

Article Figures & Data
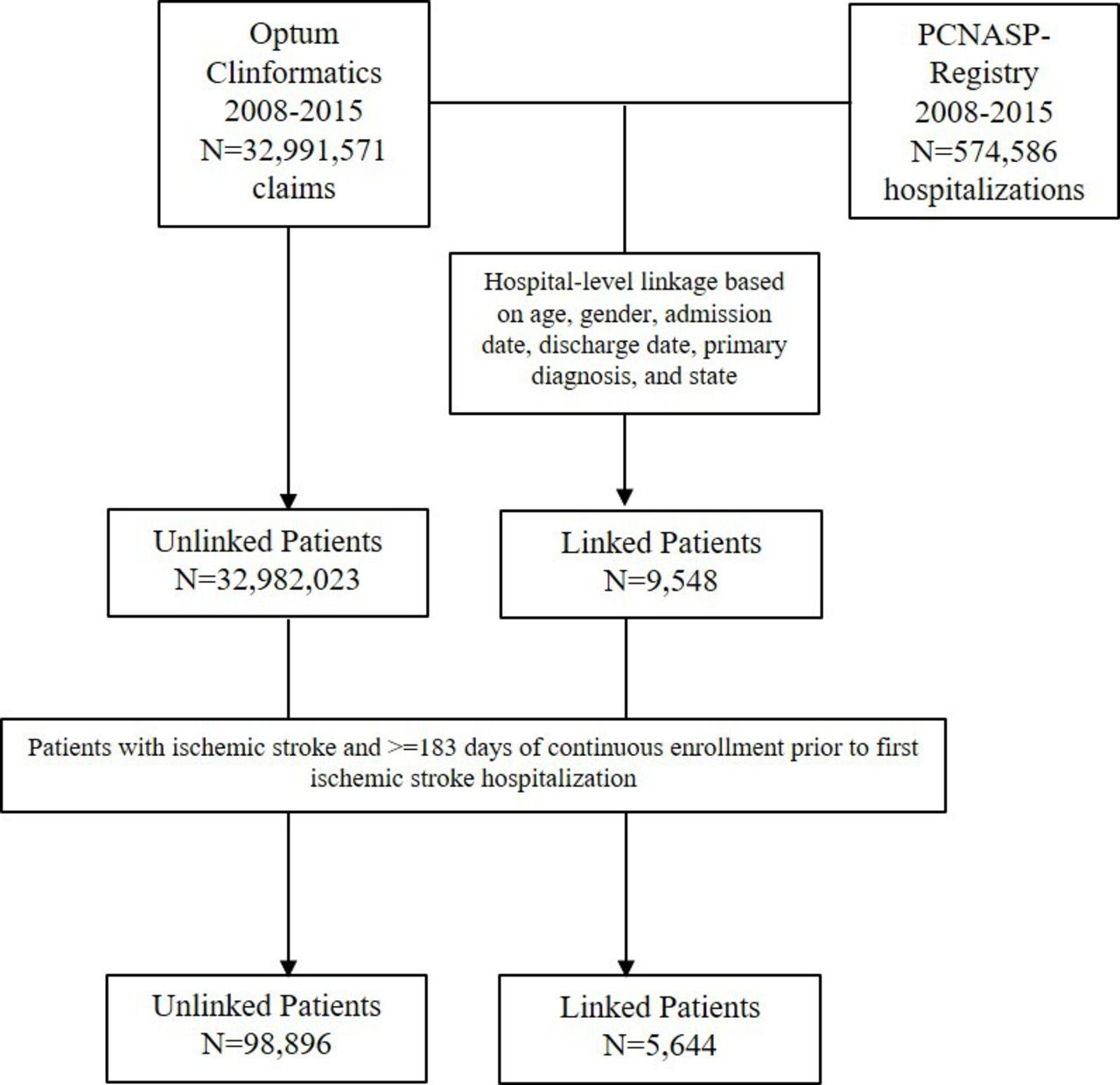
- Figure 1
Identification of linked and unlinked study cohorts resulting from data linkage between ischaemic stroke admissions in Paul Coverdell National Acute Stroke Program (PCNASP)—registry and ischaemic stroke admissions in claims dataset.
