

Abstract
Objective To characterise the clinical utility of transthoracic echocardiography (TTE) at the time of acute ischaemic stroke (AIS).
Background The utility of obtaining a TTE during AIS hospitalisation is uncertain.
Methods We studied AIS hospitalisations at a single centre (2002–2016). TTE abnormalities were classified as findings associated with: high stroke risk (Category I), cardiac events (Category II) and of unclear significance (Category III). We performed logistic regressions to predict Category I, II and III abnormalities. The odds of 1 year recurrent stroke hospitalisation captured by ICD 9 and 10 codes as a function of Category I, II and III abnormalities were assessed. Improvement in predictive capacity for 1 year recurrent ischaemic stroke hospitalisation beyond stroke risk factors was evaluated by net reclassification improvement.
Results There were 5523 AIS hospitalisations. Nearly 81% of admission TTEs were abnormal (18.7% Category I, 32.7% Category II, 72.8% Category III). Older patients with coronary artery disease, atrial fibrillation, hypertension, diabetes, and patent intracranial and extracranial vessels were likely to have an abnormal TTE. Category I finding was associated with lower odds of 1-year recurrent stroke hospitalisation (OR 0.54, 95% CI 0.30 to 0.96). Category I data significantly improved the predictive value for 1-year recurrent ischaemic stroke hospitalisation beyond stroke risk factors (net reclassification improvement 0.1563, 95% CI 0.0465 to 0.2661).
Conclusions TTE abnormalities associated with stroke and cardiac event risk were commonly detected during AIS hospitalisation. Detection of Category I TTE findings reduced the risk of recurrent stroke, potentially due to neutralisation of the cardioembolic source by targeted therapy, indicating the clinical utility of TTE.
What is already known on this topic
Transthoracic echocardiography (TTE) studies are routinely performed in patients hospitalised with acute ischaemic stroke (AIS). The utility of obtaining a TTE during AIS hospitalisation is uncertain.
What this study adds
We demonstrate that 18% of AIS TTE studies demonstrate high-risk cardioembolic sources of stroke and we identify clinical and radiographic predictors of these TTE findings. Detection of these abnormalities by TTE was associated with lower odds of 1 year recurrent stroke hospitalisation (OR 0.54, 95% CI 0.30 to 0.96) and improved the predictive capacity for 1 year recurrent ischaemic stroke hospitalisation beyond stroke risk factors.
How this study might affect research, practice, and/or policy
These findings may inform future guidelines and clinical practice regarding the utilisation of TTE during AIS hospitalisation to facilitate prevention of recurrent stroke.
Introduction
Patients with acute ischaemic stroke (AIS) routinely undergo transthoracic echocardiography (TTE) during the inpatient encounter, however the clinical utility of this study in patients who had a stroke is unknown. Cardiac abnormalities can coexist in patients with ischaemic stroke due to shared vascular risk factors. One meta-analysis demonstrated a prevalence of asymptomatic coronary artery disease (CAD) of 52% among patients with AIS and a 3% risk of myocardial infarction (MI) within 1 year in patients without any cardiac history.1 While some AIS and cardiac therapies overlap, others are uniquely aimed at each disease. Pharmacological, surgical and procedural interventions target certain cardiac conditions and decrease mortality, but are rarely used in patients without cardiac diagnoses.2 Quantifying cardiac abnormality frequencies and their progression over time in patients with AIS is critical to inform when to obtain a TTE for the purpose of mitigating risk of future stroke and cardiovascular events.
Prior studies describe the epidemiology of cardiac abnormalities detected by TTE in patients with AIS, however, these are limited by solely assessing findings pertinent to stroke prevention, cross-sectional design, small samples sizes and lack of generalisability due to being performed outside of the USA.3–5 Reflecting the paucity of evidence linking TTEs obtained during AIS admission and clinical outcomes, the yield of echocardiography in the AIS context is denoted as uncertain in the current guidelines.6
Clinicians face uncertainty about whether TTE in patients with AIS informs management to prevent future stroke and cardiovascular events while attempting to practice resource stewardship. Patient-level predictors of having a TTE abnormality during AIS admission need to be more clearly defined. It is unknown which patients with AIS with a prior TTE study will have a newly detected finding. Finally, it is important to determine whether detecting the presence of specific TTE findings during AIS hospitalisation are associated with risk of future stroke, MI and heart failure hospitalisation.
