

Abstract
Background Although vascular dementia (VaD) is not uncommon in the hospital, most studies on VaD are community based. This study on VaD is the first to use a national hospital information system (HIS) in China.
Methods This study was a hospital population-based cohort study, and data were acquired from the Hospital Quality Monitoring System, a Chinese national database that covers 1531 tertiary hospitals in China. The medical records in the HIS included demographic information, diagnoses, procedures, expenses, etc. VaD was diagnosed by hospital attending physicians and identified by the International Classification of Diseases (ICD) 10 code (F01.0-F01.9).
Results 1259 (82.23%) tertiary hospitals were included in this study, and 274 230 hospitalisation records of 123 700 VaD patients from 2016 to 2018 were identified for analysis. VaD (51.27%) was the most common type of dementia in hospitalised patients. The age-adjusted and sex-adjusted hospital incidence of VaD was estimated to be 2.97 per 100 000 person-years (95% CI 2.92 to 3.02). The mean age of VaD patients admitted to hospitals was 74.13±10.88, with more male (61.0%) patients. The main comorbidities were hypertension (67.2%), heart disease (63.6%) and cerebral infarction (55.5%). The mortality rate of VaD in hospital was 28.91‰ (95% CI 28.0 to 29.9) between 2016 and 2018. The top 1 cause of death due to VaD was pneumonia and other respiratory disorders.
Conclusions VaD is the most common form of dementia in hospitalised patients. It casts huge burdens on affected patients and their caregivers. Vascular risk factors are prevalent in VaD patients. Reducing these factors is essential to improve patient care. The leading causes of death by VaD are pneumonia and other respiratory disorders. Hospital care and the management of respiratory illness are critical for VaD care in the hospital.
What is already known on this topic
Studies on vascular dementia (VaD) incidence in China are limited and lack of national studies.
What this study adds
This is the first study to use a national hospital information system database in China.
How this study might affect research, practice or policy
The study has found that VaD as the most common form of dementia in hospitalised patients. This helps to raise awareness in VaD in the hospital. It also warrants further research in identifying and monitoring risk factors in stroke patients.
Introduction
Rates of dementia are increasing dramatically, which imposes a substantial social and economic burden in China.1 Due to the large population of cerebrovascular stroke patients in East Asia, cognitive impairment by vascular aetiology is one of the leading causes of dementia in that region.2 Patients and their caregivers are concerning about poststroke dementia,3–5 since possibility of poststroke dementia in 1 year reaches nearly 50 times higher than general population.4 About 1 in 10 patients develop poststroke dementia in 12 months after the first stroke hit.5 Two million new stroke cases appeared every year in China.6 The prevalence of vascular dementia (VaD) has risen since 1999.7 The burden is increasing due to physical disability secondary to stroke and cognitive impairment related to stroke.
Previous estimates of dementia burden, including VaD, might be underestimated in China because these studies were based on small datasets and limited by population sampling.1 The prevalence of VaD in China from 2009 to 2019 was different between the north and the south or between urban and rural areas.7 However, most studies were conducted locally at the provincial or municipal levels with limited sample size.7 To overcome these limitations, we used the Hospital Quality Monitoring System (HQMS), a Chinese national database, to assess the incidence, comorbidities, medical expenses and demographic characteristics of VaD.
Methods
Data sources and collection
This study used the HQMS database, which was developed by the National Health Commission of China.8 9 Designed to evaluate the healthcare status all over China, this information system was launched in 2011 to collect and to quality control medical records from the hospital information system (HIS) at each public tertiary hospital. Tertiary hospitals have a minimum requirement of 500 beds and are the top tier of the medical system in China.10 HQMS consistently collects the information of inpatient medical records, including the diagnosis, demographic characteristics, conditions at discharge, medical expenses, etc. This unique national HIS allows universal data collection. The present study was a project by the China National Clinical Research Center for Neurological Diseases and the China National Center for Quality Control of Neurological Diseases. The study was approved by the Institutional Review Board at Beijing Tiantan Hospital.
Data sources also included the China National Bureau of Statistics for the population’s demographic information (http://www.stats.gov.cn).
