

Abstract
Objective Pial arteriovenous fistulas (PAVFs) are rare and mostly observed in children. However, the overall angioarchitecture, clinical features, treatments and long-term prognosis for pediatric patients remain unclear.
Methods Clinical data of consecutive 42 pediatric PAVFs were documented and analysed. According to the differences of age distribution and clinical features, they were split into a younger group (≤3 years old; 20 cases) and an older group (3–14 years old; 22 cases).
Results Their mean age was 4.9±3.9 years, and the mean preoperative modified Rankin Scale (mRS) score was 1.64±1.57. Fourteen patients (33.3%) were asymptomatic, followed by epilepsy (21.4%), intracranial haemorrhage (16.7%), hydrocephalus (9.5%), developmental delay (7.1%), intermittent headache (7.1%) and congestive heart failure (4.8%). Annual bleeding rate and rebleeding rate before treatment reached 3.86% and 3.17%. Poor venous drainage including sinus dynamic obstruction (21 cases, 50.0%) and sinus occlusion (17 cases, 40.48%) were found with high frequency among these patients. Finally, 33 cases were cured (78.57%), and 4 cases faced surgery-related complications (9.52%). During 24–140 months’ follow-up, the mean mRS score reduced to 0.57±0.40. However, only 22 cases (52.38%) recovered to absolutely normal, and poor venous drainage was the risk factor for patients’ incomplete recovery (p=0.028, Exp(B)=14.692, 95% CI 1.346 to 160.392). Compared with the older group, younger group showed more chronic symptoms, more secondary pathological changes, more times treatment and worse prognosis (p=0.013, 0.002, 0.000 and 0.032, respectively).
Conclusions Pediatric PAVF has different angioarchitectures, clinical features and prognoses in different age groups. Poor venous drainage is an important factor leading to poor prognosis, and it accounts for incomplete recovery in nearly half of patients.
Introduction
Pial arteriovenous fistula (PAVF) is a rare intracranial vascular disease defined as a direct pathological connection between one or more arterial supplies and venous drainage without an intervening nidus. According to previous reports, PAVF accounts for 1.6%–7.3% of all intracranial vascular malformations and seems more common in pediatric patients.1–5 There is no intervening tangles of vessels between the feeding artery and draining vein, which makes the lesion more vulnerable to rupture or causes secondary symptoms, such as subependymal or cortical atrophy, white matter calcification, occlusive venography and hydrocephalus, which may lead to poor prognosis for pediatric patients in particular.6–8
In recent years, with the innovation of interventional materials and techniques, endovascular treatment has achieved relatively high occlusion rates and becoming the preferred treatment for PAVFs.9–11 However, the long-term prognosis of patients after treatment is unclear. And, the effect of lesions’ angioarchitecture on clinical symptoms, treatment and prognosis has been less frequently studied in previous studies. Additionally, although surgeons perceive some differences in pediatric patients of different ages, there has not yet been enough clinical data to prove and reveal these differences.
Patients and methods
Patients
A retrospective review of our prospectively maintained database was performed on pediatric patients diagnosed with a cerebral arteriovenous malformation (CAVM) from January 2010 to December 2019. Based on MRI and selective cerebral digital subtraction angiography (DSA), more than three experienced cerebral vascular specialists were employed to make the diagnosis. PAVFs are defined as lesions comprising single or multiple arterial feeders draining directly into the venous channel without intervening tangle of blood vessels as in CAVMs. Vein of Galen malformations, arteriovenous fistula inside arteriovenous malformations (AVMs), and traumatic or iatrogenic arteriovenous fistula were excluded. Patients’ basic information, clinical features, angioarchitecture, treatment details and follow-up results were collected. The age distribution was concentrated in two peaks (2 years old and 7 years old), with 3 years old being the watershed of the age distribution. Considering the differences in children’s developmental characteristics and their clinical characteristics, these pediatric patients were divided into a younger group (≤3 years, 20 cases) and an older group (>3 years, ≤14 years, 22 cases).
Treatment and results
In our centre, microsurgical disconnection, endovascular embolisation and hybrid operation can be skillfully performed for every patient. Considering the particular context of pediatric PAVFs (such as the trauma of open surgery, the effect of surgery on blood circulation and the risk of postoperative complications), endovascular embolisation was preferred as the primary treatment for most cases. According to the angioarchitecture of the lesion and the experience of the surgeon, four embolisation strategies were chosen to occlude the high-flow fistula: (1) coil embolisation; (2) Glubran embolisation; (3) coil combined with Glubran or Onyx embolisation and (4) balloon microcatheter-assisted Glubran embolisation.
Clinical results were assessed by the modified Rankin Scale (mRS). Follow-up results were recorded via the inpatient (29 cases), outpatient (8 cases) or telephone (5 cases). The radiographic outcome was evaluated by DSA (33 cases) or MR angiography (9 cases). Images at more than 24 months’ follow-up were used to confirm the complete obliteration of lesions. Subtotal occlusion was defined as more than 90% of the lesions disappeared but not completely occluded. Partial occlusion was defined as less than 90% resolution of the lesion after treatment.