In this study, we aim to (1) Explore the frequency of findings on AIS admission TTE and their rates of progression over time, (2) Identify patient-level predictors of having specific TTE findings during AIS admission and new TTE findings if a prior study was normal, and (3) Determine the odds of 1 year hospitalisation for recurrent stroke, MI and heart failure associated with having specific TTE findings at the time of AIS admission.
Methods
Patient population
This retrospective study was performed at an academic institution from 2002 to 2016. The cohort was derived from the institution’s Get-With-The-Guidelines-Stroke database, a quality improvement initiative in which hospitals enter clinical and radiographic data of all patients hospitalised with a stroke diagnosis.7 Patients with AIS are identified retrospectively by administrative discharge ICD-9 and ICD-10 codes and prospectively by daily review of clinical logs. Data abstraction, entry and adjudication are performed by trained study personnel. There are logic checks and form controls to minimise data entry errors. The covariates in this study were age, gender, race, admission year, history of atrial fibrillation (AF), CAD/prior MI, hypertension (HTN), hyperlipidaemia (HLD), diabetes mellitus (DM), carotid disease, peripheral vascular disease (PVD) excluding the carotid artery, prior stroke or transient ischaemic attack, smoking, chronic kidney disease (CKD), heart valve prosthesis, National Institutes of Health Stroke Scale (NIHSS) at presentation (dichotomised as minor and major stroke by NIHSS <4 and >4),8 presenting symptoms, and home medications.
Hospitalisations were included in this cohort if age at admission was ≥18 years, AIS was diagnosed during hospitalisation and a TTE was performed during the AIS hospitalisation. Of the 8859 consecutive admissions to our hospital with AIS, a total of 5523 met these criteria. Subgroups consisted of admissions with (1) Prior, most recently performed TTE available in hospital system’s records (n=1106), (2) TTE performed ≥3 months after AIS hospitalisation (n=1077), and (3) TTE performed most recently prior to the AIS hospitalisation and at ≥3 months after the AIS hospitalisation (n=373).
Radiographic features
Radiographic information was extracted by natural language processing of radiology reports from each stroke admission encounter using Python programming language (Python Software Foundation, https://www.python.org/). All radiology reports were created by board-certified radiologists. We applied predefined regular expression sequences for specific radiographic findings to radiology reports of neuroimaging obtained during AIS admission including CT head without contrast, CT angiogram of head and neck, brain MRI, MR angiogram head and neck, carotid ultrasound, and conventional angiogram. Our Python codebase is uploaded on GitHub and available by request. We collected information about cortical location of stroke, supratentorial (defined as structures rostral to and including the thalamus) and infratentorial location of stroke, and the presence of any moderately or severely stenotic or occluded intracranial artery or extracranial carotid or vertebral arteries. We determined the accuracy of this automated method of radiology chart review by selecting 100 observations for each variable and blindly comparing values ascribed by human (RS) versus machine algorithm review of the radiology report.
Echocardiographic features
All patients in this cohort underwent a two-dimensional TTE during admission for an AIS. TTEs were performed by trained hospital sonographers and interpreted by board-certified echocardiographers. TTE images were collected per Intersocietal Accreditation Commission of Echocardiography standards and included colour Doppler, continuous wave and pulse wave data. Images were analysed in apical two-chamber and four-chamber views as well as parasternal long-axis and short-axis views.
