

Abstract
Background Surgical treatment of posterior inferior cerebellar artery (PICA) aneurysms is challenging because many are nonsaccular and atherosclerotic. We report our tailored approach to PICA aneurysms, which is based on angioarchitecture supplemented by high-resolution vessel wall MRI (HR-VW MRI) findings.
Methods From March 2010 to September 2020, 27 patients with 29 PICA aneurysms underwent surgical treatment in our institution. Since October 2016, HR-VW MRI has been used for aneurysmal wall assessment. Clinical characteristics, radiological data and surgical outcomes were analysed.
Results Nineteen proximal PICA aneurysms (vertebral artery (VA), P1, P2 and P3) were treated using the far-lateral approach. Ten distal PICA aneurysms (P4, P5) were treated using the suboccipital midline approach. Direct clipping or clip reconstruction was achieved in 19 aneurysms. Ten were trapped in conjunction with extracranial–intracranial or intracranial–intracranial bypass, including three occipital artery-PICA reimplantations, three PICA-VA reimplantations, two PICA-PICA side-to-side anastomoses, one PICA-PICA reimplantation and one PICA-PICA reanastomosis. All aneurysms were eventually completely obliterated and all bypasses remained patent. At the last follow-up, 26 patients (96.2%) achieved a good outcome (modified Rankin Scale score <3). Eight patients underwent HR-VW MRI. Among these, the six aneurysms with focal wall enhancement required bypass and the two with negative enhancement were successfully clipped.
Conclusion PICA aneurysms have a higher frequency of complex features such as large or giant size and fusiform or dissecting morphology. Favourable outcomes were achieved with individualised microsurgical strategies based on angioarchitecture. HR-VW MRI may be used as a promising technique to predict aneurysmal atherosclerosis.
Key messages
What is already known on this topic
Posterior inferior cerebellar artery (PICA) aneurysms have a higher frequency of complex features, and surgical treatment is still challenging because of anatomic variability, lower cranial nerves interference, diverse aneurysmal morphology and atherosclerosis.
What this study adds
Surgical strategies for treatment of PICA aneurysms consists of aneurysm clipping and various bypass modalities, such as occipital artery-PICA, PICA-vertebral artery and PICA-PICA bypass. Favorable outcome could be achieved if a PICA aneurysm is treated with proper surgical strategy. The selection of surgical strategies is mainly based on the assessment of aneurysmal morphology and enhancement pattern on high-resolution vessel wall MRI (HR-VW MRI).
How this study might affect research, practice or policy
The aneurysmal enhancement patterns on HR-VW MRI may be used as a promising imaging biomarker to predict atherosclerosis of PICA aneurysms and help surgical strategy selection.
Introduction
Posterior inferior cerebellar artery (PICA) aneurysms account for 3%–4% of all cerebral aneurysms.1 Compared with aneurysms in other locations, PICA aneurysms are more likely to be fusiform. After rupture, they are associated with higher incidence of lower cranial nerve dysfunction and tracheostomy/percutaneous endoscopic gastrostomy placement.2–4 Although endovascular treatment can allow PICA preservation, selective aneurysm coiling may not be possible in up to 79% of fusiform aneurysms.5 Stent-assisted coiling may preserve the circulation but can place patients at risk of unpredictable rebleeding.6 Furthermore, distal PICA segment aneurysms can be difficult to access via an endovascular approach and direct PICA occlusion may result in infarction and death.7
Therefore, microsurgical treatment may be required for the treatment of complex PICA aneurysms. This approach can be challenging because of anatomic variability, interference of lower cranial nerves, diverse aneurysmal morphology and size, and presence of atherosclerosis, calcification, and intraluminal thrombosis, all of which must be assessed preoperatively.4 8–16 However, previously developed angioarchitecture-based surgical algorithms do not take aneurysmal wall structure into account despite its impact on treatment selection. High-resolution vessel wall MRI (HR-VW MRI) has shown promise in identifying aneurysmal wall inflammatory reaction and atherosclerosis and may be useful in surgical planning.17 Therefore, We have developed tailored operative techniques for PICA aneurysms that are based on digital subtraction angiography (DSA) angioarchitecture characteristics, including morphology, location and wall structure.12 14 18 19 This study describes our evaluation process, surgical strategy and outcomes.
