the manuscript and drafted the manuscript. TE performed imaging analysis of CMR. JF performed imaging analysis of brain MRI. NJ, WD, MK and RW were involved in analysis of ECG and Echocardiography. JF and ME contributed major intellectual content and drafted the manuscript. All authors read, drafted and approved the manuscript. KGH accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study was supported by the German Ministry of Education and Research (grant G.2.17, Center for Stroke Research Berlin), by the DZHK (German Center for Cardiovascular Research) (grant B14-035_SE) and by the GETEMED AG, Teltow, Germany by supplying ECG recorders.
Competing interests RW received grants from Deutsches Zentrum für Herz-/Kreislaufforschung, Deutsche Forschungsgemeinschaft, European Union, Bundesministerium für Bildung und Forschung, Medtronic and Boehringer Ingelheim as well as personal fees from Astra, Bayer, Boehringer Ingelheim, CVRx, Daiichi, BMS, Medtronic, Novartis, Pfizer, Pharmacosmos and Servier, all outside the submitted work. ME received funding from DFG under Germany's Excellence Strategy—EXC-2049—390688087, BMBF, DZNE, DZHK, EU, Corona Foundation, and Fondation Leducq. ME reports grants from Bayer and fees paid to the Charité from AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Daiichi Sankyo, Amgen, GSK, Sanofi, Covidien, Novartis, Pfizer, all outside the submitted work. CHN received research grants from German Ministry of Research and Education, German Center for Neurodegenerative Diseases, German Center for cardiovascular Research, and speaker and/or consultation fees from Alexion, Abbott, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer Pharma and Daiichi Sankyo. KGH reports a study grant by Bayer, lecture fees/advisory board fees from Abbott, Amarin, Alexion, AstraZeneca, Bayer, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol-Myers-Squibb, Daiichi Sankyo, Edwards Lifesciences, Medtronic, Pfizer, Portola, Sun Pharma and W. L. Gore & Associates. All other authors declare no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}