

Article Figures & Data
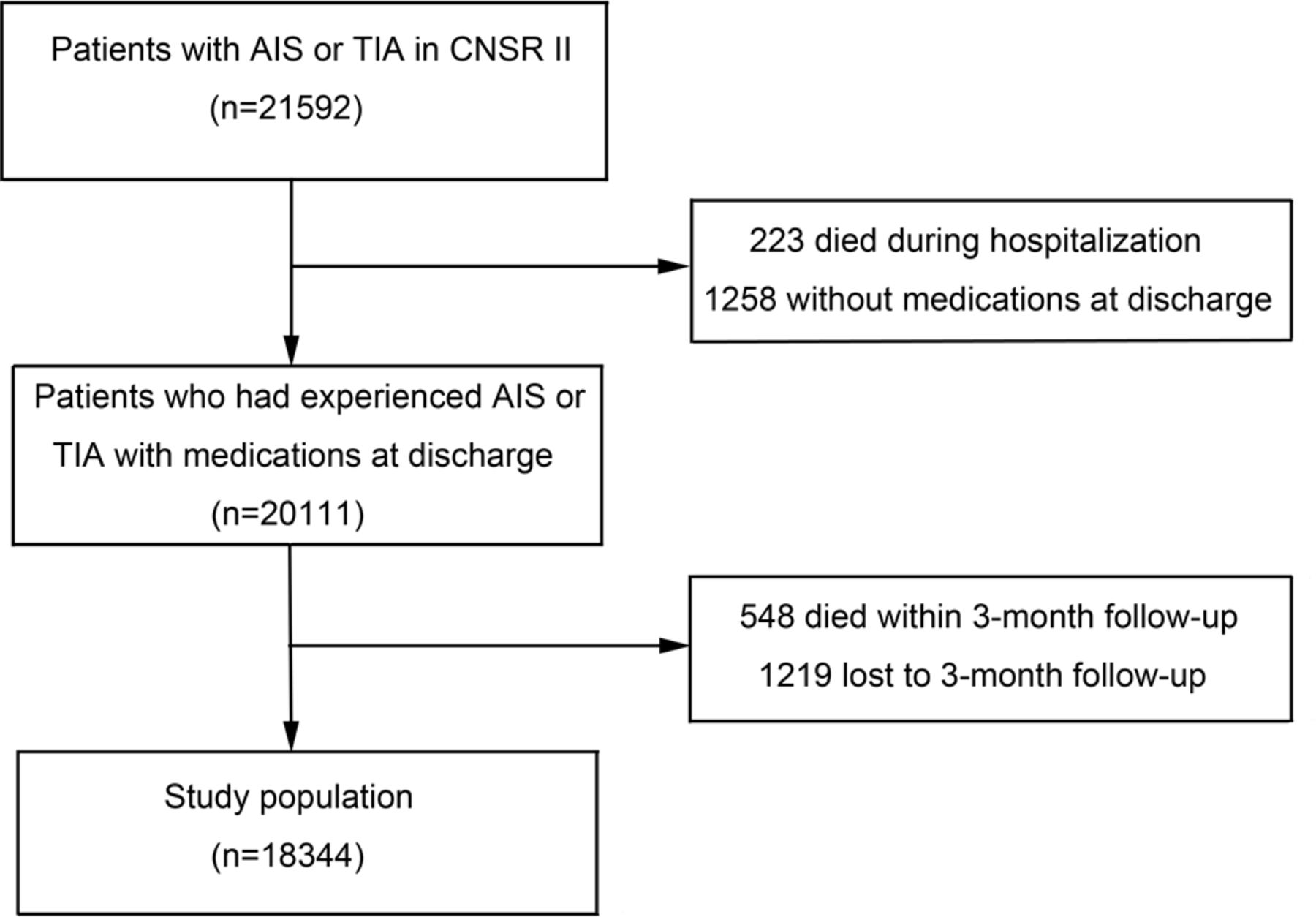
- Figure 1
Flowchart of the study. AIS, acute ischaemic stroke; CNSR II, China National Stroke Registry II; TIA, transient ischaemic attack.