Methods
Complex PICA aneurysms
The PICA is divided into five segments: anterior medullary (P1), lateral medullary (P2), tonsillomedullary (P3), telovelotonsillar (P4) and cortical (P5).19–23 Aneurysms located on any of these five segments are considered true PICA aneurysms. Most arise at the vertebral artery (VA)-PICA junction.18 24 Those located at the VA-PICA junction and on segments P1–P3 are classified as proximal. P4 and P5 aneurysms are classified as distal and share similar surgical strategies.18–24
A complex PICA aneurysm that cannot be secured by simple coiling or clipping may have one or more of the following features: giant (≥25 mm) or large (10–25 mm) size, atherosclerotic wall structure, dissecting or fusiform morphology, wide neck, and recurrence after previous coiling or clipping.14 21 25–31 Since October 2016, we have used HR-VW MRI in the preoperative evaluation of unruptured PICA aneurysms. The imaging was acquired using fat-suppressed three-dimensional fast spin-echo (FSE) CUBE T1-weighted sequences. Wall enhancement on gadolinium-enhanced imaging was classified as negative (no wall enhancement) or focal wall enhancement (FWE, strong enhancement of only a part of the wall), as previously described.17 FWE has been verified as a promising radiological marker of atherosclerotic plaque formation.17 We considered that FWE indicated a complex aneurysm since atherosclerotic plaque is often considered a feature of complex aneurysms. Bacterial, iatrogenic and traumatic aneurysms and those arising from an anterior inferior cerebellar artery-PICA variant were excluded.
Surgical strategy
Our PICA aneurysm surgical strategyis illustrated in figure 1. Angioarchitecture was carefully evaluated before surgery with DSA. For proximal PICA aneurysms, the far-lateral approach was used to provide wide exposure of the VA and PICA branch point, which enables clear identification and dissection of the aneurysm and perforators. The dentate ligament was transected to promote PICA and brainstem-spinal cord junction mobility, reducing the incidence of lower cranial nerve injury. The craniotomy was extended across the midline for distal PICA exposure if a PICA-PICA bypass was needed.14 21 25–31 For distal PICA aneurysms, a suboccipital midline approach was used. The aneurysm was exposed by starting dissection at P3 and proceeding distally. If the aneurysm was hidden deep in a cerebellar fissure, neuronavigation was used for localisation.14 21 25–31

Schematic showing the strategy for surgical treatment of posterior inferior cerebellar artery (PICA) aneurysms based on angioarchitecture and aneurysmal wall assessment. DSA, digital subtraction angiography; EC-IC, extracranial–intracranial; IC-IC, intracranial–intracranial; P1, anterior medullary segment of the PICA; P2, lateral medullary segment of the PICA; P3, tonsillomedullary segment of the PICA; P4, telovelotonsillar segment of the PICA; P5, cortical segment of the PICA; VA, vertebral artery.
After aneurysm exposure and inspection, direct clipping or clip reconstruction was preferentially performed. If the aneurysm was unclippable due to complexity, bypass and trapping was considered, especially for proximal aneurysms associated with critical brainstem perforators.1 5 9 11–14 18 20 22–24 26 29 32–38 We preferred intracranial–intracranial (IC-IC) bypass over extracranial–intracranial (EC-IC) bypass when possible. PICA-PICA side-to-side bypass was the first choice for proximal aneurysms if possible. If not, ipsilateral PICA (P3) to contralateral (P3) reimplantation was attempted (figure 2). Alternatively, PICA-VA end-to-side reimplantation (figure 3) was performed if the PICA and intracranial VA had sufficient length for anastomosis without critical perforators or occipital artery (OA)-PICA (P3) end-to-side bypass (figure 4). End-to-end reanstomosis was seldom performed because of its high incidence of thrombosis and stenosis. Rarely, if a perforator arose from the aneurysm sac, test occlusion of the perforator was performed for 30 min using electrophysiologic monitoring; if responses did not significantly change, the perforator was sacrificed. Unlike proximal aneurysms, simple PICA occlusion can be safely performed for distal onebecause of the abundant collateral circulation and the lack of brainstem perforators.13 Aneurysm obliteration and bypass patency were analysed intraoperatively using indocyanine green videoangiography, Doppler ultrasound and DSA.