Statistical analysis
SPSS for Windows (V.20.0; IB) was used for statistical analysis. Variables are expressed as the mean±SD, the median (P25, P75) or the number of patients (percentage). Intracranial dural sinus occlusion and cerebral ventricle dilation were further illustrated using the Kaplan-Meier method, and the curves were compared by the log-rank test. Pearson’s χ2 test or Fisher’s exact test was used for categorical variables, Student’s t-test and the rank sum test were used for continuous variables to evaluate differences in clinical variables and outcomes. Logistic regression analysis was used to evaluate the impact of multiple factors on incomplete recovery and detect prognostic risk factors. Statistical significance was assigned for p<0.05.
Results
Patient population
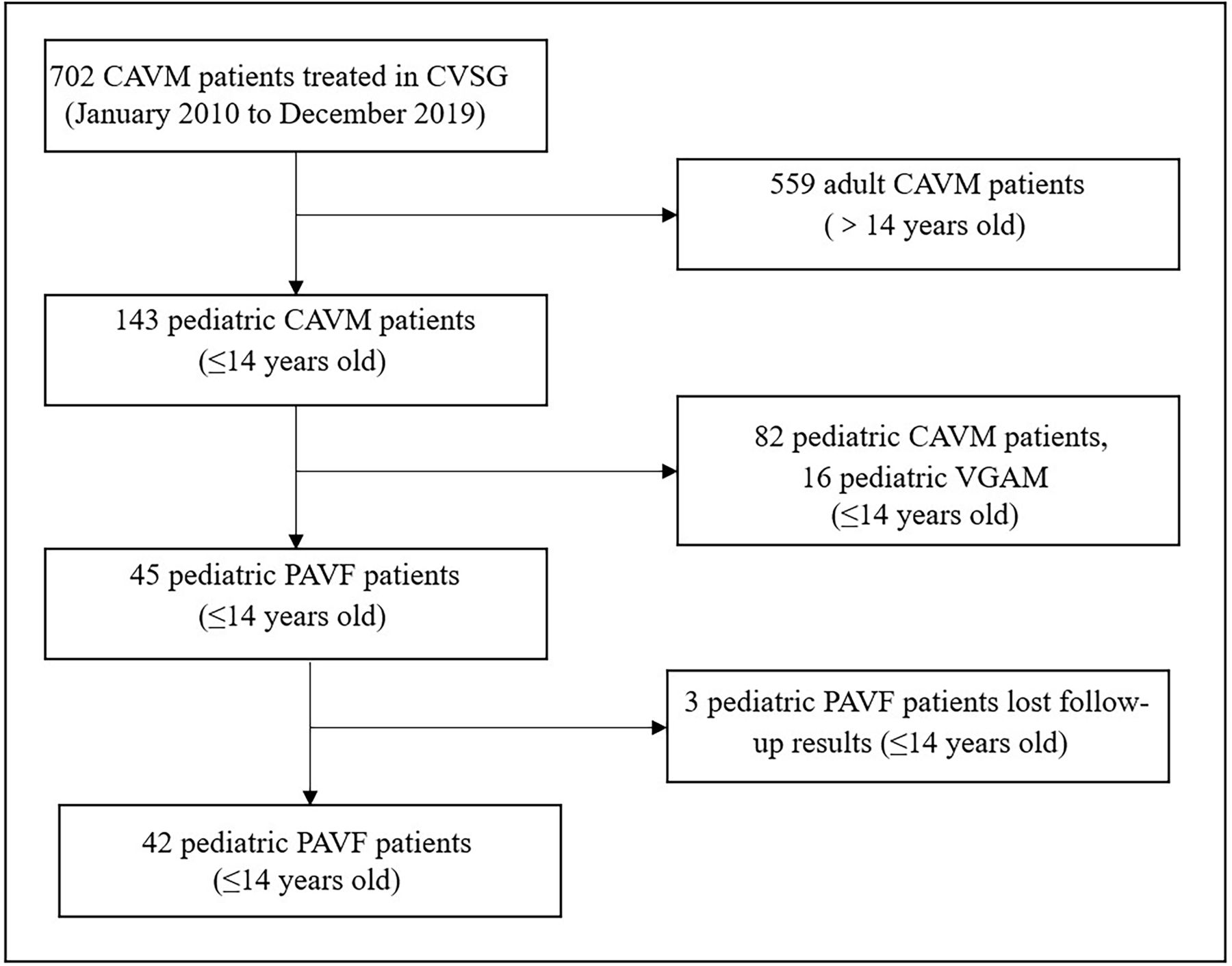
From January 2010 to December 2019, 702 patients with CAVM were treated in our Cerebral Vascular Study Group, of whom 143 were pediatric patients (≤14 years old, 20.4%). Through a retrospective review, 45 consecutive pediatric patients with PAVF were found (6.41% in all patient groups, 31.47% in the pediatric group). Excluding three cases lost to follow-up, a total of 42 cases were included (figure 1). Finally, 20 cases and 22 cases were enrolled into the younger group and the older group, respectively (tables 1 and 2).