We classified TTE findings into three mutually exclusive categories based on the reading echocardiographer’s hard-coded interpretations in the database: (1) Features associated with a high risk of cardioembolic stroke (Category I), (2) Abnormalities warranting timely cardiac workup and treatment not necessarily related to stroke management (Category II), and (3) Possible indicators of stroke aetiology and/or cardiac disease with no immediate therapeutic consequence but may warrant further monitoring and long-term risk factor management (Category III). High-risk cardioembolic sources are abnormalities outlined in the 1993 TOAST (Trial of Org 10172 in Acute Stroke Treatment) publication9 plus the presence of a patent foramen ovale (PFO) which are associated with evidence-based secondary stroke prevention treatments.10–12 Category I features included: left ventricular (LV) thrombus, PFO (ascertained by Doppler and/or agitated saline contrast), atrial septal aneurysm, intracardiac tumour, left-sided endocarditis and left-sided valvular prosthesis. Category II abnormalities were: depressed ejection fraction (EF),13 14 LV aneurysm,15 LV segmental wall motion abnormality,16 aortic stenosis17 and regurgitation18 (moderate and severe by colour Doppler), and mitral stenosis19 and regurgitation20 (moderate and severe by colour Doppler). Category III findings included: dilated left atrium (LA),21 22 LV hypertrophy (LVH),23 mitral annular calcification (MAC),24 Lambl’s excrescence25 and aortic atheroma.26
Outcomes
The outcomes of incident hospitalisation for recurrent ischaemic stroke and cardiac events were ascertained within the time frame of the day after AIS hospitalisation discharge to 1 year after discharge in the full cohort. We queried the Massachusetts General Hospital’s Research Patient Database Repository for discrete hospitalisations that occurred within the health system with a principal diagnoses of ischaemic stroke (ICD-9 434 .xx, 436 .xx; ICD-10 I63.3-I63.9), MI (ICD-9 410 .xx; ICD-10 I21.xx, I22.xx) and heart failure (ICD-9 428 .xx; ICD-10 I50.xx).27 We counted only the first incident hospitalisation for each of the individual outcomes of recurrent ischaemic stroke, MI and heart failure within 1 year after AIS discharge.
Statistical analysis
Comparison of TTE abnormalities in patients who had an ischaemic stroke across time
Statistical analyses were performed in SAS software V.9.4 (Cary, North Carolina, USA). Baseline demographic and clinical characteristics are presented as percentages and means as appropriate. Among patients with both TTEs prior to and during AIS admission, exact McNemar’s testing was used to determine whether there was a significant difference in the proportion of patients with each prespecified cardiac abnormality at the two time points. This test was selected due to the lack of independence between repeated measures within the same group of patients.28 29 Statistical significance was set at p<0.05. This test was also applied among patients with both an inpatient TTE and TTE >3 months after admission. Among patients with TTEs available prior to, during, and ≥3 months after admission, we compared the proportions of patients with each cardiac abnormality at each time point by Cochran’s Q test.
Logistic regression modelling
To identify predictors of Category I, II and II abnormalities detected on AIS admission TTE, multivariable logistic regression models were developed using clinical and imaging covariates available at the time of or soon after presentation including age, gender, race, prior medical comorbidities and medication use, NIHSS at presentation, and radiographic findings (cortical infarct location, infratentorial infarct location, and vessel stenosis or occlusion). We excluded patients with prior history of heart failure from this analysis since heart failure was one of the TTE outcomes of interest. Among patients without a history of heart failure (n=5228), we modelled the likelihood of observing any of the prespecified TTE findings. We also modelled the likelihood of having a TTE abnormality in each of the three categories with specific management implications. Parsimonious models were created by stepwise selection (p values of entry and exit: 0.05). These models were also generated in a subgroup of patients with no prior history of heart failure, mechanical heart valve or AF (n=4234) since there are well-defined management approaches with these diagnoses and AIS. We created a multivariable logistic regression model to identify independent predictors of having a new TTE finding if a prior TTE showed no abnormalities. Finally, we ascertained the odds of (1) Incident hospitalisation for recurrent ischaemic stroke, (2) MI, and (3) Heart failure within 1 year of the index AIS hospitalisation in all patients with AIS regardless of baseline heart failure status as a function of having a Category 1, II and III TTE abnormality detected by the AIS TTE by univariate logistic regression modelling.
Net reclassification improvement analysis
We sought to evaluate the additive value of Category I findings in predicting incident hospitalisation for recurrent ischaemic stroke within the 1 year follow-up period. We calculated the net reclassification index and its two-sided 95% CI to understand the incremental predictive capacity of Category I TTE biomarker data above the baseline characteristics collected during AIS admission.30 These characteristics were the following: age, sex, race, and history of prior stroke, HTN, HLD, diabetes, AF and heart failure.
