

Abstract
Intravenous thrombolysis is not recommended in anticoagulated patients receiving direct oral anticoagulants (DOACs) and a recent intake within the last 48 hours in US and European guidelines. However, three observational studies now suggest safety of thrombolysis in patients with recent intake of DOACs, and thus support previous experimental data. In this perspective, the current evidence and practical consequences are discussed.
Perspective
It is estimated that every sixth patient who had an ischaemic stroke otherwise qualifying for intravenous thrombolysis (IVT) has a prescription for direct oral anticoagulants (DOACs).1 Currently, US and European guidelines recommend against the use of IVT in patients with ingestion of a DOAC within the last 48 hours unless certain laboratory tests are normal and regardless of the DOAC dose,2 3 but a large heterogeneity of recommendations exists among other regions.4 Determining DOAC plasma levels in emergency situations is challenging and time-consuming in most settings. Furthermore, DOAC plasma level cut-offs below which thrombolysis is deemed safe vary considerably among institutions. Consequently, the vast majority of patients with acute ischaemic stroke and no further contraindications despite oral anticoagulation are excluded from acute medical reperfusion therapy.
Recently, a US stroke registry found no increased risk of symptomatic intracranial haemorrhage (sICH) among patients who had taken DOACs within the preceding 7 days, compared with patients who took no anticoagulants (unadjusted sICH risk 3.7% vs 3.2%; adjusted OR 0.88, 95% CI 0.7 to 1.1).5 There were limitations in the analysis, such as not knowing the precise timing of the last DOAC dose for most patients, with only a very small group of patients who had confirmed ingestion within 48 hours before experiencing a stroke. Additionally, information on selection strategies including plasma level measurements for these patients was not provided. More recently, a global multicentre retrospective cohort study determined the risk of sICH associated with use of IVT for acute ischaemic stroke in patients with confirmed DOAC ingestion within 48 hours before admission.6 In a comparison of 832 DOAC patients and 32 375 non-DOAC controls, all treated with IVT, there was no signal for harm in terms of sICH (unadjusted sICH risk 2.5% in the DOAC group vs 4.1% in IVT controls; adjusted OR 0.57, 95% CI 0.36 to 0.92). There was also no difference between factor Xa inhibitor (59%, 489 of 832) or factor IIa inhibitor-treated patients (41%, 342 of 832) regarding the risk of sICH. Importantly, the study included 355 patients who received IVT without reversal treatment or DOAC concentration measurement prior to IVT, with no safety concerns either. Functional outcome did not differ between IVT-treated patients with recent DOAC ingestion and controls, suggesting no otherwise increased risk of harm.6 Data from the Safe Implementation of Treatments in Stroke registry (SITS) now show similar safety data.7 In a propensity score-matched analysis, bleeding rates and outcome were compared in N=739 patients with DOACs with 738 with no oral anticoagulant prior to IVT. Baseline differences remained after propensity score matching with a larger onset to needle time in the DOAC group, less concomitant antiplatelet treatment but more endovascular treatments. sICH according to the European Cooperative Acute Stroke Study II criteria was 3.6% vs 4.5%, a non-significant difference.7 As in the previous studies, no differences in functional outcome at 3 months were observed. As a limitation of the SITS analysis, only 245 patients had a confirmed last intake within 24 hours before IVT, and in most of the other patients, the time point seems unclear and DOAC plasma concentrations are not available. A recent trial comparing intravenous argatroban (an direct thrombin inhibitor) in addition to IVT versus IVT alone reported no increased sICH risk or risk of a parenchymal haematoma type 2 (2.3% vs 2.5%), providing additional safety data.8
Are these data now sufficient to modify guideline recommendations? Despite the inherent limitations of observational data from non-randomised studies, we do now have data of similar quality as historically accepted by the stroke community to allow IVT in patients with preceding warfarin therapy (international normalised ratio (INR) ≤1.7) or dual antiplatelet therapy.3 The number of patients with effective anticoagulation in the DOAC studies is even larger than in the low-INR warfarin studies. Given the established benefits of IVT, and no signs of harm, neither in the observational data nor experimentally, the evidence towards a more liberal approach is better than the evidence to withhold the only established medical reperfusion treatment for acute ischaemic stroke in DOAC-treated patients.