Flow chart showing the selection process for the overall study cohort. CAVM, cerebral arteriovenous malformation; CVSG, Cerebral Vascular Study Group; PAVF, pial arteriovenous fistula; VGAM, vein of Galen aneurysmal malformation.
Population and angioarchitecture features of pediatric pial arteriovenous fistula (PAVF)
Treatment and results of pediatric PAVFs
The mean age at presentation was 4.9±3.9 years (varying from 4 months to 14 years). The mean period from onset to treatment was 14.8±10.1 months (varying from 1 day to 7 years), and that of the younger group was shorter (t=3.43, p=0.003) (table 1).
Fourteen patients (33.3%) were found in post-traumatic examinations without PAVF related symptoms, and other patients suffered from epilepsy in 9 cases (21.4%), cerebral haemorrhage in 7 cases (16.7%), hydrocephalus in 4 cases (9.5%), developmental delay in 3 cases (7.1%), intermittent headache in 3 cases (7.1%) and congestive heart failure in 2 cases (4.8%). Among them, one case was discovered in antenatal examination at 32 weeks of pregnancy, and atrial septal defect and hypospadias were found after birth. Compared with the older group, the younger group seemed to suffer more from chronic symptoms (χ2=6.11, p=0.013) (table 1). The annual bleeding rate before treatment reached 3.86%. Recurrent haemorrhage before treatment was seen in one patient, and the annual bleeding rate was 3.17%. No difference in haemorrhage events was found between the two groups (χ2=0.48, p=0.490). The mean preoperative mRS score was 1.64±1.57, and that of the older group was lower (t=2.84, p=0.045).
Angioarchitecture and associated symptoms
Locations and angioarchitectures of these lesions were confirmed by MRI and angiography in all patients. Finally, single lesion of PAVF was identified in 31 cases (73.8%), others had combined lesions or multiple lesions (26.2%). Regarding the PAVFs, 21 cases were on the left side, 20 cases were on the right side and 1 case was bilateral. 85.7% of the lesions located in the supratentorial region, including the temporal lobe in 10 cases (23.8%), occipital lobe in 9 cases (21.4%), quadrigeminal region in 7 cases (16.7%), frontal lobe in 6 cases (14.3%), parietal lobe in 1 case, frontal lobe and quadrigeminal region in 1 case (2.4%) and temporal lobe and occipital lobe in 1 case (2.4%).
All of the AVFs were macroshunt with high blood flow. Arteries of anterior circulation, posterior circulation arteries and both circulation arteries were involved in 64.3%, 61.9% and 26.2% of these patients, respectively. Additionally, branches of posterior cerebral arteries were the most common feeding artery (20/42, 47.6%), followed by middle cerebral arteries (16/42, 38.1%) and anterior cerebral arteries (12/42, 28.6%).
Venous varix at the beginning of the drainage vein was identified in 41 cases (97.6%). Thirty-seven cases with only 1 drainage outlet, including the superior sagittal sinus (SSS,13 cases), sigmoid sinus (SigS, cases), straight sinus (StrS, 7 cases), torcular herophili (TorH, 4 cases), transverse sinus (TraS,4 cases), falcine sinus (FalS, 1 case) and perimedullary vein (PerV, 1 case). Two drainage outlets were seen in five cases (11.9%), including two cases in SSS and SigS, three cases in SSS+StrS and one case in SSS+FalS. One or more sinus occlusions were seen in 17 cases (40.5%), and sinus stenosis (moderate to severe) was seen in 9 cases (21.4%). Dynamic angiography imaging showed that 50.0% of the patients had accompanying dynamic sinus obstruction (cerebral venous drainage was obviously blocked and the circulation time of cerebral blood flow was prolonged). Sinus occlusion and dynamic obstruction were more common in the younger group (p=0.014 and p=0.013, respectively).
