

Article Figures & Data
- Figure 1
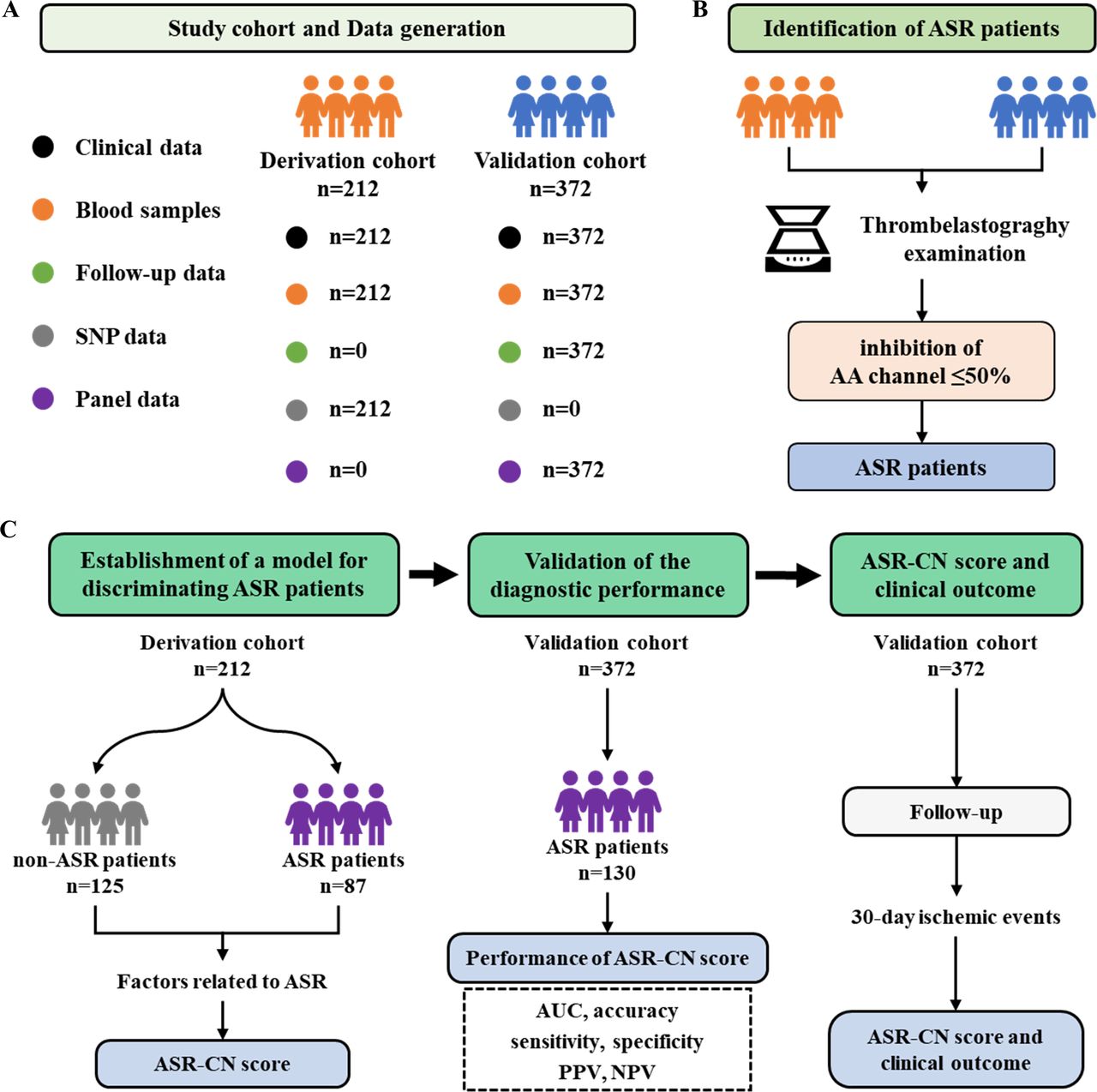
Data generation and study design. (A) The summary of data generation. (B) The flowchart of identifying ASR patients. (C) The flowchart of study design. We included 212 ICH patients in the Surgical Treatments of Antiplatelet Intracerebral Hemorrhage cohort who discontinued aspirin <5 days in the derivation cohort. In total, 87 patients of them were identified as ASR. In addition, we recruited 372 patients with UIA undergoing interventional procedures as a validation cohort. Among them, 130 patients were identified as ASR. Within the derivation cohort, we investigated the SNPs related to ASR, and constructed a scoring system (aspirin resistance in Chinese population score (ASR-CN score)) to identify ASR patients. Within the validation cohort, we validated the accuracy of the ASR-CN score in identifying ASR patients and whether the ASR-CN score is related to clinical outcomes (30-day ischaemic events after UIA embolisation). AA, arachidonic acid channel in the thromboelastography; ASR, aspirin resistance; ICH, intracerebral haemorrhage; NPV, negative predictive value; PPV, positive predictive value; SNP, single-nucleotide polymorphism; UIA, unruptured intracranial aneurysm.