- Figure 2
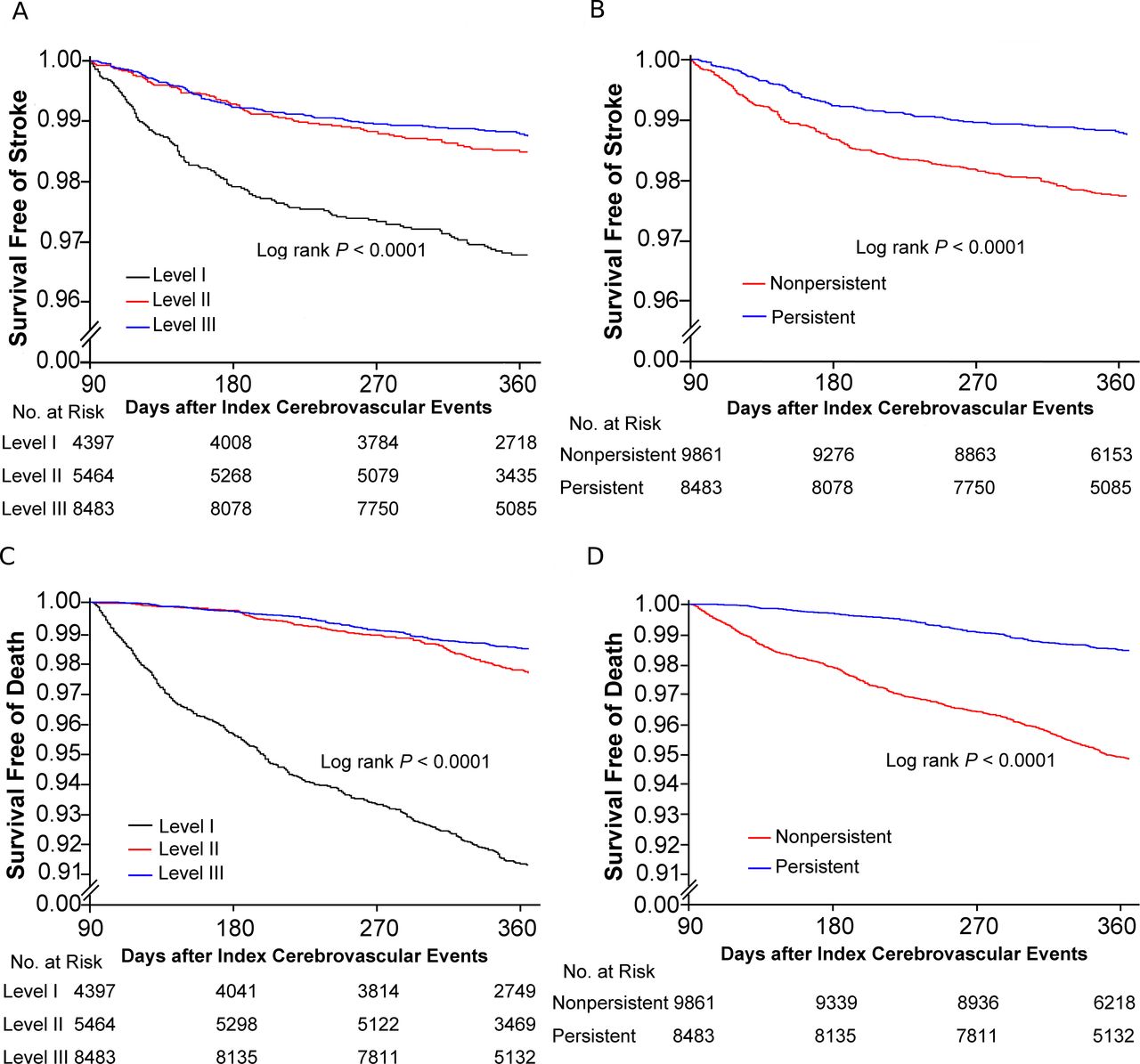
Probability of survival free of recurrent stroke or all-cause death after acute ischaemic stroke or transient ischaemic attack by the composite or regimen persistence. (A) Kaplan-Meier curves of survival free of recurrent stroke by the composite persistence. (B) Kaplan-Meier curves of survival free of recurrent stroke by the regimen persistence. (C) Kaplan-Meier curves of survival free of all-cause death by the composite persistence. (D) Kaplan-Meier curves of survival free of all-cause death by the regimen persistence.