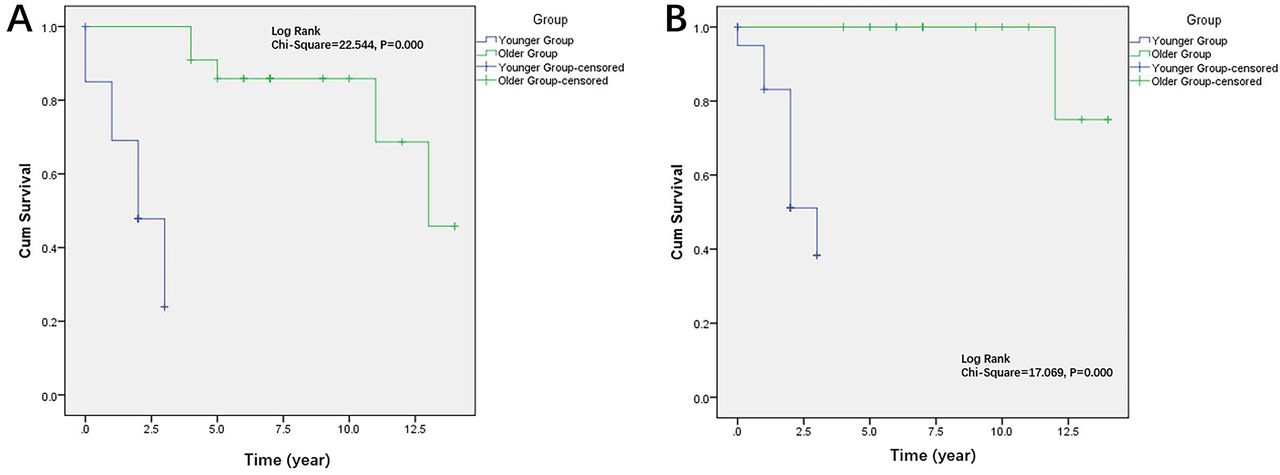
Cerebral ventricle dilation was noted in 13 cases, of which there were 3 patients presented with hydrocephalus and 2 patients presented with developmental delay. Statistical analysis showed that dynamic sinus obstruction was correlated with ventricular dilation (χ2=4.725, p=0.030). Cardiac enlargement was noted in 21 cases; among them, only 2 patients presented with symptoms associated with congestive heart failure. Cardiac enlargement was more common in young children (χ2=9.545, p=0.002) and patients with dural sinus occlusion (χ2=4.842, p=0.028) (figure 2).

Kaplan-Meier curves demonstrating the risk of intracranial dural sinus occlusion and cerebral ventricle dilation. Kaplan-Meier curves (log-rank test) illustrating intracranial dural sinus occlusion risks (A) and cerebral ventricle dilation risks (B) of pediatric pial arteriovenous fistula in younger children (≤3 years) were higher than in older children (>3 years, ≤14 years).
Treatment and results
Endovascular embolisation was preferred as the primary treatment for PAVF in all these cases, including Glubran embolisation in 17 cases, coil combined with Glubran or Onyx embolisation in 16 cases, balloon microcatheter-assisted Glubran embolisation in 6 cases and coil embolisation in 3 cases (figures 3,4). The cure rates of each method were 64.7% (11/17), 87.5% (14/16), 83.3% (5/6) and 100.0% (3/3), respectively. At the time of follow-up, a total of 33 cases were cured (78.6%). Compared with the older group, the younger group seemed to need more times embolisation (t=12.365, p=0.000) (table 2).

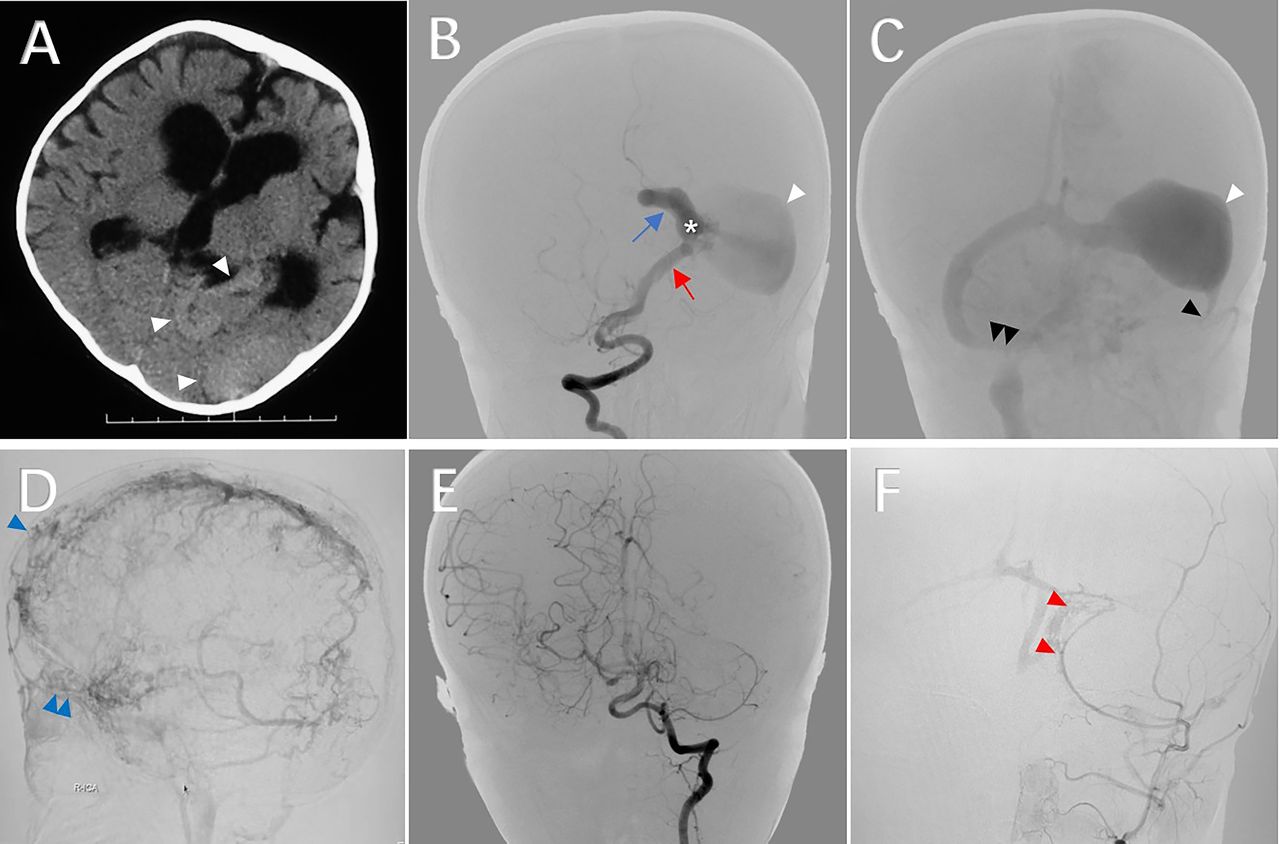
Pial arteriovenous fistula (PAVF) in younger child. An 8-month-old girl suffered from paroxysmal absence seizure since birth, accompanied with motor and language delayed development for 6 months. On admission, physical examination showed head circumference enlarged significantly and scalp veins dilated obviously (mRS=1). A subtentorial PAVF fed by left posterior cerebral artery (PCA) was diagnosed, and balloon-assisted Glubran embolisation was performed successfully. However, multiple de novo DAVFs were found 2 years later, and the patient‘s symptoms