

Article Figures & Data
Figures
- Figure 1
cSVD groups. CAA pattern was defined by any number of CAA features ((A) multiple subcortical spots pattern on FLAIR (yellow arrows), (B) lobar lacunes on FLAIR (inset, orange arrow) and (C) severe CSO EPVS as seen on T2 (inset, green arrows)), whereas HTN-cSVD pattern includes one or more of the features in the bottom panel, which are classically attributed to HTN-cSVD ((D) peribasal ganglia WMH on FLAIR (yellow arrows), (E) deep lacunes on FLAIR (inset, orange arrow) and (F) severe basal ganglia EPVS as seen on T2 (inset, green arrows)). The mixed NHIM group included at least one imaging finding from both the CAA pattern and HTN-cSVD pattern. No NHIM had none of these imaging characteristics.CAA, cerebral amyloid angiopathy; CSO, centrum semiovale; cSVD, cerebral small vessel disease; EPVS, enlarged perivascular spaces; FLAIR, fluid-attenuated inversion recovery; HTN-cSVD, hyperintensive cerebral small vessel disease; NHIM, non-haemorrhagic imaging markers; WMH, white matter hyperintensities.
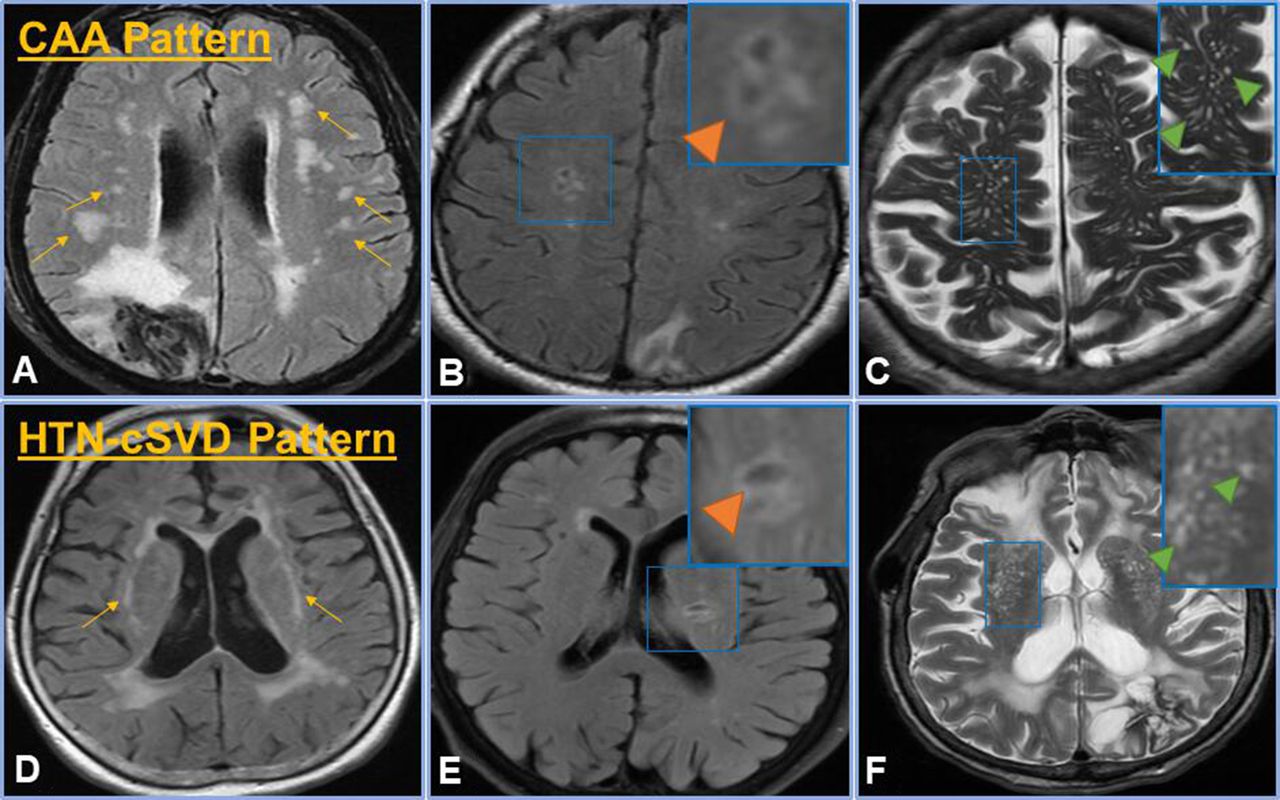
- Figure 2
Participant selection methodology. The above schematic depicts the total number of patients included in the study (n=1791). Of these, 1289 (72%) received an MRI scan of the brain. From this cohort, patients were diagnosed with either probable CAA, possible CAA (isolated lobar ICH) or HTN-cSVD. Lastly, the patients with isolated lobar ICH were further stratified into patients with HTN-cSVD pattern, CAA pattern, mixed NHIM or no NHIM. CAA, cerebral amyloid angiopathy; HTN-cSVD, hyperintensive cerebral amyloid angiopathy; ICH, intracerebral haemorrhage; NHIM, non-haemorrhagic imaging markers.