Results
There were 5523 hospitalisations in the cohort (table 1). More than half were male, and the mean age of patients was 68.6 years. The majority of the cohort was Caucasian (86%) with HTN (68%), AF (20%), HLD (40%) and DM (23%). Average admission NIHSS was 8. Nearly 33% reported taking an antithrombotic (29% an antiplatelet, 4.9% an anticoagulant). Seventy-two per cent had cortical infarcts, 27% had infratentorial infarcts, and 30% had significant head or neck stenosis or occlusion of a head or neck artery. The accuracy of our automated method of radiology data extraction in a random sample of 100 selected for each variable was 98% for neuroanatomical location and 99% for vessel abnormality.
Characteristics of the study cohort
Nearly 81% of admission TTEs had at least one abnormality of interest. The most frequent admission TTE findings were: dilated LA (44%), MAC (37%), LVH (26%), aortic atheroma (17%), PFO (16%), segmental LV wall motion abnormality (14%), moderate or severe mitral regurgitation (11%), and EF ≤35% (7.4%). In the cohort without a prior history of heart failure, a total of 4157 out of 5228 (79.5%) admission TTEs demonstrated at least one abnormality. There were 981 (18.7%) admission TTEs with a Category I finding, 1711 (32.7%) with a Category II finding and 3806 (72.8%) with a Category III finding. Among patients with no history of heart failure, mechanical cardiac valve or AF (n=4234), there were 3227 admission TTEs with any prespecified abnormality (76.2%), 854 with a Category I abnormality (20.1%), 1062 with a Category II abnormality (25.1%) and 2642 with a Category III abnormality (62.4%).
Comparison of TTE abnormalities in patients who had a stroke across time
Among patients with TTEs both before and during AIS admission, the proportion of patients with the following abnormalities increased significantly on the subsequent TTE: PFOs (p<0.01), dilated left atria (p<0.01), LV thrombi (p=0.03), LVH (p=0.01), EF ≤15% and <35% (p<0.01 and p<0.01, respectively), Lambl’s excrescence (p<0.01), MAC (p=<0.01), aortic atheroma (p<0.01) and cardiac valvular prostheses (p<0.01) (table 2). Median time from prior TTE to the inpatient TTE was 539 days (IQR: 162–1317). Among those with an inpatient and follow-up TTE, there was an increase in the proportion of patients with: dilated LA (p<0.01), segmental LV wall motion abnormality (p=0.03), MAC (p<0.01), and moderate and severe mitral regurgitation (p<0.01).