were only partially relieved (mRS=1). (A) Axial brain CT scan imaging, shows hydrocephalus, melting brain signs and high-density shadows in left occipital lobe (white arrowhead); (B, C) Posteroanterior view of right vertebral artery (VA) angiogram (B), early arterial phase; (C) venous sinus phase), shows the PAVF with venous varix (star) was feed by the calcarine branch of PCA (red arrow) and drained via the superior hemispheric vein (blue arrow) to the extremely dilated transverse sinus (white arrow). The left sigmoid sinus was occluded (black arrowhead) and the terminal of right sigmoid was severely stenosed (double black arrowhead); (D) Lateral view of right internal carotid artery (ICA) angiogram (venous sinus phase), shows the dynamic sinus obstruction made the cortical vein tortuous and dilated obviously, the transverse sinus and sigmoid sinus were not developed, the intracranial venous drainage were frontal scalp veins (blue arrowhead) and periocular venous plexus (double blue arrowhead); (E) Posteroanterior view of left VA angiogram 2 years post embolisation, shows the fistula was completely obliterated; (F) Posteroanterior view of left external carotid artery angiogram 2 years post embolisation, shows DAVFs located in the left occipital sinus (red arrowhead), the right sigmoid sinus and left transverse sinus were occluded. DAVFs, dural arteriovenous fistula; mRS, modified Rankin Scale.

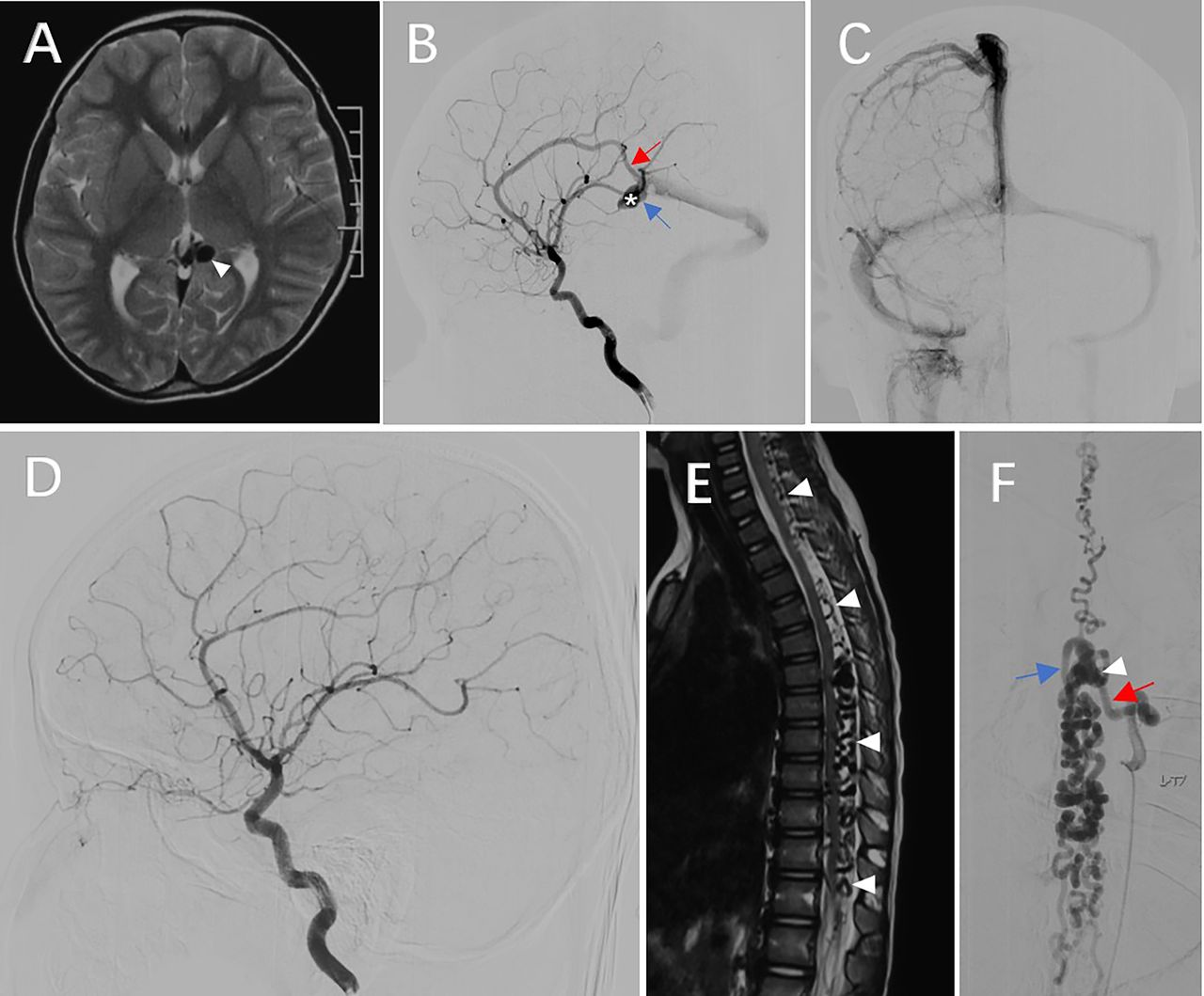
Pial arteriovenous fistula (PAVF) in older child. A 7-year-old boy suffered from back pain for 1 month, MRI and DSA show a PAVF in quadrigeminal region and a perimedullary arteriovenous fistula (PMAVF) in the seventh thoracic vertebra level. On admission, physical examination was normal (mRS=0). Then, both of the lesion received the embolisation with Glubran successfully, which were confirmed to have been cured in the 3 years follow-up DSA. (A) Axial T2-weighted MRI, show flow-voids (white arrowhead) in the left quadrigeminal region; (B) Lateral view of left ICA angiogram (arterial phase), shows the PAVF with a venous varix (star) was feed by the pericallosal artery (red arrow) and drained via the vein of Rosenthal (blue