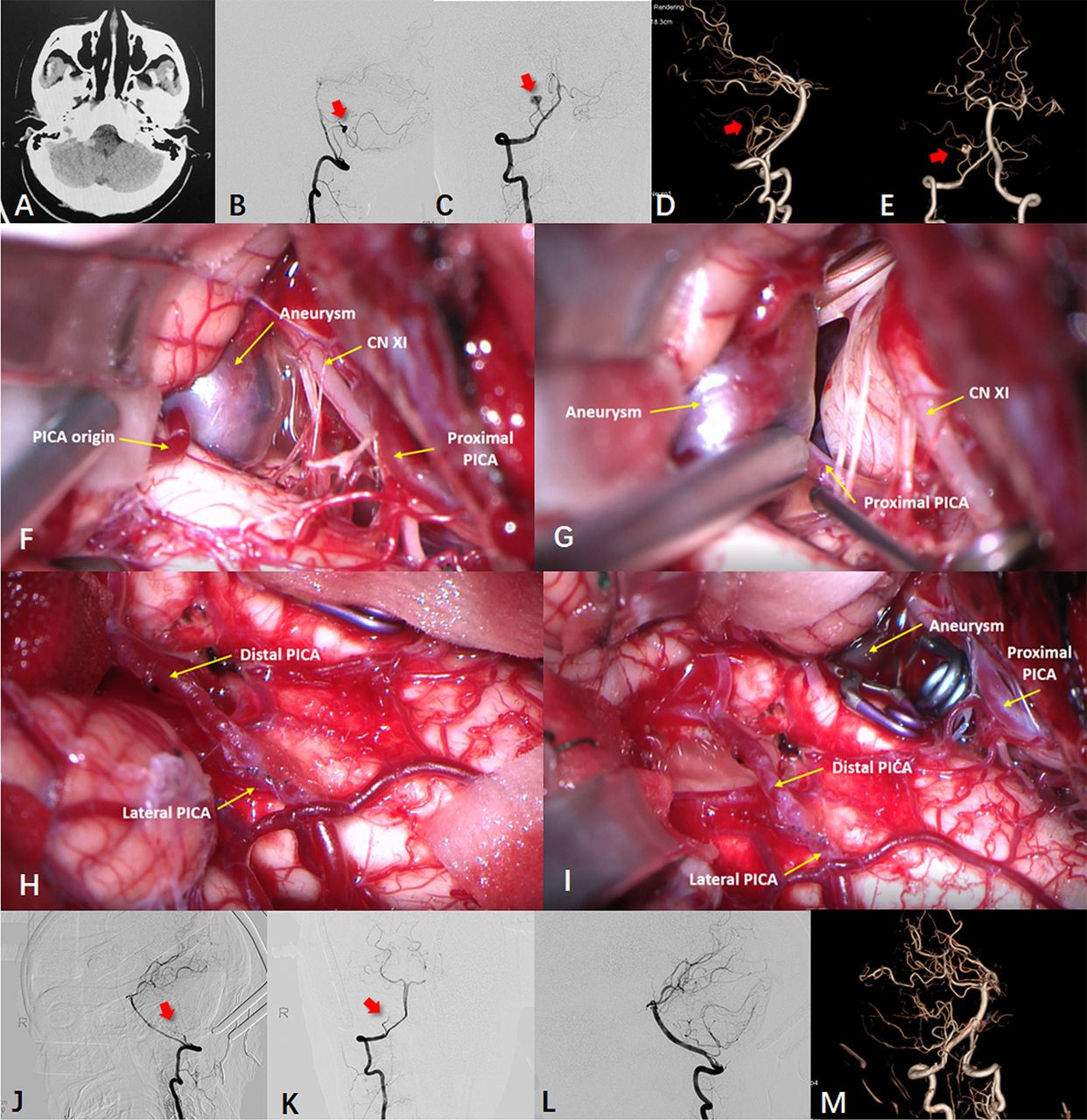
Case 20: P3-P3 reimplantation. (A) A young female with headache and dizziness for 5 days showed a high-density lesion of the right lateral medulla on CT. (B–E) Digital subtraction angiography (DSA) showed a right P3 segment posterior inferior cerebellar artery (PICA) dissecting aneurysm (red arrows). (F–I) Using the suboccipital midline approach, the aneurysm was exposed adjacent to cranial nerves (CN) XI and XII. After temporary clipping of the proximal PICA, the aneurysm was trapped by clipping the proximal and distal PICA. A contralateral P3-ipsilateral P3 end-to-side bypass was performed for vascular reconstruction. (J–M) DSA showed aneurysm obliteration (red arrows) and bypass patency.