Study population
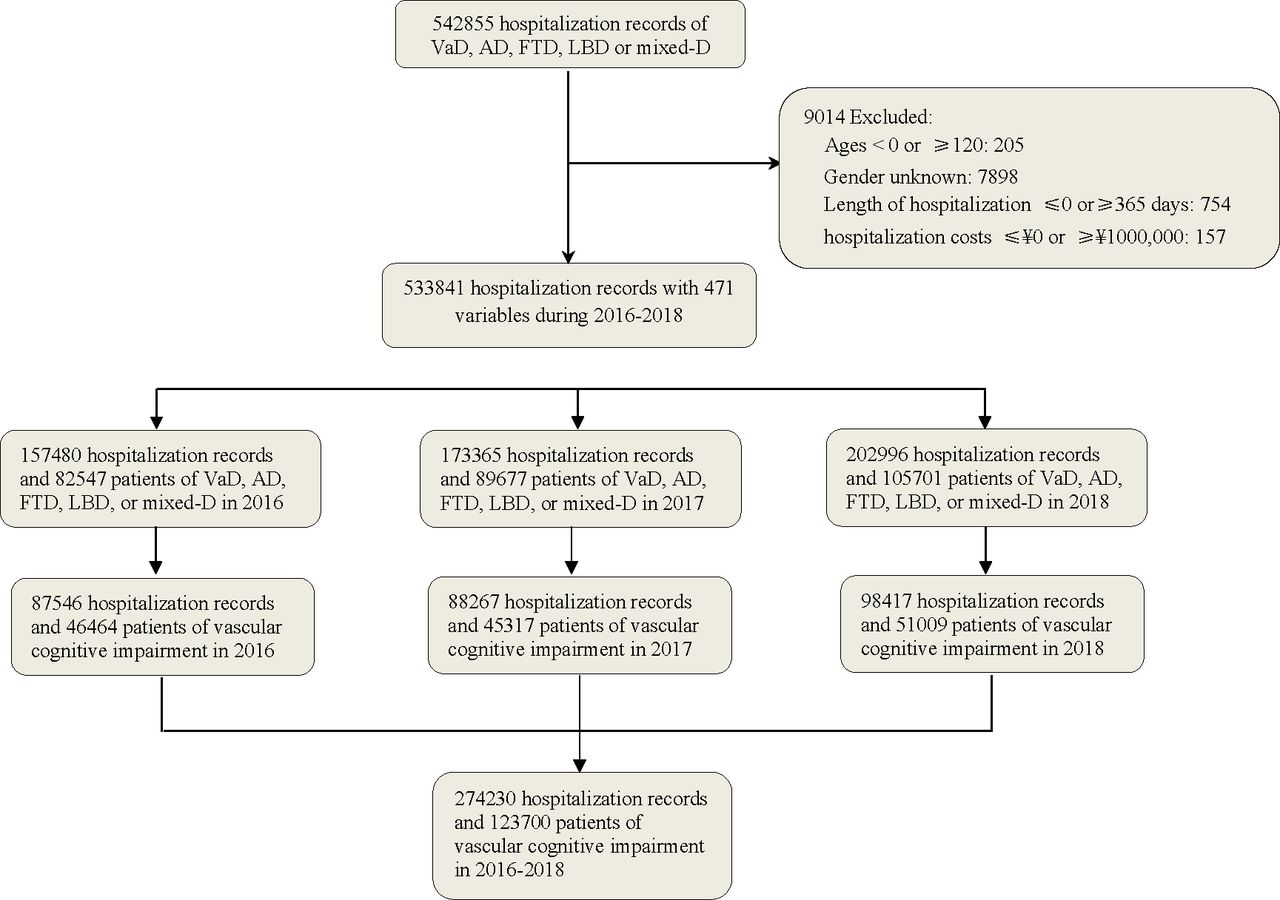
A total of 1531 tertiary hospitals were surveyed. A total of 1259 (82.23%) of them that had standardised electronic medical records were included in this study. A total of 274 230 hospitalisation records of VaD were obtained from the HQMS database between 1 January 2016 and 31 December 2018 (figure 1).

Patient records were obtained from the HQMS database between 1 January 2016 and 31 December 2018. AD, Alzheimer’s disease; FTD, frontotemporal dementia; HQMS, Hospital Quality Monitoring System; LBD, Lewis body dementia; VaD, vascular dementia.