- Figure 2
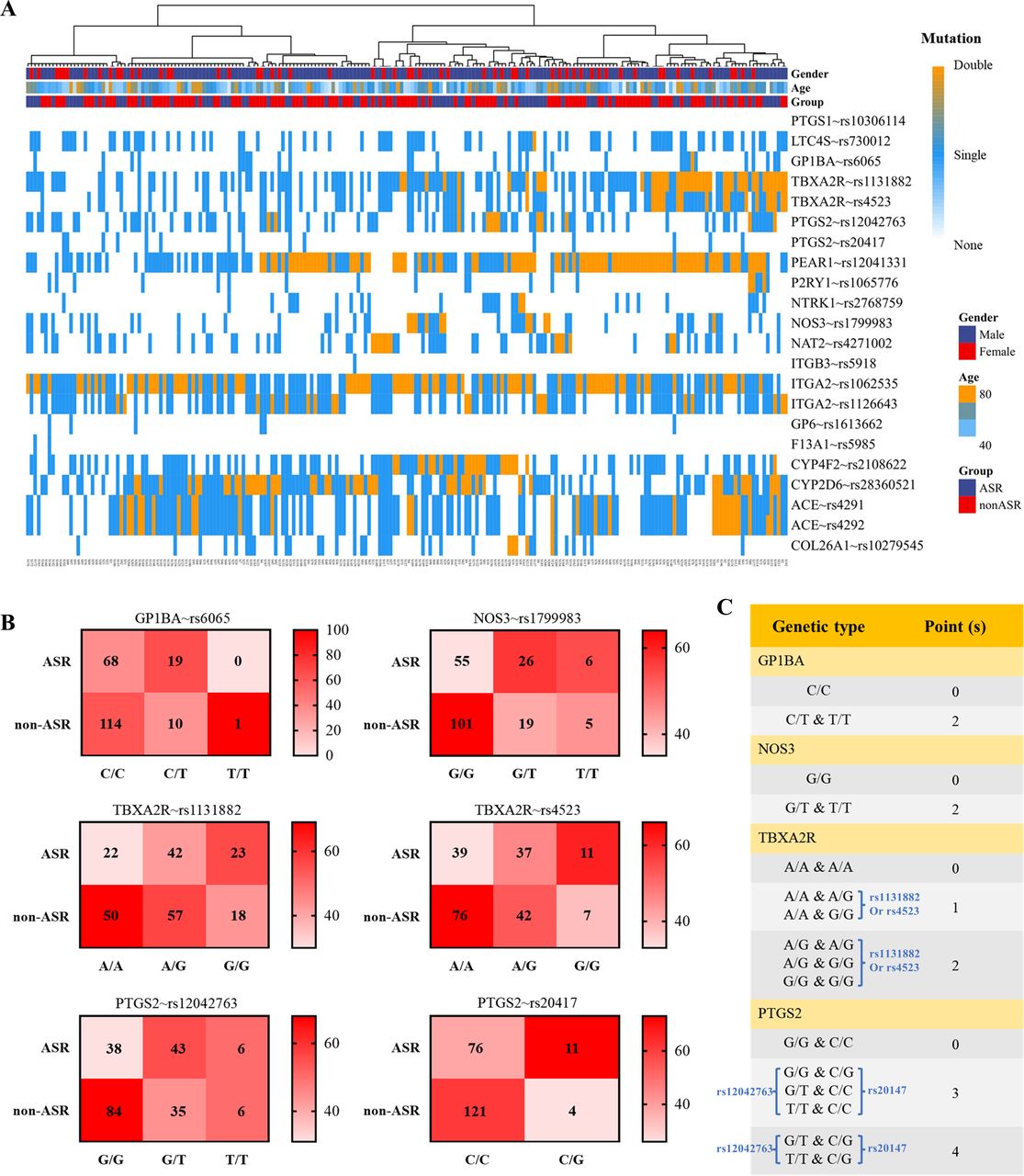
The genetic mutation associated with ASR and the aspirin resistance in the Chinese population score (ASR-CN) scores (A) The heatmap presents the mutations of single-nucleotide polymorphism related to aspirin’s metabolism and efficacy, based on the derivation cohort. (B) The confusion matrixes show the number and percentage of ASR in each genetic type for GP1BA, NOS3, TBXA2R and PTGS2, within the derivation cohort. (C) The ASR-CN score was used to identify patients at high risk of ASR. ASR, aspirin resistance.