- Table 1
Baseline characteristics in patient level and 3-month composite persistence of the study population
Variables Composite persistence* Overall Level I Level II Level III P value n=18 344 n=4397 n=5464 n=8483 Patient level Age, median (IQR), years 64 (56–73) 67 (58–76) 64 (56–73) 64 (56–73) <0.001 Female, n (%) 6651 (36.3) 1585 (36.1) 2114 (38.7) 2952 (34.8) <0.001 Ethnicity (Han), n (%) 17 789 (97.0) 4246 (96.6) 5285 (96.7) 8258 (97.4) 0.02 Education level, n (%) <0.001 High school or above 5949 (32.4) 1262 (28.7) 1895 (34.7) 2792 (32.9) Middle school 4349 (23.7) 1028 (23.4) 1326 (24.3) 1995 (23.5) Elementary or below 8046 (43.9) 2107 (47.9) 2243 (41.1) 3696 (43.6) Health insurance, n (%) <0.001 UBMIS 9527 (51.9) 2105 (47.9) 2972 (54.4) 4450 (52.5) NRCMS 7197 (39.2) 1905 (43.3) 2016 (36.9) 3276 (38.6) Commercial insurance 58 (0.3) 16 (0.4) 18 (0.3) 24 (0.3) Self-payment 1562 (8.5) 371 (8.4) 458 (8.4) 733 (8.6) Family income per month >3000 yuan
(US$434), n (%)2171 (11.8) 493 (11.2) 710 (13.0) 968 (11.4) 0.006 Medical history, n (%) Hypertension 11 905 (64.9) 2369 (53.9) 4016 (73.5) 5520 (65.1) <0.001 Diabetes 3772 (20.6) 535 (12.2) 1570 (28.7) 1667 (19.7) <0.001 Dyslipidaemia 2320 (12.7) 470 (10.7) 769 (14.1) 1081 (12.7) <0.001 Atrial fibrillation 1103 (6.0) 282 (6.4) 361 (6.6) 460 (5.4) 0.007 Myocardial infarction 439 (2.4) 105 (2.4) 123 (2.3) 211 (2.5) 0.67 Coronary artery disease 2068 (11.3) 491 (11.2) 641 (11.7) 936 (11.0) 0.43 Previous TIA 1002 (5.5) 246 (5.6) 324 (5.9) 432 (5.1) 0.10 Previous stroke 5508 (30.0) 1294 (29.4) 1612 (29.5) 2602 (30.7) 0.21 Ever smoking 8197 (44.7) 1943 (44.2) 2404 (44.0) 3850 (45.4) 0.21 Drinking 5579 (30.4) 1297 (29.5) 1621 (29.7) 2661 (31.4) 0.03 Admission NIHSS score, median (IQR) 3 (1–6) 4 (1–7) 3 (1–6) 3 (1–6) <0.001 Type of disease, n (%) <0.001 Ischaemic stroke 16 563 (90.3) 3894 (88.6) 4950 (90.6) 7719 (91.0) TIA 1781 (9.7) 503 (11.4) 514 (9.4) 764 (9.0) Severity of illness at discharge, n (%) <0.001 mRS >3 3552 (19.4) 965 (22.0) 986 (18.1) 1601 (18.9) mRS ≤2 14 777 (80.6) 3430 (78.0) 4470 (81.9) 6877 (81.1) New stroke within 3 months, n (%) 770 (4.2) 235 (5.3) 193 (3.5) 342 (4.0) <0.001 *Composite persistence was defined as the percentage (0% to 100%) of discharge medication classes that patients were still taking at 3 months. Level I: persistence=0%; level II: 0%<persistence<100%; level III: persistence=100%.
mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; NRCMS, new rural cooperative medical schemes; TIA, transient ischaemic attack; UBMIS, urban basic medical insurance schemes.
- Table 2
Baseline characteristics in hospital level and 3-month composite persistence of the study population
Variables Composite persistence* Overall Level I Level II Level III P value n=18 344 n=4397 n=5464 n=8483 Hospital level Hospital grade, n (%) 0.72 Tertiary 12 472 (68.0) 2968 (67.5) 3719 (68.1) 5785 (68.2) Secondary 5872 (32.0) 1429 (32.5) 1745 (31.9) 2698 (31.8) Region, n (%) <0.001 Eastern 10 947 (59.7) 2678 (60.9) 3360 (61.5) 4909 (57.9) Central 4250 (23.2) 1020 (23.2) 1161 (21.3) 2069 (24.4) Western 3147 (17.2) 699 (15.9) 943 (17.3) 1505 (17.7) Teaching hospital, n (%) 10 276 (56.0) 2502 (56.9) 3046 (55.8) 4728 (55.7) 0.40 Stroke unit, n (%) 10 312 (56.2) 2297 (52.2) 3073 (56.2) 4942 (58.3) <0.001 Hospital beds >1000, n (%) 8725 (47.6) 2047 (46.6) 2731 (50.0) 3947 (46.5) <0.001 No of neurological ward beds >80, n (%) 9830 (53.6) 2116 (48.1) 2892 (52.9) 4822 (56.8) <0.001 *Composite persistence was defined as the percentage (0% to 100%) of discharge medication classes that patients were still taking at 3 months. Level I: persistence=0%; level II: 0%<persistence<100%; level III: persistence=100%.
