

Abstract
Objective Open microsurgery, often with bypass techniques, is indispensable for complex aneurysms. To date, it remains unknown whether arterial anatomy or quantitative blood flow measurements can predict insufficient flow-related stroke (IRS). The present study aimed to evaluate the risk factors for IRS in patients treated with open microsurgery with bypass procedures for complex internal carotid artery aneurysms.
Methods Patients with complex aneurysms undergoing bypass surgery were retrospectively reviewed. The recipient/donor flow index (RDFI) was preoperatively evaluated using colour-coding angiography. RDFI was defined as the ratio of the cerebral blood volume of the recipient and donor arteries. The sizes of the recipient and donor arteries were measured. The recipient/donor diameter index (RDDI) was then calculated. IRS was defined as the presence of new postoperative neurological deficits and infarction on postoperative CT scans. We assessed the association between RDFI and other variables and the IRS.
Results Twenty patients (38±12 years) were analysed. IRS was observed in 12 patients (60%). Patients with postoperative IRS had a higher RDFI than those without postoperative IRS (p<0.001). RDDI was not significantly different between patients with and without IRS (p=0.905). Patients with RDFI >2.3 were more likely to develop IRS (p<0.001).
Conclusion Quantitative digital subtraction angiography enables preoperative evaluation of cerebral blood volume. RDFI >2.3, rather than RDDI, was significantly associated with postoperative IRS. This preoperative evaluation allows appropriate decisions regarding the treatment strategy for preventing postoperative IRS.
Introduction
Intracranial aneurysms are common lesions; previous studies have reported a prevalence of 3% in the adult population.1 The number of incidentally discovered aneurysms is increasing due to the increasing availability of cranial imaging.2 There are three modalities for treating intracranial aneurysms: observation, open microsurgery and endovascular occlusion. The past three decades have witnessed a rise in innovative techniques and studies, leading to the decrease in microsurgical cases and the shift of market forces and patient attitudes toward endovascular therapies.3–6 Simple aneurysms tend to be treated endovascularly with standalone coiling, balloon-assisted coiling and stent-assisted coiling. Flow diverters are now dominant in the treatment of internal carotid artery (ICA) aneurysms.7 Even for bifurcation aneurysms, intra-aneurysmal flow diverters have been developed for application.8 Nonetheless, aneurysms with wide necks, large size, dolichoectatic morphology, intraluminal thrombus, previous endovascular therapy or atherosclerotic walls still require open microsurgery.9 For complex aneurysms, bypass techniques are often needed; they function as conduits that replace lost flow from deliberate arterial sacrifice and restore vital circulation to the brain. However, their forms and blood flows vary widely. Although quantitative blood flow measurements with Doppler ultrasonography are logical, a bulky probe that must fit circumferentially around vessels for measurements makes it cumbersome with deep bypasses. Therefore, in complex aneurysms with deep bypasses, neurosurgeons usually base donor and recipient pairings on arterial anatomy rather than quantitative blood flow measurements.
Quantitative colour-coded digital subtraction angiography (DSA) provides visualisation of cerebrovascular flow in a single image according to the relative time to maximum intensity.10 It has been used to evaluate the haemodynamics in brain arteriovenous malformations, aneurysmal subarachnoid haemorrhage (SAH) and moyamoya disease.11–13 In this study, we aimed to quantitatively assess the blood flow in complex aneurysms of bypass donors and recipients and to investigate the correlation between the recipient/donor flow index (RDFI) and insufficient flow-related stroke (IRS).
Materials and methods
Patient selection
Following the approval of the Beijing Tiantan Hospital Research Ethics Committee, records of patients with intracranial aneurysms evaluated at our institution between 2012 and 2020 were retrospectively reviewed. Patients were included if they had DSA studies obtained before treatment and underwent open microsurgery with bypass techniques.
The onset presentations of patients were categorised into the following: SAH, headache, cranial nerve deficits and asymptomatic. The vascular origin of the aneurysm was classified into ICA or middle cerebral artery (MCA). Based on angiographic morphology and clinical context, we classified aneurysms as saccular or serpentine. The aneurysm size was measured using anteroposterior and lateral DSA images. With thrombotic aneurysms whose intraluminal diameter on angiography was less than the overall aneurysm diameter, axial CT or MRI was used to measure aneurysm size. In patients who harboured multiple aneurysms, aneurysms that led to the symptoms were selected for assessment and fixation.