- Figure 2
Antihypertensive and lipid-lowering medication use prior and subsequent to index stroke hospitalisation as measured in Paul Coverdell National Acute Stroke Program (PCNASP) and in claims at 90 days prestroke and 90 days post dischargPCNASP (reported on admission): based on medications reported on admission in PCNASP registry. Claims (fills prior to admission): based on prescription medications filled in the 90 days prior to the stroke hospitalisation in claims. Antihypertensive and lipid-lowering medication use prior to admission in the PCNASP was missing for <1%. PCNASP (prescription at discharge): based on medications prescribed at discharge in PCNASP among patients discharged home. Antihypertensive and statin prescription at discharge in the PCNASP was missing for 11.3% and 1.7%, respectively. Claims (fills after discharge): based on prescription medications filled in the 90 days following discharge as recorded in claims among patients discharged home. To evaluate prescription medications filled following discharge in claims, analyses were limited to patients with continuous enrollment for the 90 days after the stroke hospitalisation. Antihypertensive drugs: includes ACE-inhibitors, angiotensin II receptor blockers (ARBs), beta-blockers, calcium channel blockers, thiazide diuretics, loop diuretics and other antihypertensives. Lipid-lowering drugs: includes statins or other lipid-lowering medications. PCNASP included information on the use of lipid-lowering drugs on admission and on the prescription of statins at discharge.


- Table 1
Linkage performance in claims dataset of 32 991 571 claims encounters
Linkage step Linkage rule*† Number of flexible fields for matching Total linked Hospitalisations Uniqueness‡ 1 Age at admission (±1 year), date of admission (±1 day), date of discharge (±1 day), sex, state, and primary diagnosis, by hospital ID 3 17 850 89.6 2 Age at admission, date of admission (±1 day), date of discharge, sex, state, and primary diagnosis, by hospital ID 1 10 917 98.0 3 Age at admission, date of admission, date of discharge (±1 day), sex, state, and primary diagnosis, by hospital ID 1 10 445 98.0 4 Age at admission (±1 year), date of admission, date of discharge, sex, state, and primary diagnosis, by hospital ID 1 14 004 98.0 5 Age at admission, date of admission, date of discharge, sex, state, and primary diagnosis, by hospital ID 0 10 079 99.1 *Unless otherwise specified, linkage rules employed exact matching of linking fields.
†Optum Clinformatics only includes year of birth for commercial beneficiaries, thus the linking field age at admission was always allowed to differ by 1 year.
‡Uniqueness = (1−(N multiple hospitalisations in claims+N multiple hospitalisations in registry))/N linked hospitalisations] *100
- Table 2
Comparison of claims variables between beneficiaries in Optum with versus without successful Paul Coverdell National Acute Stroke Program-linkage
Patient characteristics Linked
(n=5644)
N (%)Unlinked
(n=98 896)