Findings on TTE during inpatient hospitalisation for ischaemic stroke versus a most recent prior TTE (left) and inpatient TTE versus follow-up TTE (right)
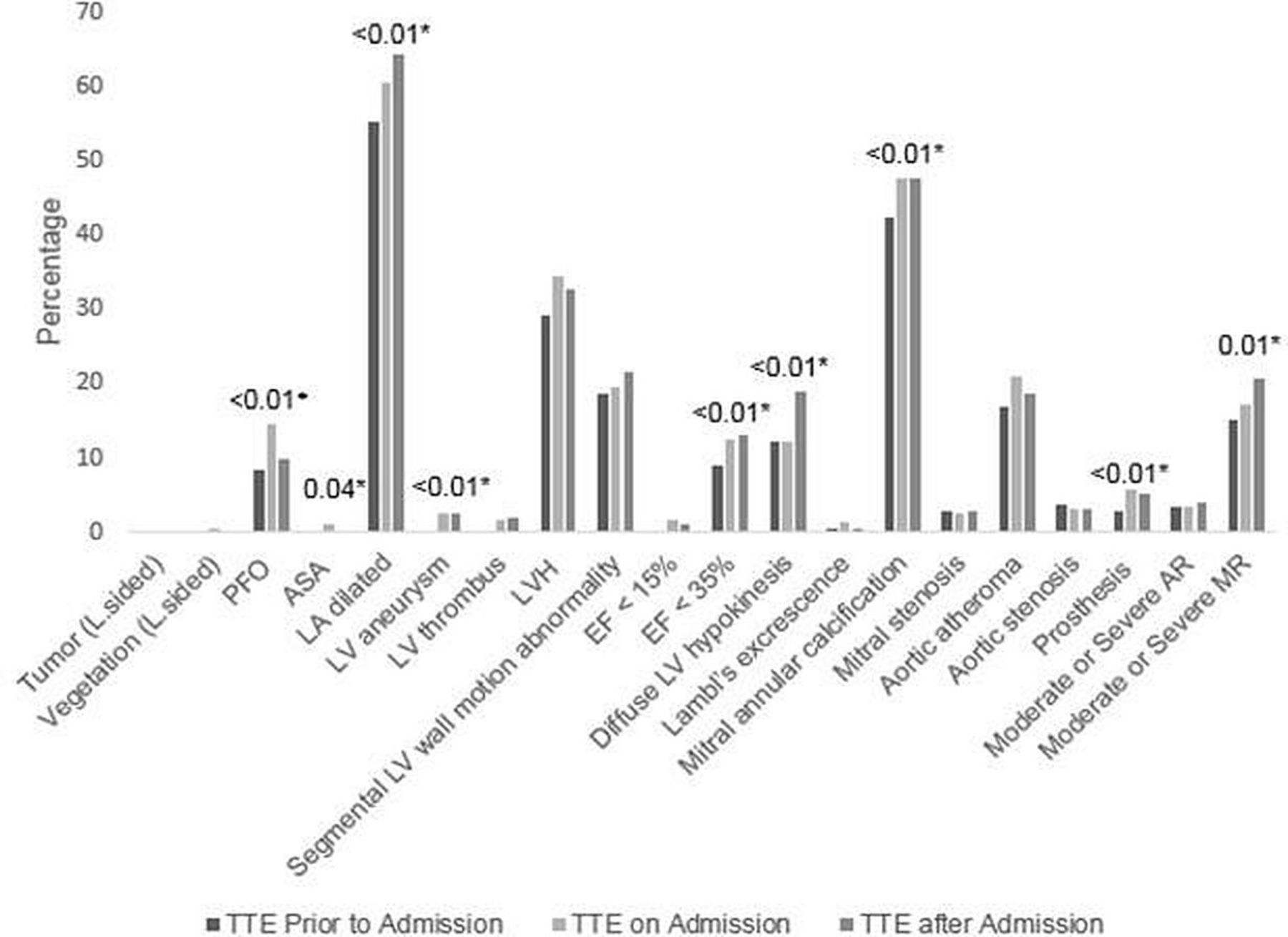
In the subgroup (n=373) with TTEs across all three time points (prior to AIS admission, during the inpatient AIS period and ≥3 months after the admission) (figure 1), higher proportions were noted with dilated LA (p<0.01), EF ≤35% (p<0.01), PFOs (p<0.01), atrial septal aneurysms (p=0.04), MAC (p<0.01), a new prosthetic valve (p<0.01), and moderate and severe mitral regurgitation (p=0.01) over time.

Cardiac abnormalities across serial transthoracic echocardiography (TTE). Percentages of patients with TTE abnormalities prior to ischaemic stroke admission, at the time of admission and after admission. (N=373). *Median time from first to the third TTE: 1094 days (IQR 559–1900). AR, aortic regurgitation; EF, ejection fraction; LV, left ventricular; MR, mitral regurgitation; PFO, patent foramen ovale.
Multivariable modelling
Table 3 presents independent, patient-level predictors of an abnormal TTE during admission in the cohort without a prior history of heart failure including older age (OR 2.01, 95% CI 1.73 to 2.34), CAD/prior MI (OR 3.44, 95% CI 2.64 to 4.47), AF (OR 3.15, 95% CI 2.40 to 4.14), diabetes (OR 1.28, 95% CI 1.06 to 1.54), HTN (OR 1.32, 95% CI 1.14 to 1.54), and patent head and neck vessels (OR 1.18, 95% CI 1.01 to 1.38) (c-statistic 0.71). There was a higher likelihood of a Category I finding among those who were younger, Caucasian, had no history of AF, HTN, or DM, had an infratentorial infarct, had a low severity stroke, and had patent head and neck vessels (c-statistic 0.68). The odds of having a Category II TTE abnormality were higher among patients who were older, had a history of CAD, AF, HTN, or PVD, had a higher NIHSS, and had patent head and neck vessel (c-statistic 0.73). Significant predictors of a Category III finding included older age, male sex, a history of CAD, AF, HTN, DM, or CKD, and a higher NIHSS.