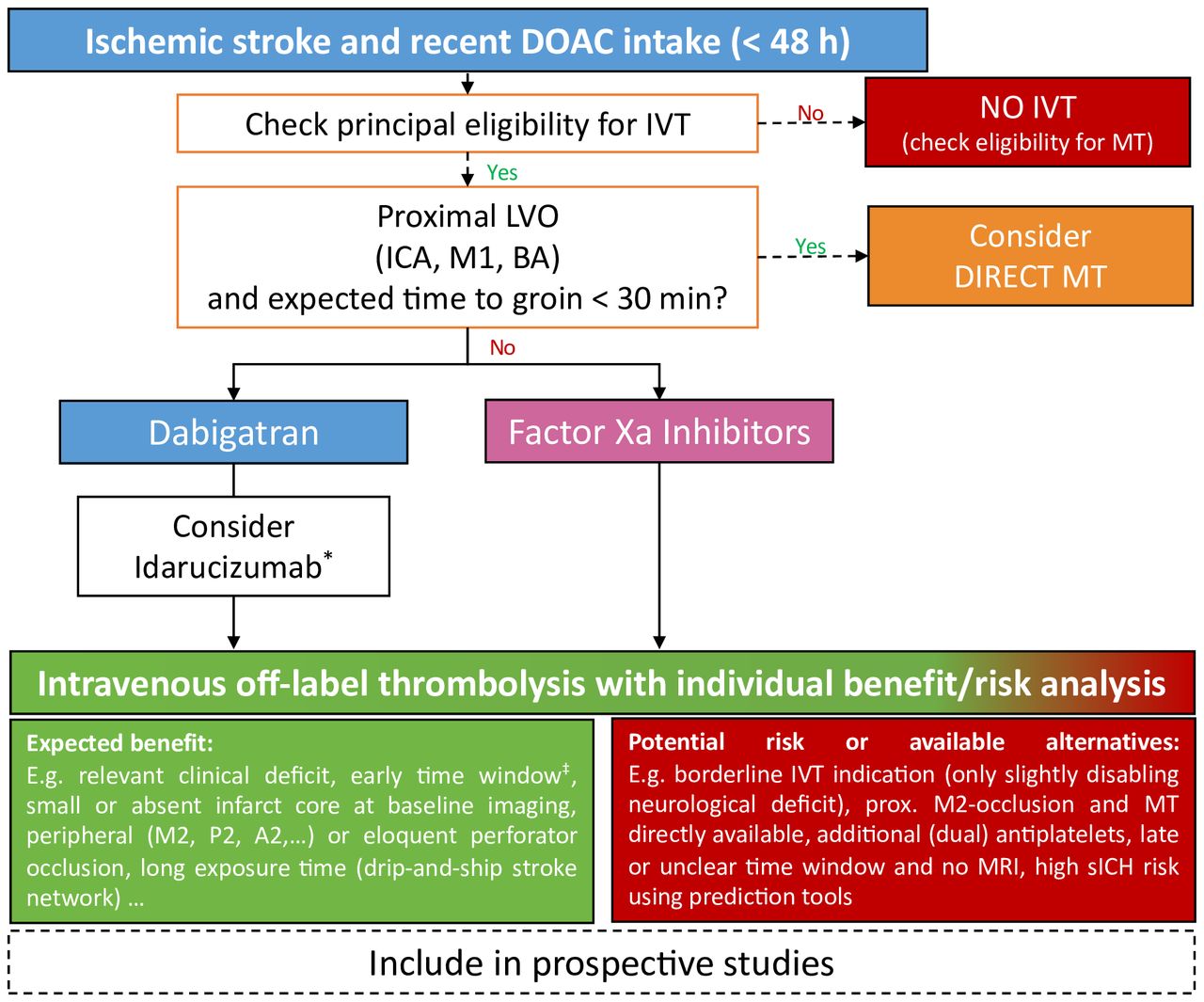
Figure 1 shows an approach to IVT despite DOAC pretreatment based on the discussed evidence. An individual risk/benefit assessment should be made, including established bleeding predictors as well as availability of alternative treatment options (eg, direct mechanical thrombectomy). This risk/benefit analysis should also encompass the time window, as the majority of patients in Meinel et al were treated in early time windows (median time from onset to IVT 2.5 hours, IQR 1.8–3.5),6 and only few patients were treated using multimodal imaging to guide decision-making. Regarding dabigatran, prospective studies need to address the question, whether IVT after reversal using idarucizumab is safer and of similar efficacy compared with IVT without reversal, as suggested by previous observational data.9 Other than idarucizumab, andexanet alfa for reversal of factor Xa inhibitors is not licensed for emergency interventions, and there is evidence of an increased risk of thromboembolic events in patients with ICH receiving andexanet alfa. Due to this, as well as logistical obstacles and high cost, it is currently not recommended before IVT on an expert consensus level. The safety data are mainly based on outcomes of individually selected patients treated at experienced stroke centres. Prospective follow-up of any modified approach is therefore recommended to both identify any not-yet detected safety signals, as well as to establish more information regarding a potential additional beneficial effect of DOAC pretreatment on the efficacy and safety of IVT.

Algorithm for intravenous off-label thrombolysis in patients with acute ischaemic stroke on treatment with direct oral anticoagulants (DOACs). *Optional: administration of idarucizumab (two times 2.5 g intravenously before IVT) if available immediately. ‡Restrict IVT to patients in early time window (rationale: median time to IVT was 2.5 hours (1.8–3.5) in Meinel et al; MRI might help to determine patients eligible for IVT in wake-up stroke or unknown time windows (DWI/FLAIR mismatch)). Factor Xa