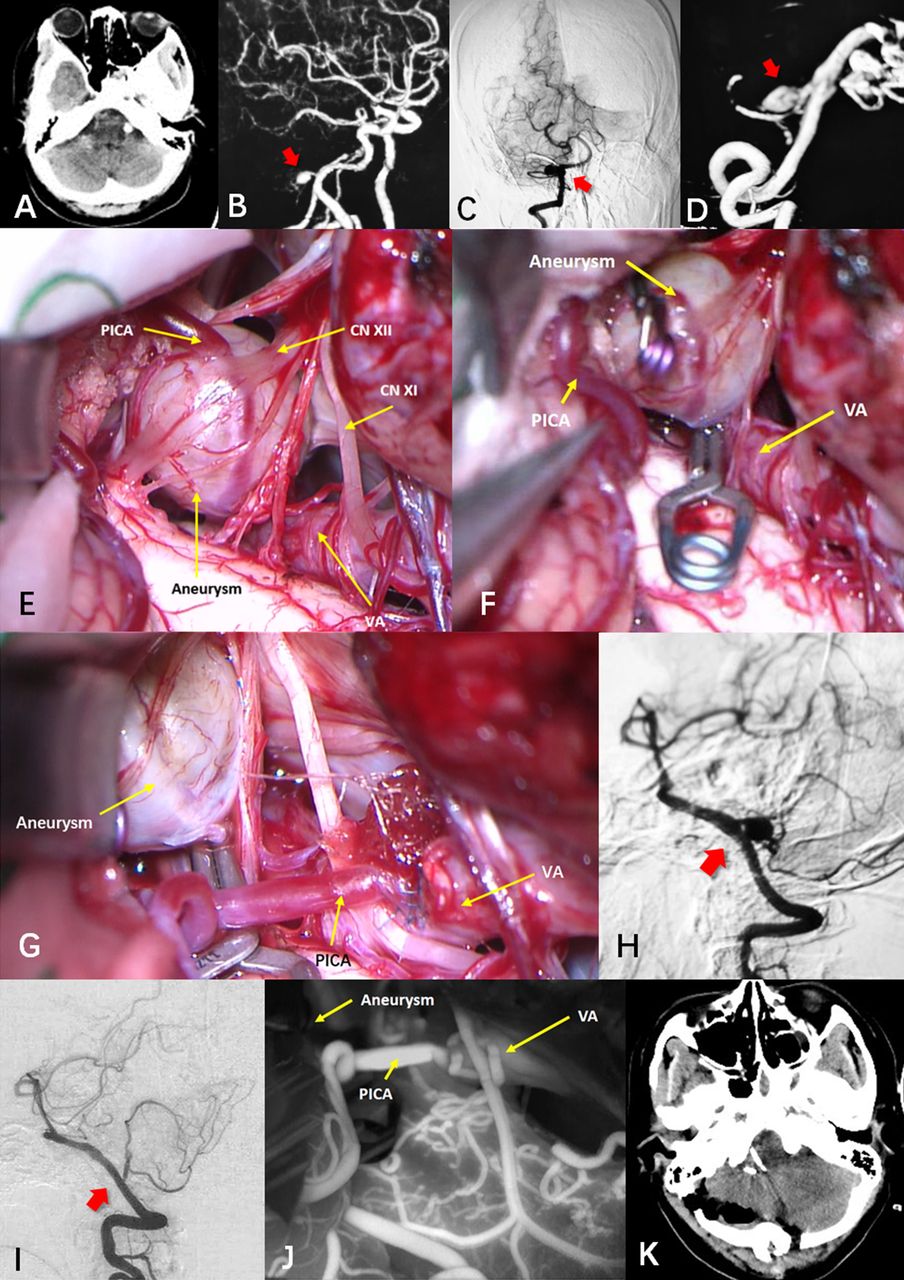
Case 21: posterior inferior cerebellar artery (PICA)-vertebral artery (VA) reimplantation. (A) A mid-aged female underwent CT to evaluate headache. A high-density lesion of the right lateral medulla was visualised. (B–D) MR angiography and digital subtraction angiography (DSA) showed a wide-necked right P1 saccular aneurysm (red arrow). (E–G) The aneurysm was saccular, contained plaques, and was located beneath cranial nerves (CN) XI and XII. Using the right far-lateral approach, the aneurysm was trapped through clipping of the proximal and distal pica and vascular reconstruction was performed using a PICA-VA bypass. (H) DSA before surgery showed the aneurysm (red arrow). (I) DSA after surgery confirmed aneurysm obliteration (red arrow) with bypass patency. (J) intraoperative indocyanine green angiography showed aneurysm obliteration with bypass patency. (K) Postoperative CT showed expected findings and NO infarction.