Multivariable logistic regression models predicting an abnormal TTE finding (left), a Category I finding (left-centre), a Category II finding (right-centre) and a Category III finding (right) among those with no prestroke history of heart failure
Among patients with no history of heart failure, mechanical cardiac valve or AF (n=4234), older age, Caucasian race, history of CAD, HTN or DM, and patent head and neck vessels were patient-level risk factors for having any of the prespecified TTE abnormalities (c-statistic 0.68, table 4). Younger, Caucasian patients with no history of HTN, DM, or antiplatelet use, NIHSS <4, infratentorial infarct, and patent head and neck vessels were more likely to have a Category I finding (c-statistic 0.67). A Category II abnormality was associated with patients who were older, had a history of CAD and HTN, a higher NIHSS, a cortical infarct, and patent head and neck vessels (c-statistic 0.72). Older, male patients with a history of CAD, HTN or DM, and higher NIHSS were more likely to have a Category III finding (c-statistic 0.72).
Multivariable logistic regression models predicting an abnormal TTE finding (left), a Category I finding (left-centre), a Category II finding (right-centre) and a Category III finding (right) among those with no prestroke history of heart failure, mechanical heart valve or atrial fibrillation (n=4234)
We created a model predicting the odds of a new prespecified TTE finding (n=83) during AIS admission if a prior TTE in our system was unremarkable (n=891) (table 5). Older patients with CAD, PVD, CKD, no history of HLD and no known carotid disease were likely to develop a novel TTE finding at the time of AIS (c-statistic 0.71).
Multivariable logistic regression model predicting a new abnormal TTE finding (n=83) in those with a prior normal TTE (n=891)
There were a total of 124 hospitalisations for recurrent stroke, 21 hospitalisations for MI and 28 hospitalisation for heart failure within 1 year of the index AIS hospitalisation. In univariate logistic regression modelling of all patients with AIS, the odds of an incident hospitalisation for recurrent ischaemic stroke within 1 year of discharge from the index AIS hospitalisation was significantly higher among patients with a Category I finding detected by the AIS TTE versus patients without a Category I finding (OR 0.54, 95% CI 0.30 to 0.96, p=0.0347, table 6). There was no significant difference in hospitalisations for MI (OR 1.45, 95% CI 0.53 to 3.97, p=0.4701) or heart failure (OR 1.01, 95% CI 0.38 to 2.65, p=0.9895) by Category I status. The odds of a recurrent stroke hospitalisation within 1 year of AIS were similar by Category II status (OR 0.77, 95% CI 0.51 to 1.16), but the odds of hospitalisation for MI (OR 2.46, 95% CI 1.04 to 5.80) and heart failure (OR 5.62, 95% CI 2.47 to 12.79) within 1 year were significantly higher among patients with Category II findings. There was no association between the odds of hospitalisation for any of the three conditions as a function of Category III status.
Odds of hospitalisation for recurrent ischaemic stroke, myocardial infarction and heart failure as a function of TTE finding categories
There was significant net reclassification improvement with the additional input of Category I TTE data to baseline characteristics (net reclassification index 0.1563; 95% CI 0.0465 to 0.2661) for predicting recurrent ischaemic stroke hospitalisation. The addition of Category I TTE data to baseline characteristics compared with the model comprised of baseline characteristics alone resulted in 79% of events being correctly reclassified (p<0.001) and 63% of non-events being reclassified (p<0.001).