The diagnosis of VaD
VaD was diagnosed by hospital attending physicians according to Chinese Guidelines for the diagnosis and treatment of vascular cognitive impairment.11 The Chinese guideline was adopted from the classification of vascular cognitive impairment.12 13 Clinical and neuropsychological evaluation and imaging studies were performed. Patients with VaD showed severe cognitive impairment that affects activities of daily living, occupation or social skills.11 VaD includes four main subtypes: (1) vascular risk factor-associated VaD; (2) ischaemic VaD; (3) haemorrhagic VaD; and (4) mixed dementias (VaD and Alzheimer’s dementia). This classification is consistent with the current Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-V).14 VaD was identified by ICD 10 code (F01.0-F01.9).
The criteria of inclusion and exclusion
The records were excluded for those ages <18 or ≥120 years, gender unknown (probably due to missing citizen identification cards), length of hospitalisation ≤0 or ≥365 days and hospitalisation costs ≤ ¥0 or ≥¥1 000 000. Duplicated patients were excluded each year through individual identification in the database.
Statistical analysis
The annual incidence of VaD in the hospital was estimated by dividing the number of patients by the local populations from 2016 to 2018. The incidence of VaD was calculated in male and female groups and analysed across age groups by 0–40 years and every 5 years after 40 years. We used Poisson distribution to obtain 95% CIs. Age was calculated and expressed as mean±SD. The number of hospitalisations, length of hospital stay, total hospitalisation costs and self-pay costs were presented as medians with quartile 1 and quartile 2. Gender, occupation, access to hospitals, comorbidities and payment methods were presented as the number and proportion. All analyses were performed with SAS software (V.9.4, SAS Institute Inc). The hospital rate distribution map was drawn using the Arcgis V.10.4 Software for Windows.
Results
Incidence of VaD
We collected 274 230 hospital records of 123 700 VaD patients from 2016 to 2018 (figure 1). The hospital incidence of VaD was estimated to be 2.97 per 100 000 person-years (95% CI 2.92 to 3.02) during the study period. It was 3.36 per 100 000 (95% CI 3.33 to 3.39) in 2016, 3.26 per 100 000 (95% CI 3.23 to 3.29) in 2017 and 3.66 per 100 000 (95% CI 3.63 to 3.69) in 2018. Some patients were admitted multiple times over the study period. From 2016 to 2018, about 24 047 (19.44%) patients admitted to hospital for VaD, and other 99 653 (80.56%) patients were for comorbidities. The majority of VaD patients (111, 257, 89.9%) were over 60 years old. Among these elderly patients, the hospital incidence of VaD was 11.86‰ (95% CI 11.80 to 11.93) between 2016 and 2018.
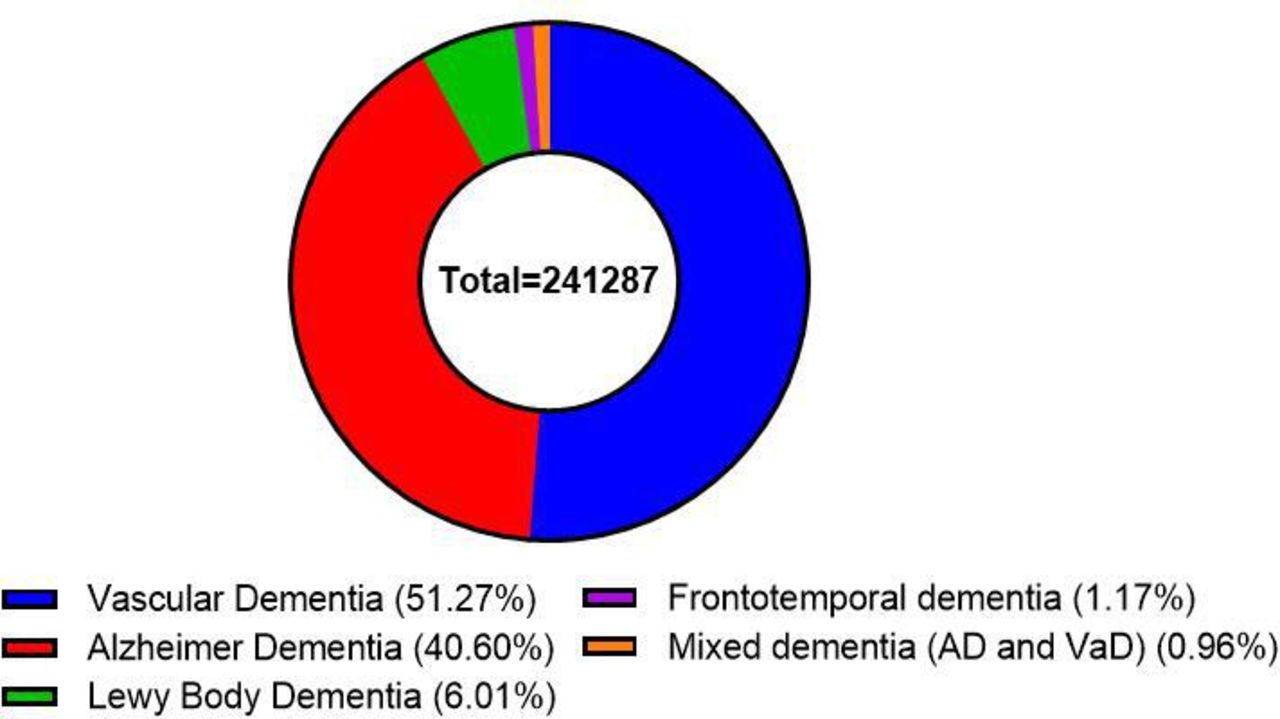