Perioperative management
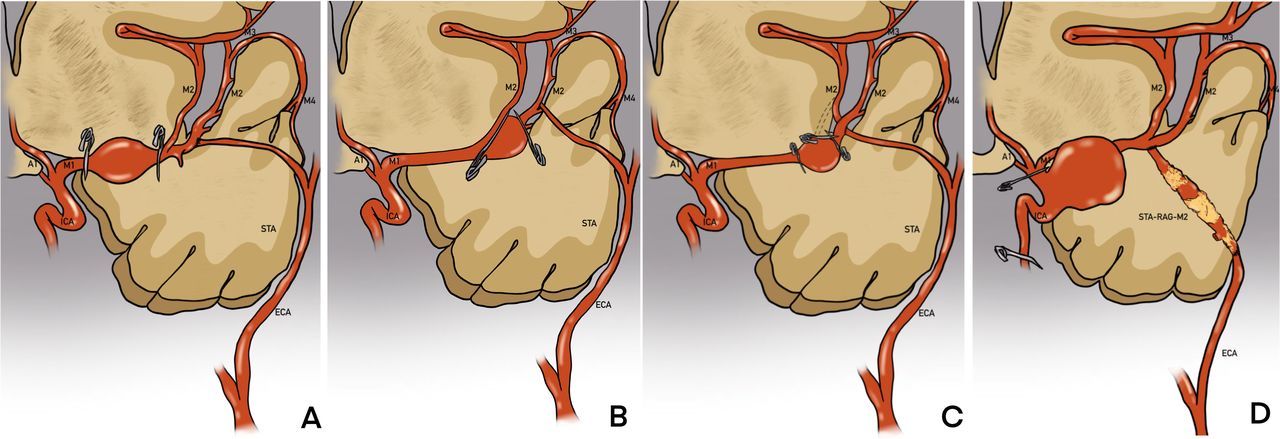
Patients with MCA aneurysms underwent superficial temporal artery to MCA (STA-MCA) bypass, while STA-radial artery graft to the MCA (STA-RAG-MCA) bypass was performed in patients with ICA aneurysms. An Allen test was performed to confirm an intact palmar arch and adequate hand perfusion despite occlusion of the radial artery (RA). STA and RA were mapped with the Doppler flow probe, harvested and prepared in advance. The aneurysms were exposed using standard site-appropriate surgical approaches. For MCA aneurysms, one branch of the STA was anastomosed to the distal M2 segment, which is usually the inferior trunk. Two permanent clamps were placed proximal and distal to the aneurysm (figure 1A). For MCA bifurcation aneurysms, there are usually two situations: (1) when aneurysms incorporating the origin of one of the M2 branches, we performed a clip reconstruction of the parent artery, and the STA branch was anastomosed to the M2 branch originating from the aneurysm (figure 1B). (2) When both MCA branches originated from the aneurysm, we performed a double reimplantation technique. One branch of the STA was anastomosed to the inferior trunk. The superior trunk was isolated between the aneurysm clips, transected and reimplanted on the inferior trunk (figure 1C). For ICA aneurysms, the trunk of the STA was end-to-end anastomosed to the RAG, and the other side of the RAG was anastomosed to the M2 segment. The proximal and distal aneurysms were permanently occluded (figure 1D). Adequacy of treatment and patency of graft vessels were analysed intraoperatively using intraoperative angiography, indocyanine green fluorescence video angiography (ICG-VA) or postoperative computed tomography angiography (CTA) (3–5 days after surgery). All patients underwent a CT scan within the first day after surgery. After ruling out the intracranial haematoma, aspirin was administered postoperatively and continued indefinitely (100 mg once a day for life). Repeat CT or MRI scans were performed in cases of postoperative neurological deterioration.

A schematic diagram of the two bypass procedures. (A) STA-M2 bypass; (B) clip reconstruction and STA-M2 bypass; (C) double reimplantation technique of STA-M2 bypass; (D) STA-RAG-M2 bypass. RAG, radial artery graft; STA, superficial temporal artery.