Discussion
Our study assesses TTE findings identified during an AIS hospitalisation. About 19% of studies demonstrated an abnormality associated with a high risk of cardioembolic stroke, 33% with an abnormality warranting cardiac management not specifically related to stroke and 72% with findings with no significant immediate implication but which may prompt further monitoring and long-term risk factor management to prevent a future cerebrovascular or cardiovascular event. Some findings were more frequently observed over time. Patient-level risk factors for an abnormal TTE include age, vascular risk factors, having cortical or infratentorial acute infarcts, and patent head and neck vessels. Only 9% of admission TTEs demonstrated a new abnormal finding compared with a prior TTE study. Older and unhealthier patients with no known carotid disease and a prior normal TTE have higher odds of a new TTE abnormality during AIS admission. Having a TTE finding detected at the time of AIS which has been associated with high stroke risk was associated with a significantly lower rate of ischaemic stroke hospitalisation within 1 year. Conversely, detection of a TTE feature associated with high risk of cardiac events was associated with a significantly elevated odds of hospitalisation for MI and heart failure within 1 year. There was no 1 year risk of stroke or cardiac events associated with TTE findings with no significant immediate clinical implication. Finally, there was significant incremental predictive value of Category I data above baseline demographic and clinical characteristics for 1 year recurrent ischaemic stroke hospitalisation risk. These findings confirm the important role of inpatient TTEs at the time of AIS admission particularly in patients with a high-risk profile to prompt interventions to prevent future cerebrovascular and cardiac events.
Two other studies have evaluated TTE findings in the AIS context. Abreu et al observed that 37% of patients with AIS had TTE findings that would warrant anticoagulation3 while Fralick et al noted that only 14% of TTEs in patients with AIS identified clinically actionable findings for secondary stroke prevention.31 These percentages lie within the range of the prevalences of potential cardioembolic sources identified by TTE in our study. Our study, however, also uniquely describes abnormalities associated with both future neurological and cardiac events. Given the high proportions of AIS TTEs with abnormalities in the three prespecified categories in our study, a TTE during the AIS encounter may be a pivotal screening and diagnostic opportunity to promote brain and heart health. For instance, a new diagnosis of low EF merits may prompt not only anticoagulation for secondary stroke prevention but also cardiology consultation and prescription of evidence-based cardioprotective medications which may not be administered as first-line therapy for routine management by stroke care providers. A concomitant finding of LVH or aortic atheroma may also prompt more aggressive risk factor management to promote the health of both vascular beds. As such, the diagnostic implications from a TTE during an AIS admission may have significant immediate and downstream effects.
Our study uniquely explores TTE findings during AIS hospitalisation and their association with future stroke and cardiovascular events within 1 year of the index AIS. The ascertainment by TTE of findings linked with high stroke risk was associated with significantly lower odds of hospitalisation for ischaemic stroke within a year. The addition of Category I TTE biomarker data significantly improved the predictive capacity for recurrent ischaemic stroke beyond traditional vascular risk factors. These echocardiographic features have been designated as high risk in the stroke literature and there are clear evidence-based secondary stroke prevention treatment algorithms. The identification of any of these stroke risk related TTE abnormalities during AIS admission likely prompted targeted stroke guideline-directed intervention to neutralise effectively the risk of future stroke from that specific source such as treatment of endocarditis with antibiotics or initiation of anticoagulation for an LV thrombus.
Among patients with TTE findings associated with high risk for a cardiac event, there was no increased odds of future stroke events, but there was a two times and five times higher risk of MI and heart failure, respectively. There may be two explanations for this observation. First, the risk of a cardiac event among patients with these TTE findings is elevated by definition and may reflect the natural course of cardiovascular disease. While this may be the case, there were multiple guideline-directed medical therapies available to modify the risk of cardiovascular events during this epoch that may not be in the toolkit of stroke providers. It is possible that under-recognition of the clinical significance of Category II findings may result in underutilisation of guideline-directed medical therapies, rendering the course of their sequela of cardiovascular outcomes unmitigated.
While the rates of recurrent hospitalisation events were low at 3.1%, importantly if considered solely from a payer’s standpoint, the estimated cost of a TTE only (estimated at $634 per study) in patients with a Category I or II abnormality detected during AIS admission in our cohort was $1585 000 while the estimated cost of hospitalisation for all three events within 1 year of the AIS was $2923 564.32 33 In contrast, the estimated total cost of ubiquitously obtaining TTEs in all patients with AIS in our cohort would have been $3501 582. These findings suggest that obtaining TTEs in patients with AIS particularly with a high pretest probability of having a Category I or II finding may be of clinical utility without compromising resource stewardship.