- Figure 3
Validation of the performance of the ASR-CN scores to identify ASR patients. (A) Within the validation cohort, ASR patients had higher ASR-CN scores compared with non-ASR patients. (B) The performance of ASR-CN score and other parameters to discriminate ASR patients from non-ASR patients. (C) The forest plot displayed the result of the univariate logistic analysis for ASR within the validation cohort. The mutations in GP1BA, NOS3, TBXA2R and PTGS2 were related to ASR. High ASR-CN was a risk factor for ASR. AUC, area under the curve; APTT, activated partial thromboplastin time; ASR, aspirin resistance; ASR-CN; aspirin resistance in the Chinese population; CA, coronary artery; PT, prothrombin time.
- Figure 4
A high ASR-CN score is associated with a high risk of ischaemic events in patients receiving intracranial aneurysm embolisation. (A) More ASR patients (with a arachidonic acid channel in the thromboelastography<50%) experienced ischaemic events within 30 days after aneurysm embolisation compared with the non-ASR patients. (B) The confusion matrix presents the percentage of patients suffering from 30-day ischaemic events in each CYP2C19 metaboliser. Patients with PM metaboliser had the highest percentage of 30-day ischaemic events. (C) The distribution of patients with 30-day ischaemic events in each ASR-CN score. (D) The forest plot shows the results of the univariate logistic analysis for 30-day ischaemic events. ASR, aspirin resistance; ASR-CN, aspirin resistance in the Chinese population; CA, coronary artery; EM, extensive metaboliser; IM, intermediate metaboliser; PM, poor metaboliser.




- Table 1
The demographic and clinical features of patients in the derivation cohort
Characteristics ASR n=87 Non-ASR n=125 P value Age, years, m (IQR) 56 (48–66) 61 (51–71) 0.902 Male gender, n (%) 64 (73.6%) 91 (72.8%) 0.117 Comorbidities, n (%) Dyslipidaemia 7 (8.0%) 13 (10.4%) 0.565 Diabetes mellitus 25 (28.7%) 36 (28.8%) 0.992 CA diseases 67 (77.0%) 107 (85.6%) 0.110 Ischaemic stroke or TIA 22 (25.3%) 43 (34.4%) 0.158 Ever-or-now smokers, n (%) 29 (33.3%) 25 (20.0%) 0.029* Regular drinkers, n (%) 3 (3.4%) 4 (3.2%) 0.921 Laboratory findings Platelet count, ×109, m (IQR) 216 (192–238) 216 (200–226) 0.790 APTT, m (IQR) 24.8 (24.5–31.7) 24.8 (24.4–30.4) 0.323 PT, m (IQR) 1.01 (1.00–1.07) 1.00 (0.96–1.04) 0.059 Fibrinogen, g/L, m (IQR) 2.8 (2.3–3.1) 2.8 (2.4–3.6) 0.100 Antiplatelet therapy, n (%) 0.218 Aspirin 71 (81.6%) 93 (74.4%) Dual antiplatelet 16 (18.4%) 32 (25.6%) Haematoma location, n (%) 0.838 Supratentorial lobar 23 (26.4%) 43 (34.4%) Supratentorial deep 57 (65.5%) 62 (49.6%) Cerebella 7 (8.0%) 20 (16.0%) Haematoma volume, mL, m (IQR) 51.8 (33.3–75.3) 49.7 (36.2–82.2) 0.477 *The difference was significant.
APTT, activated partial thromboplastin time; ASR, aspirin resistance; CA, coronary artery; PT, prothrombin time; TIA, transient ischaemic attack.