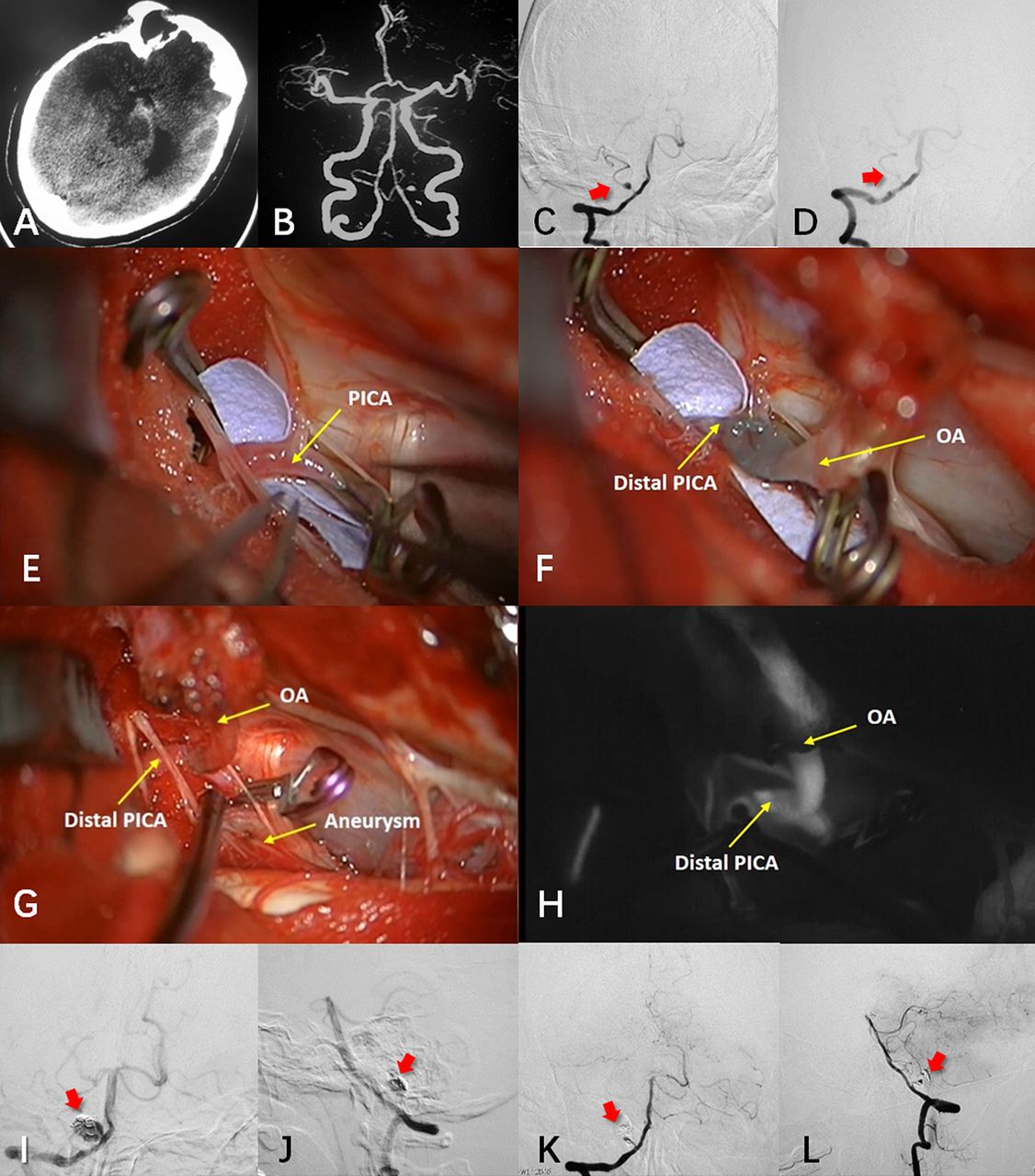
Case 18: occipital artery (OA)- posterior inferior cerebellar artery (PICA) bypass. (A, B) A mid-aged woman presented with aneurysmal subarachnoid haemorrhage due to rupture of a proximal right P2 segment aneurysm. (C) Digital subtraction angiography (DSA) at presentation showed the aneurysm (red arrow), which was coiled. (D) Post-coiling DSA showed complete embolisation (red arrow), but 6 months later, the aneurysm recurred. (E–G) Using the far-lateral approach, the aneurysm was exposed and trapped by clipping the distal PICA and vascular reconstruction was performed using OA-PICA end-to-side bypass. (H) Intraoperative indocyanine angiography showed aneurysm obliteration and bypass patency. (I–J) Preoperative DSA showed the recurrent pica aneurysm (red arrows). (K–L) Postoperative DSA showed aneurysm obliteration (red arrows) with bypass patency.