arrow); (C) Posteroanterior view of left ICA angiogram (venous sinus phase), shows no occlusion or stenosis in dural sinus; (D) Lateral view of left ICA angiogram 3 years postembolisation, show the fistula was completely obliterated; (E) Sagittal T2-weighted MRI, shows flow-voids (white arrowhead) around the spinal cord, extending from cervical to lumbar level; (F) Posteroanterior view of left T7 intercostal artery preoperative angiogram, shows the fistula (white arrowhead) feeding by L-T7 radiculomedullary (red arrow) and draining by perimedullary veins (blue arrow) was occluded successfully. DSA, digital subtraction angiography; mRS, modified Rankin Scale.
The incidence of procedure-related complications was 9.52% (4/42), including postoperative draining vein thrombosis (2 cases), postoperative haemorrhage (1 case) and postoperative hemianopia of the bilateral visual field (1 case). Patients suffering from draining vein thrombosis presented with headache, nausea and vomiting followed by grand mal seizures and recovered after heparin anticoagulant therapy. The patient suffering from postoperative haemorrhage presented with only slight headache and recovered after conservative treatment. And, the patient suffering from hemianopia of the bilateral visual field, caused by unexpected arterial embolism, almost recovered 1 year later.
The average follow-up time was 71.5±36.6 months (range 24–140 months). The mean mRS score at follow-up was 0.57±0.40, which was improved compared with the preoperative status. Twenty-two patients recovered to normal without any symptoms, which seemed more common in the older group (χ2=4.624, p=0.032) (table 2).
In the follow-up angiography, de novo dural arteriovenous fistulas (DAVFs) with cortical veins involved (classification was Cognard IIb and Borden II) were found in four patients (9.5%) (figure 3). All of them were young children (≤3 years) with intracranial dural sinus occlusion and dynamic sinus obstruction. Additionally, severe sinus stenosis was noted in three of them. Statistical analysis also showed that de novo DAVF was more likely in the younger group (χ2=5.349, p=0.039) and correlated with dural sinus occlusion (χ2=4.751, p=0.029) (table 2).