N (%)Standardised difference Demographics Age, mean (SD) 69.7 (11.9) 72.5 (12.3) −0.23 Female 2797 (49.6) 51 821 (52.4) −0.06 Comorbidities* Combined comorbidity index, mean (SD) 1.4 (2.5) 1.5 (2.4) −0.03 Hypertension 3866 (68.5) 64 675 (65.4) 0.07 Diabetes 1974 (35.0) 31 964 (32.3) 0.06 Dyslipidaemia 2710 (48.0) 43 584 (44.1) 0.08 Prior ischaemic stroke 1192 (21.1) 17 852 (18.1) 0.08 Prior transient ischaemic attack 526 (9.3) 8802 (8.9) 0.01 History of atrial fibrillation 820 (14.5) 17 384 (17.6) −0.08 Carotid stenosis 411 (7.3) 6342 (6.4) 0.03 Prior haemorrhagic stroke 83 (1.5) 1067 (1.1) 0.03 Ischaemic heart disease or procedure 1341 (23.8) 22 974 (23.2) 0.01 Peripheral vascular disease (PVD) or PVD surgery 497 (8.8) 10 024 (10.1) −0.05 Congestive heart failure 786 (13.9) 14 487 (14.7) −0.02 Chronic kidney disease 699 (12.4) 13 338 (13.5) −0.03 Chronic obstructive pulmonary disease 694 (12.3) 12 772 (12.9) −0.02 Pneumonia 346 (6.1) 5890 (6.0) 0.01 Dementia 575 (10.2) 12 087 (12.2) −0.06 Cancer or history of malignant neoplasm 661 (11.7) 11 328 (11.5) 0.01 Obesity 811 (14.4) 13 357 (13.5) 0.02 Smoking 455 (8.1) 6411 (6.5) 0.06 Alcohol abuse or dependence 76 (1.4) 1221 (1.2) 0.01 Drug abuse or dependence 61 (1.1) 991 (1.0) 0.01 Depression 556 (9.9) 9194 (9.3) 0.02 Medication use* Any antihypertensives† 3437 (60.9) 62 519 (63.2) −0.05 Angiotensin-converting enzyme inhibitors 1556 (27.6) 28 447 (28.8) −0.03 Angiotensin II receptor blockers 738 (13.1) 12 944 (13.1) 0.00 Beta-blockers 1980 (35.1) 35 563 (36.0) −0.02 Calcium channel blockers 1361 (24.1) 23 941 (24.2) 0.00 Thiazide diuretics 1147 (20.3) 18 151 (18.4) 0.05 Loop diuretics 837 (14.8) 15 521 (15.7) −0.02 Other antihypertensives 458 (8.1) 8045 (8.1) 0.00 Nitrates and other antianginal therapies 389 (6.9) 6088 (6.2) 0.03 Antiarrhythmics 105 (1.9) 2044 (2.1) −0.01 Digoxin 176 (3.1) 4329 (4.4) −0.07 Any lipid-lowering agents‡ 2144 (38.0) 36 294 (36.7) 0.03 Statins 2016 (35.7) 33 977 (34.4) 0.03 Other lipid-lowering agents 340 (6.0) 5231 (5.3) 0.03 Antiplatelets§ 694 (12.3) 10 480 (10.6) 0.05 Anticoagulants¶ 491 (8.7) 9163 (9.3) −0.02 Warfarin 383 (6.8) 7778 (7.9) −0.04 Direct oral anticoagulants 94 (1.7) 1198 (1.2) 0.04 Heparin, LMWH or fondaparinux 66 (1.2) 935 (1.0) 0.02 Insulin 622 (11.0) 8937 (9.0) 0.07 Non-insulin glucose-lowering medications 1034 (18.3) 17 429 (17.6) 0.02 Antidepressants** 1145 (20.3) 19 146 (19.4) 0.02 Measures of healthcare utilisation* Any hospitalisation, % 1215 (21.5) 17 462 (17.7) 0.10 Number of any hospitalisation, mean (SD) 0.3 (0.7) 0.3 (0.7) 0.08 Any hospitalisation within prior 30 days, % 467 (8.3) 6426 (6.5) 0.07 N hospital days, mean (SD) 2.0 (6.1) 1.6 (5.6) 0.07 Number of emergency department visits, mean (SD) 0.8 (2.0) 0.7 (1.9) 0.09 Number of any physician visit, mean (SD) 12.8 (17.8) 10.5 (15.7) 0.14 Total N distinct pharmacological agents prescribed, mean (SD) 6.5 (6.0) 6.3 (5.6) 0.04 Laboratory values* LDL, mg/dL, mean (SD) 105.3 (56.9) 106.9 (44.7) −0.03 LDL, N (%) 123 (2.2) 2471 (2.5) −0.02 Total cholesterol, mg/dL, mean (SD) 199.6 (61.9) 193.3 (48.8) 0.11 Total cholesterol, N (%) 120 (2.1) 2514 (2.5) −0.03 INR, mean (SD) 1.6 (0.9) 1.7 (0.9) −0.02 INR, N (%) 19 (0.3) 384 (0.4) −0.01 Creatinine, mg/dL, mean (SD) 1.1 (0.5) 1.1 (2.1) −0.05 Creatinine, N (%) 171 (3.0) 3393 (3.4) −0.02 HbA1c, %, mean (SD) 8.2 (2.5) 7.8 (2.2) 0.15 HbA1c, N (%) 90 (1.6) 1530 (1.6) 0.00 Characteristics of stroke hospitalisation Length of stay of index hospitalisation, mean (SD) 5.7 (4.7) 5.9 (6.8) −0.05 Discharge status Home 2691 (47.7) 41 191 (41.7) 0.12 Home healthcare 680 (12.1) 10 376 (10.5) 0.05 Rehabilitation facility 480 (8.5) 8596 (8.7) −0.01 Skilled nursing facility 935 (16.6) 19 766 (20.0) −0.09 Other acute inpatient facility 331 (5.9) 6701 (6.8) −0.04 Hospice 190 (3.4) 4098 (4.1) −0.04 In-hospital mortality†† 33 (0.6) 516 (0.5) 0.01 Values are N (%) unless otherwise specified.