Patients
From March 2010 to September 2020, 45 consecutive patients with PICA aneurysm were treated in our institution. Among them, 27 patients treated surgically with 29 PICA aneurysms were enrolled in this study. Clinical data regarding age, sex, symptoms, radiological imaging, surgical complications and modified Rankin Scale (mRS) score outcomes were prospectively collected.
Statistical methods
Statistical analyses were performed using SPSS software V.20.0 (IBM). The independent Student’s t-test was used to compare continuous data. Fisher’s test and the χ2 test were used to compare categorical data. A p<0.05 was considered significant.
Results
Patient characteristics
Patient characteristics are shown in table 1 (for detailed information, please see online supplemental table). The mean patient age was 49.8±11.9 years (range 29–67). Nineteen patients were female and eight were male. The most common symptoms were headache in 16 patients (59.3%), dizziness in 10 (37.0%), unconsciousness in 7 (25.9%) and focal neurological deficit in 3 (11.1%). Thirteen patients (48.1%) presented with aneurysmal subarachnoid haemorrhage. The Hunt-Hess grade was I in five patients (38.5%), II in three patients (23.1%), III in four patients (30.8%) and IV in one patient (7.7%). Sixteen patients (59.3%) underwent surgery in the hybrid operating room of our hospital.
Supplementary data
Patient characteristics
Twenty-five patients (92.6%) had a single PICA aneurysm and 2 (cases 9 and 14) had multiple PICA aneurysms. Case 9 had a P3 and a P4 segment aneurysm. Case 14 had 5 PICA aneurysms, including 3 P2 segment aneurysms which were coiled first, and 2 P5 segment aneurysms which were surgically clipped (online supplemental figure 1).Two patients (cases 5 and 17) had a single PICA aneurysm and a concomitant internal carotid artery ophthalmic segment aneurysm that was coiled before PICA aneurysm clipping. Case four harboured a concomitant cerebellar arteriovenous malformation unrelated to the aneurysm.
Supplementary data
PICA aneurysm features and surgical strategy
Twenty-nine PICA aneurysms were treated surgically. Among these, 15 were on the left (51.7%), and 14 on the right (48.3%). Nineteen were proximal (5 VA-PICA, 6 P1, 5 P2, 3 P3) and 10 were distal (4 P4, 6 P5). PICA aneurysm features and microsurgical strategies are summarised in table 2. Nineteen aneurysms were saccular (mean size 8.6±2.9 mm (range, 4.0–16.0)), five were fusiform (mean size 18.0±4.3 mm (range, 11.0–22.0)) and five were dissecting (mean size10.2±4.7 mm (range, 4.0–15.0)). Cases 18 and 24 presented with a recurrent saccular and a recurrent fusiform aneurysm after coiling, respectively. Eleven patients (37.9%) had a large aneurysm (diameter 10–25 mm) and 2 (6.9%) had a giant aneurysm (diameter ≥25 mm).
Pica aneurysm features and microsurgical strategies (n=29)
All 10 distal aneurysms were treated by direct clipping (nine saccular aneurysms) or trapping (one fusiform aneurysm). Among the 19 proximal aneurysms, 9 (47.4%) were treated by clipping and 10 (52.6%) by trapping combined with bypass (7 IC-IC and 3 EC-IC, table 2, figure 1).
Surgical complications and outcomes
Complete aneurysm obliteration was observed in 25 patients (92.6%). The other two patients (cases 18 and 27, 7.4%) exhibited near-complete obliteration that later thrombosed completely. All patients were interviewed at follow-up with a mean follow-up period of 59.0±42.7 months. Postoperative transient lower cranial nerve dysfunction (cough and hoarseness) was observed in one patient with a P1 aneurysm who underwent PICA-VA reimplantation (case 21). No ischaemic complications were observed. At the last follow-up, 26 patients (96.2%) achieved a good outcome (mRS score <3). Compared with before surgery, mRS score was worse at last follow-up in only one patient (case 21, figure 3); the other 26 had improved (n=21, 77.8%) or stable (n=5, 18.5%) scores (table 2). All 10 patients who underwent bypass showed angiographic bypass patency. No aneurysm recurrences were observed.