The use of a repeat TTE during AIS admission is often questioned when there is an existing recent TTE available. Our study demonstrates that among patients with a prior normal TTE who are admitted for AIS, nearly 9% have an abnormal finding on the TTE during admission. Predictors of a novel TTE finding include vascular comorbidities and no history of carotid disease. One explanation of this paradoxical finding is that among those with known carotid disease, the causative aetiology may be more likely large artery atherosclerosis rather than cardioembolism from a new cardiac lesion that developed in the interim. While the rareness of a new finding suggests a potentially limited role for a repeat TTE at the time of stroke if a prior TTE study is available and carotid disease is present, further study is needed to validate this observation.
We noted several patterns in our longitudinal analyses. Vascular risk factors were independent predictors of new TTE findings. LA dilation was one of the most common Category III TTE abnormalities and the proportion of patients with LA dilation increased with time. A link between LA dilation prevalence and vascular risk factors has been noted in prior studies.34 35 The observed progression of LA dilation in patients who had an ischaemic stroke is hypothesis-generating in terms of the temporal relationship linking atrial cardiopathy, AF and ischaemic stroke. There was a greater proportion of patients with depressed EF and wall motion abnormality over time, suggesting a need to consider screening high-risk patients to prevent further cardiovascular events. Finally, follow-up TTEs were more likely to detect a new diagnosis of moderate or severe mitral regurgitation. The association between severe mitral regurgitation and mortality if untreated can be up to 50% compared with 14% with valve repair or replacement, highlighting the importance of its timely detection and management.20
There are several limitations of our study. One consideration is the unknown generalisability of our results to patients in other geographical regions. Survival and detection biases are inherent in a retrospective study. We attempted to minimise detection bias by only including patients with TTE available at each of the time points of interest, however this approach can be subject to confounding by indication. The indications for the TTE studies were not precisely known and may explain the higher proportion of patients observed with a PFO during the inpatient AIS admission study compared with a prior TTE due to differences in ascertainment techniques used for specific indications. There is likely variability by sonographers and echocardiographers in the threshold for discerning and reporting a TTE abnormality, depending on indication for the TTE at the time it was ordered. Outcomes were ascertained by administrative billing codes which have variable sensitivity and specificity. There are also presumably unmeasured confounders at the patient level including the prevalence of medical comorbidities at the time of a prior and follow-up TTE. The TTE categories in this study are broad; further investigation is necessary to pinpoint specific TTE findings that can be implicated with outcomes.
Summary
We observe a high prevalence of prespecified cardiac abnormalities detected by echocardiogram at the time of acute stroke hospitalisation associated with ischaemic stroke and cardiovascular event risk. The proportion of patients who had a stroke with certain abnormalities increases with time. We identify predictors of specific TTE abnormalities at the time of admission and having a new specific TTE abnormality if a prior TTE was normal. Finally, the presence of a high stroke risk TTE abnormality at the time of ischaemic stroke hospitalisation was associated with a significantly reduced odds of recurrent ischaemic stroke upto 1 year after the index ischaemic stroke, while a high cardiac risk TTE abnormality was associated with significantly higher odds of MI and heart failure hospitalisations. The addition of Category I TTE biomarker data significantly improved prediction of recurrent ischaemic stroke risk. These findings demonstrate utility of TTE as a diagnostic test performed during the AIS admission, particularly in patients with a high pretest probability of TTE findings associated with high risk of stroke and cardiac events. Further study is necessary to determine criteria for appropriate utilisation of TTE during AIS hospitalisation to inform our current standard of care.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request by investigators.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Massachusetts General Hospital Institutional Review Board. The IRB waived the need to obtain informed consent.
Acknowledgments
The authors thank the staff who have participated in the development and maintenance of their institutional Get-With-The-Guidelines data repository.
Footnotes
Twitter @braindoc_mgh
Contributors RS's role was study conception and design, data analysis and manuscript writing.
Funding There was no specific funding source for this study, but effort by Dr Sharma and Dr Schwamm (Principal Investigator for the StrokeNet Northeast Regional Coordinating Centre) was supported, in part, by funding from the NINDS StrokeNet Network (NINDS U10 NS086729).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References




{kind=link}