A total of 542 855 hospital admissions of all main types of dementia were recorded from 2016 to 2018, including VaD, Alzheimer’s disease (AD), mixed dementia (mixed-D, mixed AD and VaD), Lewis body dementia (LBD) and frontotemporal dementia (FTD). From 2016 to 2018, about 2 77 925 patients were admitted to the hospital diagnosed with one of the five main types of dementia. VaD had the highest percentage (123 700 patients, 51.27%), followed by AD (40.60%), LBD (6.01%), FTD (1.17%) and mixed-D (0.96%) (figure 2).

Between 2016 and 2018, 123 700 patients had VaD (51.27%), followed by AD (40.60%), LBD (6.01%), FTD (1.17%) and mixed-D (0.96%). AD, Alzheimer’s disease; FTD, frontotemporal dementia; LBD, Lewis body dementia; VaD, vascular dementia.
Regional distribution
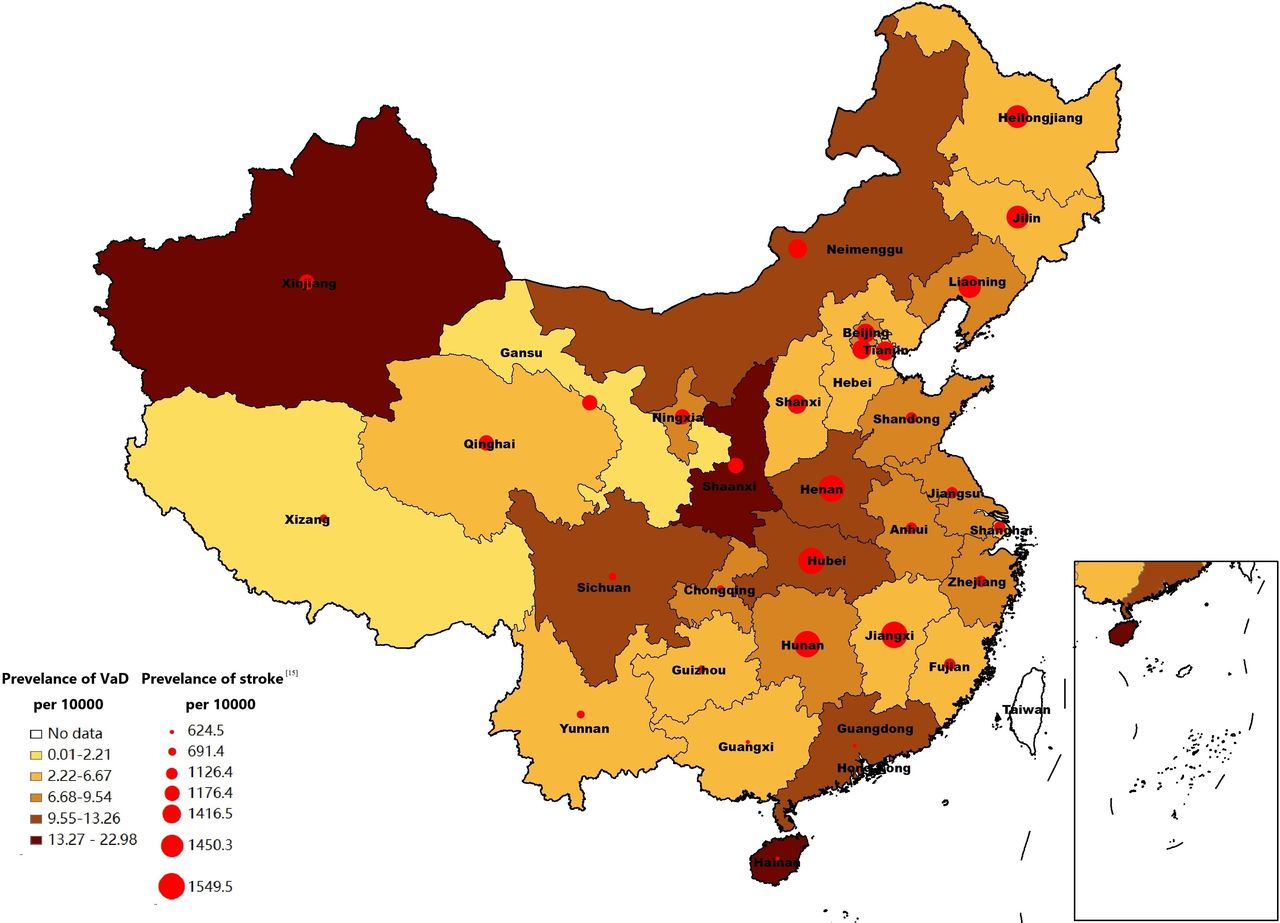
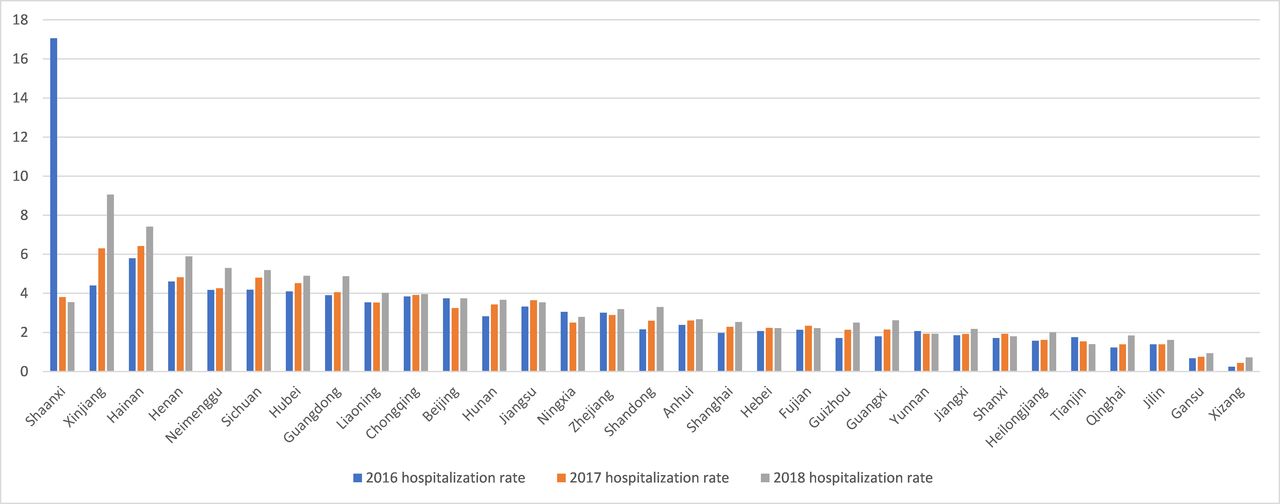
The provinces with the highest VaD hospitalisation rates were Shaanxi (22.98 per 100 000), Xinjiang (18.10 per 100 000), Hainan (16.64 per 100 000), Henan (13.26 per 100 000) and Neimenggu (12.74 per 100 000) between 2016 and 2018. Except for Shaanxi, which had the highest incidence in a single year in 2016 (17.07 per 100 000), the other top four provinces had an increasing number of cases from 2016 to 2018. The five provinces with the lowest VaD hospitalisation rates were Xizang, Gansu, Jilin, Qinghai and Tianjin (figures 3 and 4).