Conventional DSA
All enrolled patients underwent preoperative cerebral angiography in a dual-plane angiographic machine (Siemens, Erlangen, Germany) performed by professional neuroradiologists. A 5F angiographic catheter (TERUMO Medical Device, Shanghai, China) was used according to the patient’s femoral artery diameter. Conventional DSA images included anteroposterior and lateral common carotid artery angiograms. A bolus of 7 mL diluted contrast media (iobitridol; TERUMO Medical Device, Shanghai, China) with a contrast-to-normal-saline ratio of 1:1 was automatically injected at a flow rate of 5 mL/s within 1.4 s. Image acquisition was initiated 0.2 s before the contrast injection. The 2D DSA series was acquired at four frames per second. The entire DSA acquisition lasted 12 s but was manually prolonged to enable visualisation of the internal jugular vein opacification from normal brain parenchyma if required.
Postprocessing of DSA
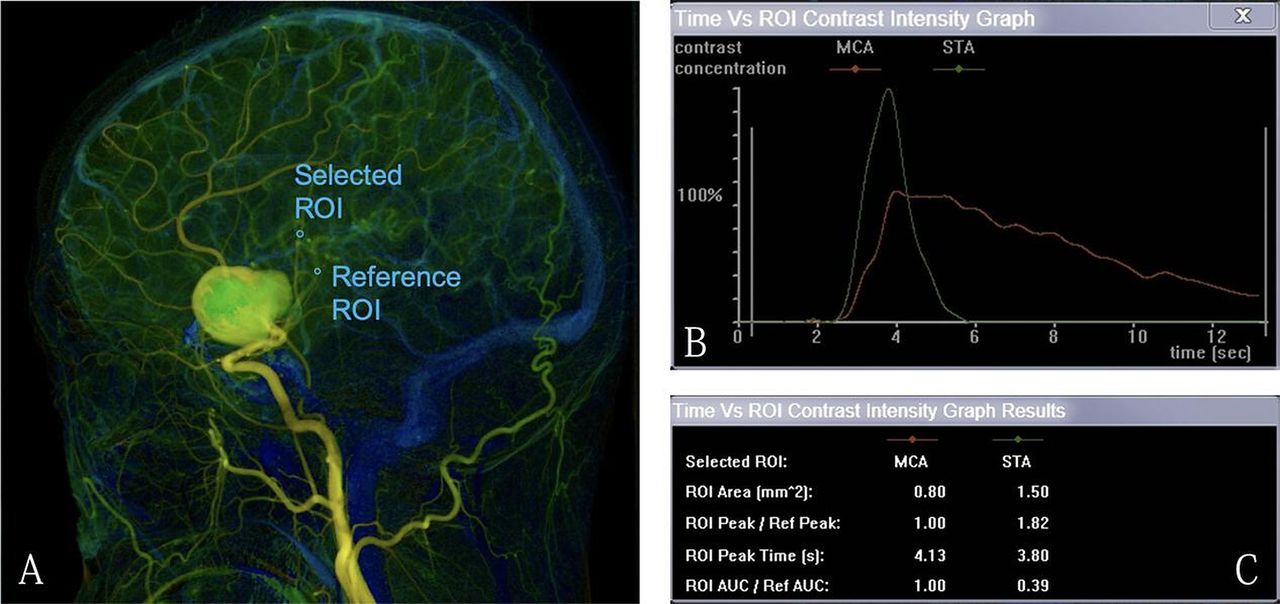
The colour-coded (ranging from red to blue) single image was obtained with postprocessing software (syngo iFlow; Siemens, Berlin, Germany), with a minimum measurement accuracy of 0.26/0.27 s. Two neuroradiologists who were blinded to the clinical baseline of the patients drew round regions of interest (ROIs) within the donor and recipient artery on the same colour-coded image (figure 2A). For each set of manually drawn ROIs, a time-attenuation intensity curve was automatically obtained by the software (figure 2B). Using the curve, the calculated area under the curve (AUC) is the total amount of contrast media passed, which corresponds to the cerebral blood volume of the perfusion MRI.14 The RDFI was calculated by dividing the recipient artery AUC values by the donor artery AUC values (figure 2C).