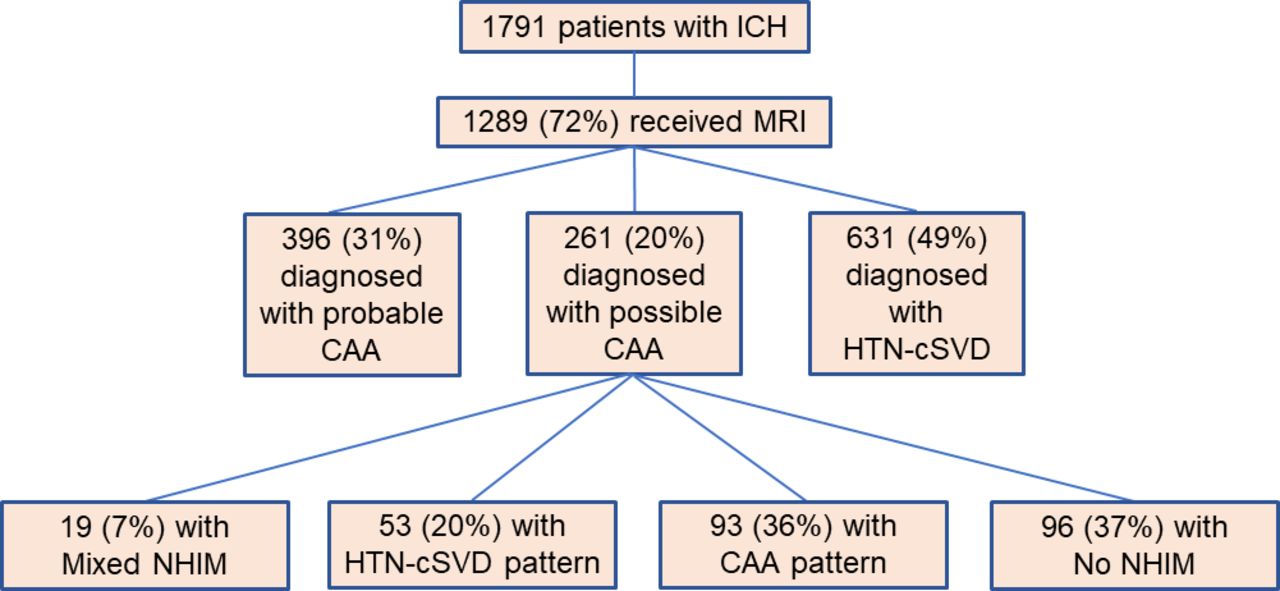
- Figure 3
Frequency of NHIM in cSVD group. This figure depicts the frequency of haemorrhagic markers found in each subgroup of isolated-LICH. The majority of patients with the CAA pattern and the HTN-cSVD pattern have one marker (with the maximum being three markers). Patients with mixed NHIM can have up to four markers, and patients with no NHIM will have zero markers (by definition). CAA, cerebral amyloid angiopathy; cSVD, cerebral small vessel disease; HTN-cSVD, hyperintensive cerebral small vessel disease; LICH, lobar intracerebral haemorrhage; NHIM, non-haemorrhagic imaging markers.