Relationship between aneurysmal wall enhancement and surgical strategy
Because of the rarity of the PICA aneurysms, only eight patients with a single proximal unruptured PICA aneurysm were scanned by HR-VW MRI since October 2016 as a pilot study. Mean aneurysm size was larger as measured by HR-VW MRI than as measured by DSA with significant difference (15.8±10.9 mm vs 17.7±11.2 mm; p=0.0023). Wall enhancement on HR-VW MRI was negative in two aneurysms and FWE in six, and the latter tended to have a larger size and morphologic characteristics unfavourable for clipping (66.7% were fusiform or dissecting). We selected clipping as the primary strategy in the two aneurysms with negative wall enhancement and planned bypass with aneurysm trapping in the six aneurysms (two PICA-PICA side to side, two PICA-VA and two OA-PICA; table 3) that demonstrated FWE because of atherosclerotic plaque and calcification. The intraoperative surgical strategies were consistent with the preoperative strategies selected based on aneurysm angioarchitecture and wall assessment. Figure 5 illustrates two typical cases.
Aneurysm wall assessment and surgical strategies

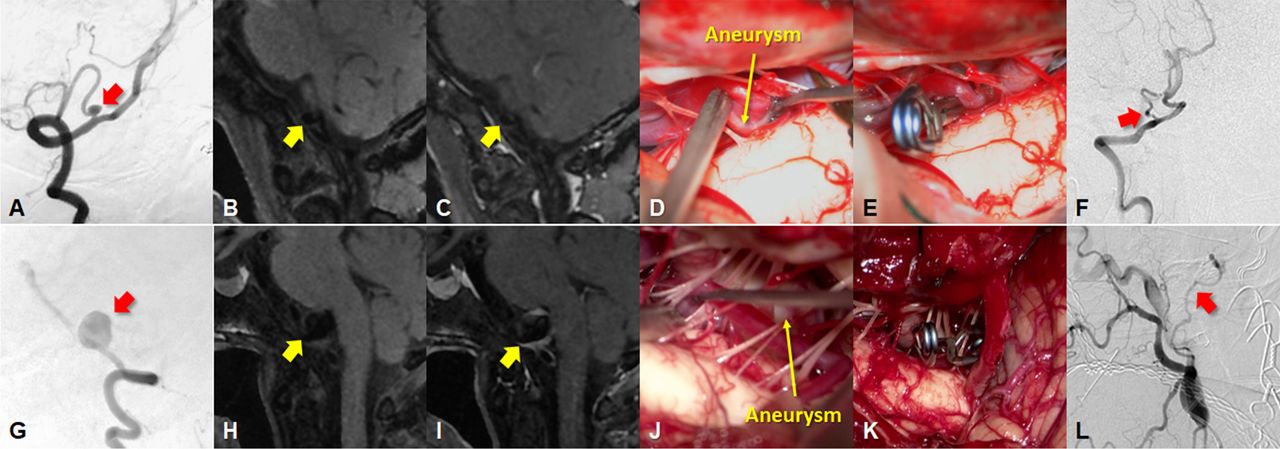
Wall assessment in determining surgical strategy for posterior inferior cerebellar artery (PICA) aneurysms: two typical cases (case 17, (A–F); case 16, (G–L): A: A 5.0 mm saccular right P1 aneurysm (red arrow) was detected using digital subtraction angiography (DSA). (B–C) Wall enhancement was negative (yellow arrows) on high-resolution vessel wall MRI (HR-VW MRI). (D) Intraoperatively, the aneurysm was saccular without plaque. (E) Using the far-lateral approach, the aneurysm neck was exposed and clipped. (F) Postoperative DSA confirmed aneurysm obliteration. G: A 15.7 mm P1 aneurysm involving the vertebral artery (VA) (red arrow) was detected using DSA. (H, I) Focal wall enhancement (yellow arrows) was present on HR-VW MRI. (J) Intraoperative observation revealed a dissecting aneurysm containing plaque. (K) Using the far-lateral approach, the aneurysm was trapped with clipping of the proximal and distal VA and PICA origin; occipital artery-PICA bypass was performed for vascular reconstruction. (L) Postoperative DSA showed aneurysm obliteration with bypass patency (red arrow).