In the map of China, stroke prevalence (red dots) and VaD hospitalisation rate (coloured squares) were overlapped in each province. VaD, vascular dementia.

Showed the distribution of VaD in each province in 2016–2018. VaD, vascular dementia.
Since stroke is a major contributing factor to VaD, we correlated the prevalence of stroke15 with that of VaD in China. In west China, a low prevalence of stroke correlated with a low incidence of VaD, which may reinforce stroke as a risk factor for VaD. However, Xinjiang was an outlier in west China, and the incidence of VaD was much higher than the prevalence of stroke. This mismatch of high VaD incidence and low stroke prevalence was also present in several central and northern provinces in China (figure 3).
Demographics
Patients with VaD had an average age of 74.13±10.88 (table 1). VaD incidence peaked at 75–84 years and then decreased (figure 5 and online supplemental figure 1). VaD occurred more in male patients (61.0%) than female patients (table 1 and online supplemental figure 1). Nearly 39.6% of VaD patients were retired, 33.44% employed, 20.4% rural agricultural workers and 6.5% unemployed. About 22.5% of patients were admitted to the hospital through emergency rooms and 61.4% through outpatient clinics (table 1).
Supplementary data
Demographic characteristics of VaD patients in tertiary hospitals in China, 2016–2018

Showed the distribution of VaD at different age in 2016, 2017 and 2018. VaD, vascular dementia.
Cost of hospitalisation
Average number of hospitalisations was 2.96±0.17, with 36.18% patients hospitalised two or more times. The median of hospital stay length was 11.00 (IQR 8.00–17.00) days. It was shortened from 12 (IQR 8–18) days in 2016 to 11 (IQR 8–17) days in 2018. The median hospitalisation cost was¥10 807.92 (¥1=$0.15, IQR 6838.84–18 535.30) with a median self-funded cost of¥3947.32 (IQR 1806.86–8774.79). The total cost of hospitalisation in VaD patients is ¥0.23 billion from 2016 to 2018. The hospitalisation cost was stable from 2016 to 2018, while the self-pay cost decreased from ¥4377.51 (IQR 1932.24–9162.54) in 2016 to ¥3592.56 (IQR 1624.15–8373.61) in 2018. About 71.7% of patients were covered by government-subsidised Urban Employee Basic Medical Insurance, Urban Resident Basic Medical Insurance and the New Rural Cooperative Medical Insurance. Self-paid patients account for only 9.2%, and patients with commercial health insurance covered 0.3% (table 1).
Associated comorbidities
Vascular risk factors, such as, hyperlipidaemia (16.5%), atherosclerosis (30.8%), type 2 diabetes (42.4%) and hypertension (67.2%) were prevalent in VaD patients. Most VaD patients experienced a stroke (68 691, 55.5%). A total of 16 472 (10.9%) had other cerebral vascular diseases, and 38 110 (30.8%) had cerebral vascular disease sequelae. A total of 78 724 (63.6%) VaD patients developed heart disease, and 19 191 (15.5%) developed respiratory diseases. Metabolic abnormalities (acid–base and electrolyte disorders, other amino acid metabolism disorders) accounted for 33 037 (26.7%) VaD cases (table 1).