inhibitors=apixaban, edoxaban, rivaroxaban. A2, segment of the anterior cerebral artery; BA, basilar artery; DWI, diffusion-weighted imaging; FLAIR, fluid-attenuated inversion recovery; ICA, internal carotid artery; IVT, intravenous thrombolysis; LVO, large vessel occlusion; M1, M2, segments of the middle cerebral artery; MT, mechanical thrombectomy; P2, segment of the posterior cerebral artery; sICH, symptomatic intracranial haemorrhage.
Importantly, current data apply to IVT using recombinant tissue plasminogen activator, as data on tenecteplase in DOAC-receiving patients are scarce (in Meinel et al,6 tenecteplase was used in n=51 patients with recent DOAC intake, the majority of them on dabigatran, with idarucizumab reversal before IVT). However, given the generally similar safety profile of tenecteplase 0.25 mg/kg compared with alteplase 0.9 mg/kg,10 11 IVT with tenecteplase seems justified in individually selected patients in the early time windows, relevant clinical deficit and eloquent peripheral or perforator occlusions not accessible by endovascular therapy. It is now time to tear down the yet crackly wall in front of reperfusion treatment for those who experience stroke despite oral anticoagulation with DOACs.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors Original draft made by JCP. All authors contributed to conceptualisation, review and editing and visualisation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JCP has received consultation fees and travel expenses from Akcea, Bayer, Boehringer Ingelheim, Daiichi Sankyo and BMS/Pfizer, outside the submitted work. TRM reports grants from Bangerter-Rhyner Foundation. YX has received a research grant from the National Institute on Aging, American Heart Association and Genentech, and honorarium from Boehringer Ingelheim. DJS is on the advisory board of Bayer Switzerland and Portola/Alexion. He reports research funding from the Swiss National Science Foundation, Swiss Heart Foundation, Bangerter-Rhyner Foundation, Bayer Foundation and Portola/Alexion. All other authors report no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.





{kind=link}