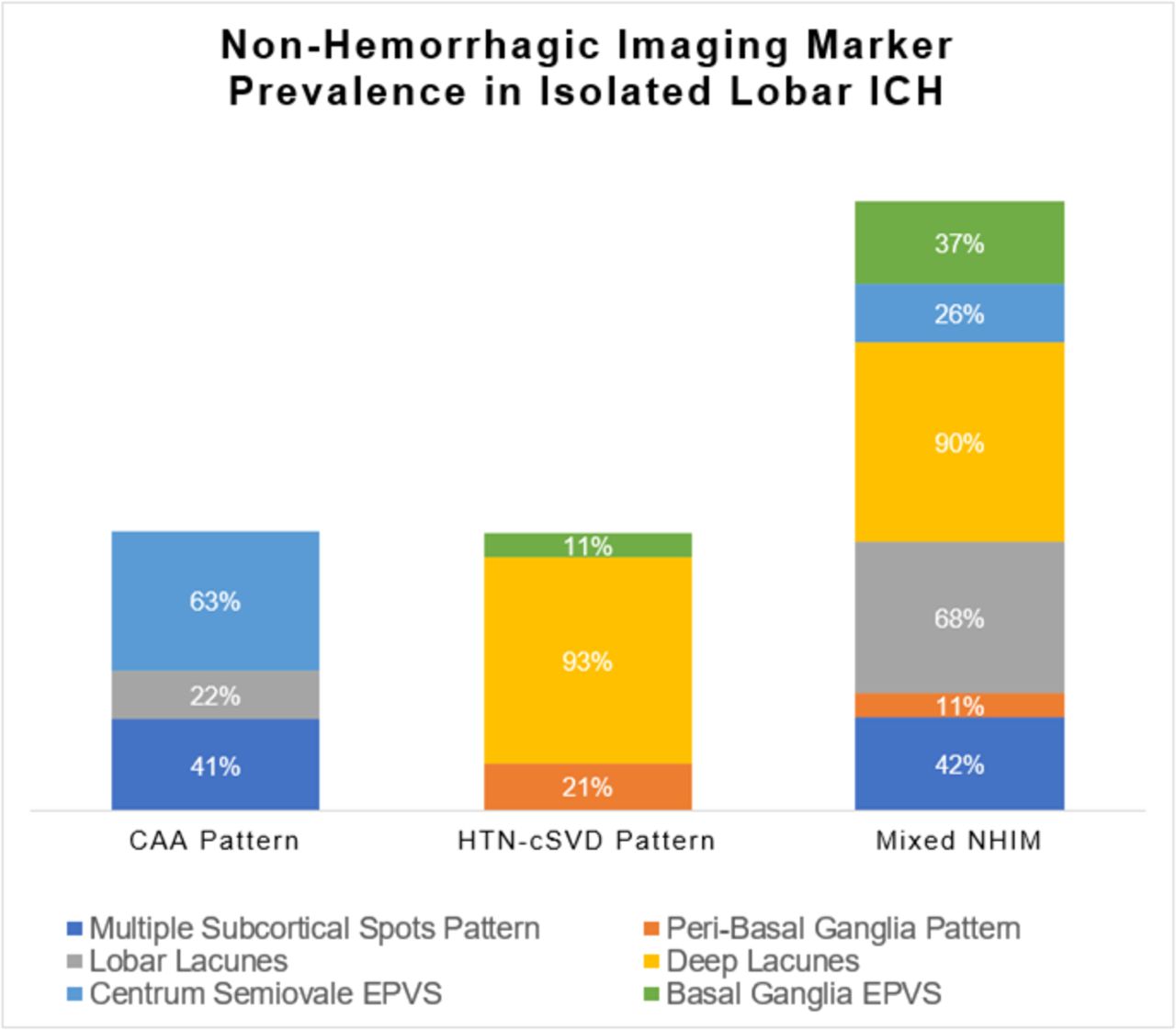
- Figure 4
NHIM prevalence in isolated lobar -ICH. This figure depicts the prevalence of each NHIM found in the subgroups of isolated lobar -ICH. Multiple subcortical spots patterns were the most common feature in the CAA pattern, whereas deep lacunes were the most common feature in both the HTN-cSVD pattern and the mixed NHIM pattern. CAA, cerebral amyloid angiopathy; EPVS, enlarged perivascular spaces; HTN-sCVD, hypertensive cerebral small vessel disease; ICH, intracerebral haemorrhage; NHIM, non-haemorrhagic imaging markers.




Tables
- Table 1
Baseline characteristics of patients with isolated-LICH (n=261)
Age (years), mean±SD 73 (±12) Female sex 147 (56) Race White 226 (87) Black 16 (6) Asian 10 (4) Hispanic 8 (3) Other 1 (0) Vascular risk factors Hypertension 193 (74) Hyperlipidaemia 131 (50) Diabetes 40 (15) Coronary artery disease 38 (15) Atrial fibrillation 43 (16) Prior stroke 43 (16) Substance use Smoking history 66 (25) Alcohol abuse 60 (23) Dementia 23 (8) Antithrombotic therapies None 136 (52) Antiplatelet 94 (36) Anticoagulant 31 (12) Glasgow Coma Scale score, median (IQR) 15 (13, 15) Systolic blood pressure (mm Hg), mean±SD 162 (±29) Diastolic blood pressure (mm Hg), mean±SD 85 (±16) Laboratory values, mean±SD White blood cell count (×103/µL), mean±SD 9.8 (±4.3) Haemoglobin (g/dL), mean±SD 13.6 (±1.8) Platelets (×103/µL), mean±SD 232 (±67) SCr (mg/dL), mean±SD 0.97 (±0.44) International normalised ratio, mean±SD 1.3 (±0.8) LVH 59 (23) CT findings Presence of perihaematoma oedema 236 (90) Presence of subarachnoid haemorrhage 84 (32) Presence of intraventricular extension 86 (33) Haemosiderin-sensitive MRI sequence GRE 182 (70) SWI/SWAN 73 (28) Other 6 (2) Treatments Extraventricular drain placement 28 (11) Surgical evacuation 30 (12) Outcomes Length of stay, median (IQR) 7 (4, 12) Poor outcome 120 (46) In-hospital mortality 93 (36) This table shows the baseline characteristics of patients with isolated-LICH. Data are counts (n) and percentages (%), means and SD, or medians and IQRs. Poor outcome was considered to be a discharge modified Rankin Scale score >2.