Mortality
A total of 3577 VaD patients died from 2016 to 2018, and the in-hospital mortality rate of VaD was 28.91‰ (95% CI 28.0 to 29.9). Hospital mortality among individuals with VaD was decreased from 25.16‰ in 2016 to 23.78‰ in 2018. The average age at death was 82.17±8.10 years, which was relatively stable over the study period (table 2). A percentage of 66.5 of VaD patients were male (table 2) who had a higher death rate (31.56‰, 95% CI 30.31 to 32.81) than female patients (24.79‰, 95% CI 23.40 to 26.17, figure 6). Most patients died in the neurology department (17.6%), intensive care unit (13.0%) and geriatric department (12.4%). The first cause of death was pneumonia (21.72%), followed by cerebral infarction (10.76%), other respiratory disorders (10.60%), COPD (5.45%) and respiratory failure (4.5%) (table 2).
Mortality of VaD patients in tertiary hospitals in China, 2016–2018

Showed the death rate of VaD in total, male and female in 2016–2018. VaD, vascular dementia.
Discussion
Most epidemiological studies on dementia used community-based cohorts.3 16 17 The strength of this study is that it is an all-inclusive hospital based cohort using a national database in China. We found that VaD has the largest proportion of all enrolled dementia in the hospital. The number of hospitalised VaD patients increased from 2016 to 2018 in China, comparable with a similar trend in other developing countries.4
Between 1990 and 2010, the estimated incidence of VaD was 2.42 cases per 1000 person-years in China.1 A recent cross-sectional study estimated that the prevalence of VaD among those over 60 years was 1.6% (1.5–1.7).17 However, since that study was community based and most VaD cases were diagnosed in the hospital, the prevalence was likely underestimated. Our study provides much-needed complementary data to community-based cohort studies.
The high incidence of VaD is likely due to the fact that China bears the very huge burden of stroke in the world. A nationwide door-to-door survey in 2013 found that the prevalence and incidence of stroke were 1596/100 000 and 345/100 000, respectively.15 The incidence of stroke has increased in China over the past 20 years,6 raising concerns of VaD as its sequela. Most VaD patients were over 60 years old. The incidence of VaD at different ages in this study was parallel to that of stroke. This finding further illustrates the temporal and causal relationship between stroke and VaD. VaD and stroke also had a similar male preference.18 The VaD patients are mostly distributed in the central, northern and northwestern regions and are less frequent in the eastern and southeastern regions. However, the geographical distribution of VaD patients does not match the prevalence of stroke in several regions. This discrepancy suggests that besides the underlying vascular contribution to the pathogenesis of VaD, region-specific environment, culture and diet may also play a role. This finding warrants further investigation to identify modifiable factors to prevent VaD.
VaD casts a tremendous economic burden on patients and their families. Among VaD patients, 33.44% were employed and 20.4% were rural agricultural workers. VaD impairs patients’ ability to work and have a functional life. Previous analysis of dementia burden in China based on small datasets, causing the underestimating of it. In Asian and Latin American countries, the burden of neurological disorders is mostly from cerebrovascular diseases.19 Previous study estimated the yearly dementia expenses in developing countries as US$73 billion, but patient care also demands societal resources, which seem scarce.20 The mean medical cost is US$3401.71 per dementia patient worldwide.21 Our study showed that the hospitalisation cost for dementia is ¥0.23 billion yearly, with an average cost of ¥18 252.49 per patient (median cost ¥10 807.92). China’s government-sponsored basic health insurance that covered 71.7% of VaD hospitalisation. Although the total hospitalisation cost was stable from 2016 to 2018, the self-pay cost decreased throughout the duration of the study.