- Table 3
Outcomes after ischaemic stroke or TIA by 3-month composite persistence
Outcomes Composite persistence N Events,
n (%)Model 1* Model 2† Adjusted HR/OR (95% CI) P value Adjusted HR/OR (95% CI) P value Stroke Level I 4397 134 (3.1) 1.00 (Ref) 1.00 (Ref) Level II 5464 80 (1.5) 0.49 (0.37 to 0.64) <0.001 0.41 (0.31 to 0.54) <0.001 Level III 8483 101 (1.2) 0.40 (0.31 to 0.52) <0.001 0.37 (0.28 to 0.48) <0.001 Composite events‡ Level I 4397 159 (3.6) 1.00 (Ref) 1.00 (Ref) Level II 5464 97 (1.8) 0.50 (0.38 to 0.64) <0.001 0.41 (0.32 to 0.53) <0.001 Level III 8483 125 (1.5) 0.42 (0.33 to 0.53) <0.001 0.38 (0.30 to 0.49) <0.001 All-cause death Level I 4397 367 (8.4) 1.00 (Ref) 1.00 (Ref) Level II 5464 120 (2.2) 0.29 (0.24 to 0.36) <0.001 0.28 (0.23 to 0.35) <0.001 Level III 8483 123 (1.5) 0.20 (0.16 to 0.24) <0.001 0.20 (0.16 to 0.24) <0.001 Disability (mRS=3–5) Level I 3733 595 (15.9) 1.00 (Ref) 1.00 (Ref) Level II 5069 704 (13.9) 0.93 (0.82 to 1.06) 0.26 0.89 (0.77 to 1.03) 0.11 Level III 7762 1022(13.2) 0.88 (0.79 to 0.99) 0.026 0.82 (0.72 to 0.93) 0.003 Composite persistence was defined as the percentage (0% to 100%) of discharge medication classes that patients were still taking at 3 months. Level I: persistence=0%; level II: 0%<persistence<100%; level III: persistence=100%.
HR for stroke, composite events and all-cause death; OR for disability.
*Model 1: adjusted for age and sex.
†Model 2: adjusted for patient and hospital characteristics, including age, sex, ethnicity, education level, health insurance, family income per month, history of hypertension, diabetes, dyslipidaemia, atrial fibrillation, myocardial infarction, coronary artery disease, previous TIA or stroke, ever smoking and drinking, admission NIHSS score, type of disease, severity of illness at discharge, new stroke within 3 months, hospital grade, region, teaching hospital, stroke unit, hospital beds and number of neurological ward beds.
‡Composite events: stroke, myocardial infarction or death from cardiovascular cause.
mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; Ref, reference; TIA, transient ischaemic attack.
- Table 4
Outcomes after ischaemic stroke or TIA by 3-month regimen persistence
Outcomes Regimen persistence N Events,
n (%)Model 1* Model 2† Adjusted HR/OR
(95% CI)P value Adjusted HR/OR
(95% CI)P value Stroke Non-persistent 9861 214 (2.2) 1.00 (Ref) 1.00 (Ref) Persistent 8483 101 (1.2) 0.56 (0.44 to 0.71) <0.001 0.57 (0.45 to 0.73) <0.001 Composite events‡ Non-persistent 9861 256 (2.6) 1.00 (Ref) 1.00 (Ref) Persistent 8483 125 (1.5) 0.58 (0.47 to 0.72) <0.001 0.59 (0.48 to 0.74) <0.001 All-cause death Non-persistent 9861 487 (4.9) 1.00 (Ref) 1.00 (Ref) Persistent 8483 123 (1.5) 0.31 (0.26 to 0.38) <0.001 0.32 (0.26 to 0.39) <0.001 Disability (mRS=3–5) Non-persistent 8802 1299 (14.8) 1.00 (Ref) 1.00 (Ref) Persistent 7762 1022 (13.2) 0.92 (0.84 to 1.00) 0.0545 0.87 (0.79 to 0.97) 0.01 Regimen persistence was referred to an all-or-none measure where patients who continued all discharge medication classes at the 3-month follow-up were considered persistent, whereas patients who discontinued at least one class of discharge medications were considered non-persistent.
HR for stroke, composite events and all-cause death; OR for disability.
*Model 1: adjusted for age and sex.
†Model 2: adjusted for patient and hospital characteristics, including age, sex, ethnicity, education level, health insurance, family income per month, history of hypertension, diabetes, dyslipidaemia, atrial fibrillation, myocardial infarction, coronary artery disease, previous TIA or stroke, ever smoking and drinking, admission NIHSS score, type of disease, severity of illness at discharge, new stroke within 3 months, hospital grade, region, teaching hospital, stroke unit, hospital beds and number of neurological ward beds.
‡Composite events: stroke, myocardial infarction or death from cardiovascular cause.
mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; Ref, reference; TIA, transient ischaemic attack.
Supplementary Materials
Supplementary data
Supplementary data
Supplementary data
Supplementary data
Supplementary data
Additional Files
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.





{kind=link}
{kind=link}