GRE, gradient echo sequences; LICH, lobar intracerebral haemorrhage; LVH, left ventricular hypertrophy; SCr, serum creatinine; SWAN, susceptibility-weighted angiography; SWI, susceptibility weighted imaging.
- Table 2
Comparison of risk factors among single LICH groups
CAA pattern (n=93) HTN-cSVD pattern (n=53) Mixed NHIM (n=19) No NHIM (n=96) Age (years), mean±SD 72.5±10.6 78.7±10.3* 80.4±8.9† 68.1±13.7‡ Female sex 49 (53) 31 (59) 14 (74) 53 (55) Hypertension 71 (76) 40 (76) 17 (90) 65 (68) Hyperlipiaemia 47 (51) 30 (57) 7 (37) 47 (49) Diabetes 13 (14) 9 (17) 3 (16) 15 (16) Coronary disease 12 (13) 11 (21) 2 (11) 13 (14) Atrial fibrillation 18 (19) 11 (21) 4 (21) 10 (10) SCr (mg/dL), mean±SD 0.96±0.25 1.00±0.32 0.99±0.33 0.97±0.63 LVH 17 (20)§ 25 (50)¶ 7 (39)** 10 (12)†† The table above shows the patient demographics, frequency of vascular risk factors, and markers of HTN-cSVD (SCr and LVH) among the various subgroups of single LICH. Data are counts (n) and percentages (%) unless specified otherwise. Of note, p<0.05 when * is compared with ‡, † is compared with ‡, § is compared with ¶, ¶ is compared with ** and ** is compared with ††.
CAA, cerebral amyloid angiopathy; HTN-cSVD, hypertensive cerebral small vessel disease; LICH, lobar intracerebral haemorrhage; LVH, left ventricular hypertrophy; NHIM, non-haemorrhagic imaging markers; SCr, serum creatinine; SCr, serum creatinine.
- Table 3
Associations with LVH
Unadjusted Adjusted OR (95% CI) P value OR (95% CI) P value Age 1.03 (1.00 to 1.05) 0.038 1.01 (0.98 to 1.04) 0.724 Sex 1.07 (0.59 to 1.93) 0.828 0.98 (0.48 to 1.99) 0.957 Hypertension 0.81 (0.39 to 1.66) 0.561 0.93 (0.40 to 2.19) 0.872 Hyperlipidaemia 0.87 (0.49 to 1.58) 0.654 0.69 (0.33 to 1.44) 0.324 Diabetes 0.99 (0.44 to 2.24) 0.975 0.93 (0.36 to 2.42) 0.881 Coronary artery disease 1.50 (0.70 to 3.21) 0.293 1.17 (0.45 to 3.03) 0.752 Atrial fibrillation 2.10 (1.02 to 4.33) 0.044 1.72 (0.74 to 4.02) 0.210 Creatinine 2.22 (1.04 to 4.76) 0.040 2.20 (1.04 to 4.68) 0.040 CAA pattern 1.55 (0.82 to 2.94) 0.179 1.90 (0.78 to 4.66) 0.161 HTN-cSVD pattern 4.53 (2.32 to 8.83) <0.001 7.38 (2.84 to 19.20) <0.001 Mixed NHIM 2.06 (0.76 to 5.57) 0.157 4.45 (1.25 to 15.90) 0.019 This table shows univariate and multivariable associations between predictor variables and LVH.
CAA, cerebral amyloid angiopathy; HTN-cSVD, hypertensive cerebral small vessel disease; LVH, left ventricular hypertrophy; NHIM, non-haemorrhagic imaging markers.




{kind=link}
{kind=link}
{kind=link}
{kind=link}