A study on the comorbidity of dementia patients (AD, VaD and other types) found VaD had the heaviest burden as measured by Charlson Comorbidity Index (CCI). Male patients had a higher CCI and lengthier hospital stays than female patients.22 The common comorbidities were stroke,22 cardiovascular diseases22 23 and chronic pulmonary disease.22 24 In this study, more than half of VaD patients experienced cerebral infarction, other cerebral vascular diseases (including aneurysm) and related sequelae. Similar risk factors were shared in stroke and dementia, and each increases each other’ s risk.16 The Oxford Vascular Study found the incidence of poststroke cognitive impairment at 1 year was estimated to be 34.4%, 8.2%, 5.2% in patients with severe stroke, minor stroke and transient ischaemic attack.4
In this study, the prevalence of vascular risk factors, such as atherosclerosis, hyperlipidaemia, diabetes25 and hypertension,26 was high. Cardiovascular risk factors are associated with neurodegeneration and vascular lesions in the brain.27 28 In the Hisayama Study, increased blood pressure variability is another significant risk factor for dementia or VaD in an elderly Japanese population.26 Hypertension seems to be associated with increased white matter hyperintensity range and shrinked brain.29 VaD and cardiovascular diseases also share many vascular risk factors, and cardiovascular diseases can contribute to cognitive decline.23 The majority of VaD patients (63.3%) developed heart disease and 15.5% VaD patients developed respiratory diseases (table 1). Risks of clinically diagnosed AD and VaD increased in association with diabetes.30 31
Yearly all-cause mortality in China from 2016 to 2018 was 7.09‰, 7.11‰ and 7.13‰, respectively, according to the national data (http://www.stats.gov.cn/). In the present study, the hospital mortality rate of VaD was 28.91‰ from 2016 to 2018. A study in the USA discovered that dementia caused about 16% of all deaths, and roughly 64% patients died withdiagnosis of dementia.32 In our study, the average age at death was 82.17±8.10 years. Male patients had a higher death rate (31.56‰) than females (24.79‰). The most common cause of death in the hospital for VaD patients was lung disease.33 34
There are several limitations in our study. First, outpatient records were not available in this study. Patients with mild VaD may elude diagnosis or be followed in the outpatient clinic; thus, the realistic incidence could be higher than our estimate. This hospital-based population does not necessarily mirror the incidence of VaD in a general population. Second, we could not calculate the prevalence of VaD in this study. The prevalence of VaD in China can be estimated when the HQMS has longer follow-up data in the future. Third, the diagnosis of VaD may have been mixed with other types of dementia, for example, AD. In tertiary hospitals, MRI imaging (in case of MRI incompatibility, CT scans were used instead) is commonly available to make the diagnosis of VaD in combination with neurological and neuropsychological evaluation. Cases were discussed among medical staff and were confirmed by hospital attending physicians. Medical records in the HQMS were quality checked by a quality assurance physician and a coder to affirm the proper entry of the ICD-10 code. Since biomarker studies (such as amyloid and tau) were not commonly used in the hospital setting, the diagnosis of VaD, which mostly based on imaging studies, temporal relationship with stroke and cognitive testing, is likely to be most accurate among all types of dementia. Fourth, the HIS as a general database does not have the data on VaD subtypes nor the duration of poststroke duration for establishing the diagnosis of dementia. According to a substudy of Chinese Stroke Registry, the occurrence rate of cognitive impairment was 52.38%, 35.55% and 34.16% at 2 weeks, 3 months and 12 months, respectively.35 This suggests that post stroke cognitive impairment has a tendency to fluctuate.
Conclusion
Our study is the first to obtain the incidence of hospitalised VaD across all age groups in an all-inclusive population sample. The accuracy and rigour of these estimates were enhanced by this comprehensive national database. Our study fills in the gap of Chinese epidemiological VaD data. The study also calls for more efforts for identifying modifiable risk factors, investing in preventing these risk factors and concerning about the burden of VaD.
Data availability statement
Data are available on reasonable request. The study protocol, statistical analysis plan and deidentified data that underlie the results of this article will be available for investigators after approval by the Institutional Review Board of China National Clinical Research Center for Neurological Diseases (Beijing, China). Please email the corresponding author for more information.
Ethics statements
Patient consent for publication
Ethics approval
Hospital Quality Monitoring System (HQMS) study is a national dataset for the population, not for an individual patient, so no ethical review is required. This study used the HQMS database. Since data were queried based on the population, not any individual patient, Institutional Review Board is not required.
Acknowledgments
We would like to thank the centres, patients and their caregivers who participated in the Hospital Quality Monitoring System Research.
Footnotes
YW and SL contributed equally.
Contributors YW, SL and JS designed the study. YW, SL and JS did the scientific literature search. QZ analysed data. YW, SL and JS created the tables. YW, SL and JS wrote the manuscript, and all authors edited revised the report. All authors read and approved the manuscript. JS and YW are responsible for the overall content as guarantor.
Funding This study is supported by the Beijing Municipal Science & Technology Commission (Grant No. Z181100001518005) and the Strategic Priority Research Program of the Chinese Academy of Sciences (XDB39000000).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}