Logistic regression analysis was used to evaluate the impact of multiple factors on incomplete recovery. We found that poor venous drainage, including dynamic sinus obstruction and sinus occlusion, was the risk factor for patients’ incomplete recovery (p=0.028, Exp(B)=14.692, 95% CI 1.346 to 160.392).
Discussion
Since first described by Walter Dandy in 1928, several cases of pial arteriovenous fistulas have been reported.4 6 8 Since they are rare and disperse, their clinical features, angioarchitecture and long-term outcomes have not been described comprehensively. Although have been reported in patients of all ages, PAVFs still show a greater likelihood of occurring in children. And, some features have different tendencies in children of different ages, however, the details of these differences are still unclear.2 3 6–8
Differences between younger and older pediatric PAVFs and associated aetiological consideration
To the best of our knowledge, this is the largest single-institution retrospective series of PAVFs. In this study, we found that younger patients were more likely to present with chronic symptoms (such as chronic hydrocephalus, developmental delay and congestive heart failure), higher preoperative mRS scores, more sinus occlusion and obstruction, more related changes in the brain and heart, more treatments and worse prognosis. Some factors may be associated with this, such as incomplete cranial suture occlusion that allows compensatory space inside the skull without obvious symptoms, inability to verbally express the symptoms experienced by the younger child. In this study, we divided the patients into a younger group and an older group to obtain clues to discover the causes of these changes. We found that the drainage status as well as the related changes showed visible differences between the two age groups. Based on the literature and our studies, we speculate that the drainage vein and sinus play an important role in the occurrence and development of PAVFs, which is also the main reason for the different clinical manifestations and prognoses.
As Padget proposed in 1956, the venous system of the brain is the earliest vascular system to develop, and it develops from large venous channels to smaller primitive venous channels in the 11–14 mm stage ahead of the arterial system.12 Then, the Wills circle develops, and the pial arteries (mere endothelial tubes) sprout from its branches and cross the pial veins during the 20 mm stage. Generally, the more acute the crossing angle is, the greater the crossing surface area that exists between the pial arteries and veins, and the greater the chance of the development of arteriovenous shunts. Such shunts are common in a transient stage during embryonic development, and they will regress with the development of the capillary network and the maturity of the vessel wall. If the regression process fails and the vessel wall matures, the arteriovenous shunt will persist and form a PAVF or other vascular lesions later.3 12 As showed in our study, cases diagnosed in antenatal examination as well as the cases with drainage via the persistent falcine sinus may support the theory that the lesions are formed during the embryonic period. Furthermore, the cases with multiple lesions (including multiple PAVFs, PAVF complicating PMAVF, AVM and peripheral congenital defects) may indicate that these patients are affected in the early stage of embryonic development. This is also consistent with previous genetic studies, which found that more than half of these patients carry genes related to hereditary vascular disease (such as hereditary hemorrhagic telangiectasia and capillary malformation-arteriovenous malformation). These genes may cause the abnormal differentiation of endothelial cells or the subsequent failure of the remodelling and maturing of the vascular network, when multiple lesions are more likely to form.13–16
Pathological progression and associated secondary changes
Haemodynamic changes occur immediately after fistula formation, creating a high-flow, low-resistance state. This causes changes in blood composition and haemodynamics inside the vein and sinus, which may cause a gradual increase in their inner diameter and is followed by intimal hyperplasia, stenosis and even occlusion.17 18 Venous varix seems to be the first characteristic change after the formation of PAVF because it can be seen in almost all pediatric patients (97.6% in our study), and less often in the adult group.6 In pediatric patients, varix does not have a significant correlation with haemorrhage because the good vascular wall elasticity of pediatric patients exert a buffer effect to tolerate high arterial flow pressure and consequently decreases the risk of haemorrhage. With the increase in shunting flow, secondary radiological and symptomatic changes appear. In our study, both dynamic sinus obstruction and cardiac enlargement occurred in 50.0% of pediatric patients, indicating that the arteriovenous shunt affects not only their normal cerebral circulation but also their systemic circulation.
In neonates and infants, medullary veins are the main absorption pathway of cerebrospinal fluid (CSF), and the driving force of this absorption mechanism is the sump effect of negative pressure in the dural sinus.19 The existence of high-flow PAVF causes venous hypertension of the dural sinus and will cause CSF malabsorption, which will be aggravated by pulmonary hypertension, skull base maturation and closure of cranial sutures.20 As a result, cerebral ventricular enlargement, brain atrophy, melting brain syndrome, developmental delay and other changes will gradually develop.21 In our series, 21 cases (50.0%) had dynamic sinus obstruction, 61.9% of them showed cerebral ventricle dilation and 14.3% of them presented with developmental delay.
This phenomenon suggests that patients with dynamic obstruction, even the patient is asymptomatic, should be treated early to avoid secondary brain injury due to cerebrospinal fluid absorption disorders.