- Table 2
Multivariate logistic analysis of factors related to aspirin resistance based on the derivation cohort
Parameters Crude Adjusted* OR (95% CI) P value OR (95% CI) P value Ever-or-now smokers 1.73 (0.86 to 3.46) 0.124 GP1BA (C/C vs C/T and T/T) 2.54 (1.06 to 6.09) 0.037 2.77 (1.13 to 6.78) 0.025 TBXA2R A/A and A/A Reference Reference A/A and A/G, A/A and G/G 1.41 (0.59 to 3.38) 0.442 1.39 (0.57 to 3.35) 0.468 A/G and A/G, A/G and G/G, G/G and G/G 2.44 (1.18 to 5.06) 0.016 2.31 (1.10 to 4.84) 0.026 PTGS2 G/G and C/C Reference Reference G/G and C/G, G/T and C/C, T/T and C/C 3.12 (1.67 to 5.84) <0.001 3.2 (1.69 to 6.10) <0.001 G/T and C/G, T/T and C/G 13.07 (1.32 to 128.97) 0.028 13.50 (1.33 to 136.83) 0.028 NOS3 (G/G vs G/T and T/T) 2.16 (1.06 to 4.39) 0.033 2.33 (1.13 to 4.82) 0.023 *The result was adjusted by age, gender, dyslipidaemia, diabetes mellitus, regular drinkers and platelet count.
- Table 3
The difference of patients in the validation cohort, grouped by 30-day ischaemic events
Characteristics Ischaemic events n=45 No ischaemic events n=327 P value Age, years, m (IQR) 57 (47–62) 55 (49–62) 0.443 Male gender, n (%) 19 (42.2%) 158 (48.3%) 0.868 Comorbidities, n (%) Hypertension 18 (40.0%) 124 (37.9%) 0.788 Dyslipidaemia 6 (13.3%) 29 (8.9%) 0.337 Diabetes mellitus 14 (31.1%) 91 (27.8%) 0.647 CA diseases 6 (13.3%) 25 (7.6%) 0.196 Ischaemic stroke or TIA 30 (66.7%) 165 (50.5%) 0.042* Ever-or-now smokers, n (%) 18 (40.0%) 115 (35.2%) 0.527 Regular drinkers, n (%) 2 (4.4%) 32 (9.8%) 0.244 Laboratory findings Platelet count, ×109, m (IQR) 216 (210–244) 216 (206–229) 0.215 APTT, m (IQR) 24.8 (23.2–30.4) 24.8 (24.5–30.4) 0.506 PT, m (IQR) 1 (1–1) 1 (1–1) 0.058 Fibrinogen, g/L, m (IQR) 2.80 (2.42–3.58) 2.80 (2.34–3.33) 0.498 Aneurysm locations, n (%) 0.198 AcomA/ACA 5 (11.1%) 27 (8.3%) ICA 30 (66.7%) 201 (61.5%) MCA 10 (22.2%) 87 (26.6%) PC 0 (0.0%) 12 (3.7%) Aneurysm size, mL, m (IQR) 6.4 (6.1–8.8) 6.3 (6.0–8.7) 0.499 ASR (TEG-AA<50%), n (%) 22 (48.9%) 108 (33.0%) 0.037* ASR-CN score, m (IQR) 4 (2–5) 3 (2–4) 0.036* CYP2C19 metaboliser, n (%) <0.001* EM 4 (8.9%) 134 (41.0%) IM 30 (66.7%) 162 (49.5%) PM 11 (24.4%) 31 (9.5%) *The difference was significant.
ACA, anterior cerebral artery; AcomA, anterior communicating artery; APTT, activated partial thromboplastin time; ASR, aspirin resistance; ASR-CN, aspirin resistance in the Chinese population; CA, coronary artery; EM, extensive metaboliser; ICA, internal carotid artery; IM, intermediate metaboliser; MCA, middle cerebral artery; PC, posterior circulation; PM, poor metaboliser; PT, Prothrombin time; TEG-AA, arachidonic acid channel in the thromboelastography; TIA, transient ischaemic attack.
- Table 4
Multivariate logistic analysis of factors related to 30-day ischaemic events based on the validation cohort
Parameters Crude Adjusted* OR (95% CI) P value OR (95% CI) P value Ischaemic stroke 2.08 (1.04 to 4.16) 0.038 2.08 (1.03 to 4.22) 0.041 ASR-CN score 1.28 (1.10 to 1.50) 0.002 1.28 (1.09 to 1.50) 0.002 CYP2C19 metaboliser EM Reference Reference IM 6.61 (2.24 to 19.48) 0.001 6.52 (2.20 to 19.29) 0.001 PM 17.83 (5.04 to 63.10) <0.001 19.50 (5.44 to 69.89) <0.001 *The result was adjusted by age, gender and aneurysm size.
ASR-CN, aspirin resistance in the Chinese population; EM, extensive metaboliser; IM, intermediate metaboliser; PM, poor metaboliser.
Supplementary Materials
Supplementary data
Additional Files
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.




{kind=link}
{kind=link}
{kind=link}
{kind=link}