Discussion
Aneurysmal wall assessments in the prediction of the surgical strategy
Surgical treatment of PICA aneurysms can achieve good results (tables 1 and 2) and the individualised surgical strategy varies according to the aneurysm’s segmental location and morphology (figure 1).14 16 18 32 39 However, although DSA remains the gold standard for aneurysm diagnosis and angioarchitecture assessment, it does not provide the aneurysmal wall structure data that HR-VW MRI does.17 We found a significant difference between DSA and HR-VW MRI aneurysm size measurements, with MRI arriving at a larger size. For aneurysms with FWE, bypass surgery should be considered and prepared for as there is a high possibility that atherosclerotic plaque will hinder clipping.17 40 This finding has encouraged us to include HR-VW MRI in future surgical planning. In our study, the intraoperative surgical strategies were consistent with preoperative assessment (table 3, figure 5).
Bypass surgery for pica aneurysms
Although clipping is generally considered the first option, this may be difficult for PICA aneurysms because of complex morphology. Bypass surgery is an important technique, especially for proximal aneurysms (figure 1). IC-IC bypass was our preferred technique because of its lower risk of cerebrospinal fluid leak and no need for graft harvesting. PICA-PICA bypass was preferred because the distal PICA tolerates prolonged temporary occlusion. If the contralateral PICA is not close enough for bypass, we have successfully transected the ipsilateral P3 distal to the aneurysm and anastomosed it to the contralateral P3 in an end-to-side fashion with a favourable outcome (case 20, figure 2). Moreover, if the VA-PICA junctionis in a high position, PICA-VA reimplantation can be achieved instead of PICA-PICA bypass (figure 3). The collateral perfusion of the contralateral VA is usually sufficient, so ischaemic risk during VA temporary occlusion is low. However, the lower cranial nerves may be closely related to the VA and hinder the operation (case 21). Aneurysm resection and PICA-PICA end-to-end reanastomosis could be attempted if the remaining parent PICA is long enough, but with a high risk of occlusion. Therefore, OA-PICA bypass, a moderate-flow EC-IC bypass, was considered the last resort if IC-IC bypass was difficult (figure 4).
Limitations
Since PICA aneurysms are rare, the number of enrolled patients was small and bias may have been introduced. Current HR-VW MRI research is limited and HR-VW MRI resolution is not high enough to determine the exact distribution of the atherosclerosis. The value of HR-VW MRI may be less applicable and more ambiguous in ruptured aneurysms than unruptured aneurysms. The HR-VW MRI concept for making surgical decisions is still speculative and in need of further research. Nonetheless, we believe that future developments in HR-VW MRI aneurysm assessment will contribute to advances in surgical treatment.
Conclusion
PICA aneurysms have a high frequency of complex features and require tailored surgical strategies. Surgical modalities included direct clipping, clip reconstruction, trapping with bypass surgery. Aneurysmal wall enhancement patterns on HR-VW MRI may assist with surgical planning. We recommend bypass surgery for aneurysms showing FWE. Favourable outcomes were achieved with individualised microsurgical strategies.
Data availability statement
Data are available on reasonable request. Individual participant data will be available. Individual participant data that underlie the results reported in this article, after deidentification (text, tables, figures and appendices) will be shared. Other documents including study protocol, statistical analysis plan will be available immediately following publication with no end date to researchers who provide a methodologically sound proposal. The documents were available to achieve aims in the approved proposal. Proposals should be directed to drzhuwei@fudan.edu.cn. To gain access, data requestors will need to sign a data access agreement.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by Huashan Hospital Institutional Review Board (HIRB), Fudan University, Shanghai, China. The ID is KY2015-256. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank Jianbin Shi for brain imaging processing, Geng Xu for intraoperative electrophysiological monitoring support.
Footnotes
ZY and JS contributed equally.
Contributors ZY: conceptualisation, data curation, methodology, software, formal analysis, visualisation, writing-original draft preparation. JS: conceptualisation, methodology, validation, data curation, formal analysis, visualisation, writing-reviewing and editing, funding acquisition, supervision. KQ: visualisation, data curation, software. PeilL: visualisation, data curation. QA: visualisation, data curation. YS: software, validation. PeixL: software, data curation. GY: validation, data curation. YT: software, validation. LZ: writing- reviewing and editing, project administration. WZ: conceptualisation, Writing-reviewing and editing, supervision, project administration, funding acquisition, responsible for the overall content as the guarantor
Funding This study was supported by the Outstanding Academic Leaders Program of Shanghai Municipal Commission of Health and Family Planning (No. 2017BR006 to WZ) ,the Shanghai Rising-Star Program (No. 18QA1400900 to JS.) and Shanghai Sailing Promgram (No.22YF1404500 to ZY).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}