Treatment strategies and long-term prognosis
Generally, occlusion of fistulas can be achieved by microsurgical disconnection, endovascular embolisation or hybrid operation.6 22–24 With improvements in neurointerventional materials and techniques, its less invasive nature and the ease of identifying the angioarchitecture have made endovascular embolisation the first-line treatment.25–27
There are three challenges in the endovascular embolisation of PAVF: (1) the large size of the afferent and efferent vessels, associated with the high-speed blood flow of the lesion, makes it difficult for embolic materials to adhere around the fistula; (2) incomplete occlusion of the fistula and venous varix is likely to cause residual lesions or recurrence, of which the emergence of new small pial feeding arteries will make the reembolisation extremely difficult and (3) the sudden occlusion of a high-flow fistula may increase the pressure inside the feeding artery and cause blood flow stasis inside the draining vein, which may increase the risk of postoperative feeding artery rupture and draining vein acute thrombosis. Different techniques have evolved to counter these challenges, such as tandem balloon embolisation, balloon-assisted Glue embolisation, coil-assisted glue embolisation and Matas test-assisted embolisation.1 7 9 26 Recently, coil-assisted and balloon-assisted Glubran embolisation are increasingly chosen in our centre because they may provide sufficient time for the diffusion and coagulation of the glue, which will improve the cure rate and reduce the risk of embolic agent migration. Transarterial balloon-assisted glue embolisation was proven to be a feasible and effective option for high-flow pial AVFs in our previous study.9 However, postoperative venous thrombosis caused by blood flow stasis and thrombogenic glue is still a common complication (2/8, 25.0%) that requires attention. Coil-assisted glue embolisation has also been proven to be a safe and effective strategy for high-flow AVF. We reported the technical details in our previous study of high-flow perimedullary AVF.28 First, we usually place several large-diameter, long coils in the venous pouch and several oversized coils in the terminal of the feeding artery loosely to reduce flow and provide support for glue adhesion. Then, we inject variable concentrations of Glubran to occlude the feeding artery and fistula. It is not suggested that Glubran fill the venous varix too much because it is more likely to cause the formation of acute thrombosis in draining veins and a permanent mass effect.
De novo DAVF is an infrequent radiographic change after the total embolisation of PAVF and has rarely been reported previously.3 De novo DAVF (Cognard IIb, Borden II) was found in four of our cases (9.5%), and all of them were younger than 3 years old. Preoperative DSA indicated that they all had dural sinus occlusion and dynamic sinus obstruction, the statistical analysis of which also showed correlations. In addition, severe sinus stenosis was noted in three of them. Combined with the high-risk factors that may contribute to the development of DAVF, we speculate that the formation mechanism of de novo DAVF may be as follows: (1) the change in pressure inside the dural sinus may cause an abnormal opening of communication between the dural arteries and sinus; and (2) after the occlusion of high-flow AVF, the blood flow in the dilated sinus reduces and slows down, followed by dural sinus thrombosis. This phenomenon also suggests that we should pay more attention to imaging follow-up of cured patients, especially younger patients with poor sinus drainage before surgery.
Limitations
There are certain limitations to our study. The relatively small sample size of the pediatric PAVFs population in our series was one of the main limitations because of the rarity of pediatric PAVFs.
Although endovascular embolisation has been proven to be the preferred treatment, different embolisation strategies may have different cure rates and different risks of complication. However, randomised controlled studies cannot be conducted to confirm which embolisation strategy is safer and more effective due to the limitation of the number of cases. Although pediatric PAVF is currently considered a congenital disease and is associated with certain genetic disorders (such as HHT and CM-AVM), however, this study did not perform genetic screening on every patient in this study, which is worthy of further investigation.
Conclusion
Pediatric PAVF is a distinct subgroup of intracranial arteriovenous shunt that has different angioarchitecture and clinical features between different age groups. Poor venous drainage is a major factor leading to the poor prognosis and the occurrence of de novo DAVF. Earlier preventive treatment is suggested in view of the early onset of radiographic changes and the delayed symptoms. Endovascular embolisation is safe and effective for pediatric PAVFs, and coil-assisted or balloon-assisted Glubran embolisation might be a better choice. Imaging follow-up is necessary to detect the residual lesion and de novo DAVF, as they still carry a potential risk of haemorrhage and need further treatment.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Footnotes
JL and ZJ contributed equally.
Contributors We want to thank all the patients for their participation in this research. Conception and design: JL, LB and FY. Acquisition of the data, analysis and interpretation of the data, and critically revising the article: all authors. Drafting the article: JL and ZJ. Reviewed submitted version of manuscript: XZ, GL and FY. Approved the final version of the manuscript on behalf of all authors: GL and HZ. Administrative/technical/material support: all authors. Study supervision: GL and HZ. Responsible for the overall content as guarantors: GL and HZ.
Funding This study was funded by Natural Science Foundation of Beijing (7222081), National Natural Science Foundation of China (82101369) and Science Program for Fostering Young Scholars (QNPY2020009).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note JL and ZJ are joint first authors. GL and HZ are joint corresponding authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}