*Unless otherwise specified, measured during the 6 months preceding the index stroke hospitalisation.
†Includes ACE-inhibitors, ARBs, beta-blockers, calcium channel blockers, thiazide diuretics, loop diuretics, and other antihypertensives.
‡Includes statins or other lipid-lowering medications.
§Includes aspirin, clopidogrel, prasugrel, ticagrelor, dipyridamole, aspirin–dipyridamole, ticlopidine.
¶Includes warfarin, dabigatran, rivaroxaban, apixaban, edoxaban, heparin, dalteparin, enoxaparin, tinzaparin, fondaparinux, argatroban, desirudin, lipirudin.
**Includes selective serotonin reuptake inhibitors (SSRIs) and non-SSRI antidepressants.
††Information on mortality is available in Optum through linkage with the Social Security Administration Death Master File. This capture is limited by a policy change in 2011 concerning the extent of the Social Security Administration disclosure of death records received from states (important notice: change in public death master file records. 2011; https://classic.ntis.gov/assets/pdf/import-change-dmf.pdf).
ARBs, angiotensin II receptor blockers; HbA1c, haemoglobin A1c; INR, international normalised ratio; LDL, low-density lipoprotein; LMWH, low-molecular-weight heparin.
- Table 3
Assessment of discordance among selected variables from the Paul Coverdell National Acute Stroke Program (PCNASP) and claims data among linked patients
PCNASP-based variables
(n=5644)Claims-based variables
(n=5644)McNemar’s test p value Absolute difference Comorbidities*, N (%) Hypertension 4021 (71.5) 3866 (68.5) 0.00 3.0 Diabetes mellitus 1780 (31.8) 1974 (35.0) 0.00 3.2 Dyslipidaemia 2590 (46.1) 2710 (48.0) 0.01 1.9 Prior ischaemic stroke 1075 (21.9) 1192 (21.1) 0.12 0.8 Prior transient ischaemic attack 406 (8.1) 526 (9.3) 0.08 1.2 History of atrial fibrillation 1155 (20.5) 820 (14.5) 0.00 6.0 Carotid stenosis 222 (4.0) 411 (7.3) 0.00 3.3 Ischaemic heart disease 1323 (23.6) 1341 (23.8) 0.70 0.2 Peripheral vascular disease 315 (5.6) 497 (8.8) 0.00 3.2 Congestive heart failure 449 (8.0) 786 (13.9) 0.00 5.9 Chronic kidney disease 138 (11.4) 699 (12.4) 0.00 1.0 Obesity 624 (39.6) 811 (14.4) 0.00 25.2 Smoking 1024 (18.3) 455 (8.1) 0.00 10.2 Drug or alcohol abuse 32 (2.8) 61 (1.1) 1.00 1.7 Depression 174 (5.6) 556 (9.9) 0.00 4.3 Stroke severity and functional information at discharge† NIH Stroke Scale Mean (SD) 6.2 (7.2) N/A N/A N/A Median (IQR) 3 (1–8) N/A N/A N/A Ambulatory status at discharge Able to ambulate independently with or without device, N (%) 2698 (50.4) N/A N/A N/A *Comorbidities in the PCNASP are based on recorded medical history during stroke hospitalisation; comorbidities for in claims are based on International Classification of Diseases, Ninth Revision diagnoses recorded during the 183-day period prior to the stroke hospitalisation. Comorbidities in the PCNASP were characterised by varying level of missingness: information on prior ischaemic stroke, transient ischaemic attack, obesity, chronic kidney disease, drug or alcohol abuse, and depression was missing for 13.0%, 11.6%, 72.1%, 78.6%, 79.6% and 44.7%, respectively; information on the other comorbidities was missing for <1%.
†Information on National Institutes of Health (NIH) Stroke Scale and Ambulatory status at discharge was missing for 28.9% and 5.2% patients, respectively.
N/A, not applicable.
Supplementary Materials
Supplementary data
Additional Files
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.




{kind=link}
{kind=link}