Postprocessing cascade of the DSA image. (A) A colour-coded single image is obtained from DSA images of common carotid artery angiography; then, we draw selected ROIs along the superficial temporal artery (STA). A reference ROI is drawn within the distal middle cerebral artery (MCA) of the aneurysm. (B) The time-attenuation intensity curve is obtained automatically. The green line represents the time-attenuation intensity curve within the STA, and the red line represents that of the MCA. (C) Using the time-attenuation intensity curve, we calculated the AUC within the STA, adjusted by the MCA. AUC, area under the curve; DSA, digital subtraction angiography; ROI, region of interest.
RDFI=AUCrecipient/AUCdonor
The diameter of the donor and recipient arteries was measured on the 2D DSA series, and the recipient/donor diameter index (RDDI) was calculated as follows:
RDDI=diameterrecipient/diameterdonor
In this study, the postprocessing of DSA was preferred to use anteroposterior projection because detection of donor and recipient arteries was easier than in lateral images.
Clinical outcome
The IRS was defined as new neurological deficits and ipsilateral hemisphere hypodensity sign on CT scan after the procedure.15 An IRS was distinguished from aneurysm-related perforator infarction based on CT findings. In aneurysm-related perforator infarctions, CT showed no lesions in the watershed territory. The neurological status of the patient was evaluated according to the modified Rankin Scale score, which was obtained on admission and at discharge. Clinical outcomes were evaluated by a clinician, who was blinded to the results of quantitative DSA (QDSA).
Statistical analysis
Categorical variables were analysed using the Pearson Χ2 test or Fisher’s exact test. Continuous variables were compared using independent Student’s t-test. Multivariate analysis was performed using a conditional logistic regression model that adjusted for potential factors related to postoperative IRS, including RDFI. A receiver operating characteristic (ROC) curve and subsequent analysis of the AUC were applied to evaluate the RDFI for predicting the IRS. Interobserver variability for the assessment of collaterals between the two observers was assessed using κ statistics. Statistical significance was set at p<0.05. Data were analysed using IBM SPSS Statistics (V.26.0; IBM Corp).
Results
Demographics and aneurysm characteristics
Open microsurgery with bypass was performed between May 2012 and September 2020 in 20 patients with complex aneurysms. A summary of each patient treated with the bypass technique is presented in table 1. Of these patients, 13 were female (13 of 20, 65%) and 7 were male (7 of 20, 35%). The average age of all patients was 38.1±11.6 years (range 20–60 years). Headache was the most common clinical presentation, accounting for 45% (9 of 20) of cases. Among the four patients presenting with varying degrees of cranial nerve deficits, visual deficits were the most common symptoms (3 of 4, 75%). One patient presented with a recurrent aneurysm after a previous microsurgical clipping. The size of the aneurysm ranged from 15 to 75 mm (mean, 35.8±13.3 mm). The MCA was the most frequently involved site, which harboured 13 aneurysms (65%).
Clinical summary of 20 patients with aneurysms who underwent bypass treatment
Association between RDFI and RDDI versus IRS
The two observers exhibited agreement in the RDFI (κ=0.726; p<0.001) and RDDI (κ=0.706; p<0.001). Among the enrolled patients, 12 (12 of 20, 60%) were diagnosed with IRS. There were no significant differences in the RDDI between patients with and without IRS. However, patients with IRS had significantly higher RDFI (3.3±1.0 vs 1.5±0.4, p<0.001) than those without IRS (table 2). After adjusting for age, sex, smoking status and hypertension, RDFI was significantly associated with IRS. The ROC curve demonstrated that RDFI >2.3 predicted a higher IRS rate, with a sensitivity and specificity of 83.3% and 100%, respectively. The area under the ROC curve was 0.9688 (95% CI, 0.906 to 1.000; p<0.001; figure 3).
Clinical characteristics and DSA parameters versus IRS

The area under the receiver operating characteristic curve was 0.763 (95% CI, 0.906 to 1.000; p<0.001). Recipient/donor flow index >2.3 predicted postoperative insufficient flow-related stroke with the highest combination of sensitivity (83.3%) and specificity (100%). AUC, area under the curve.
Representative case
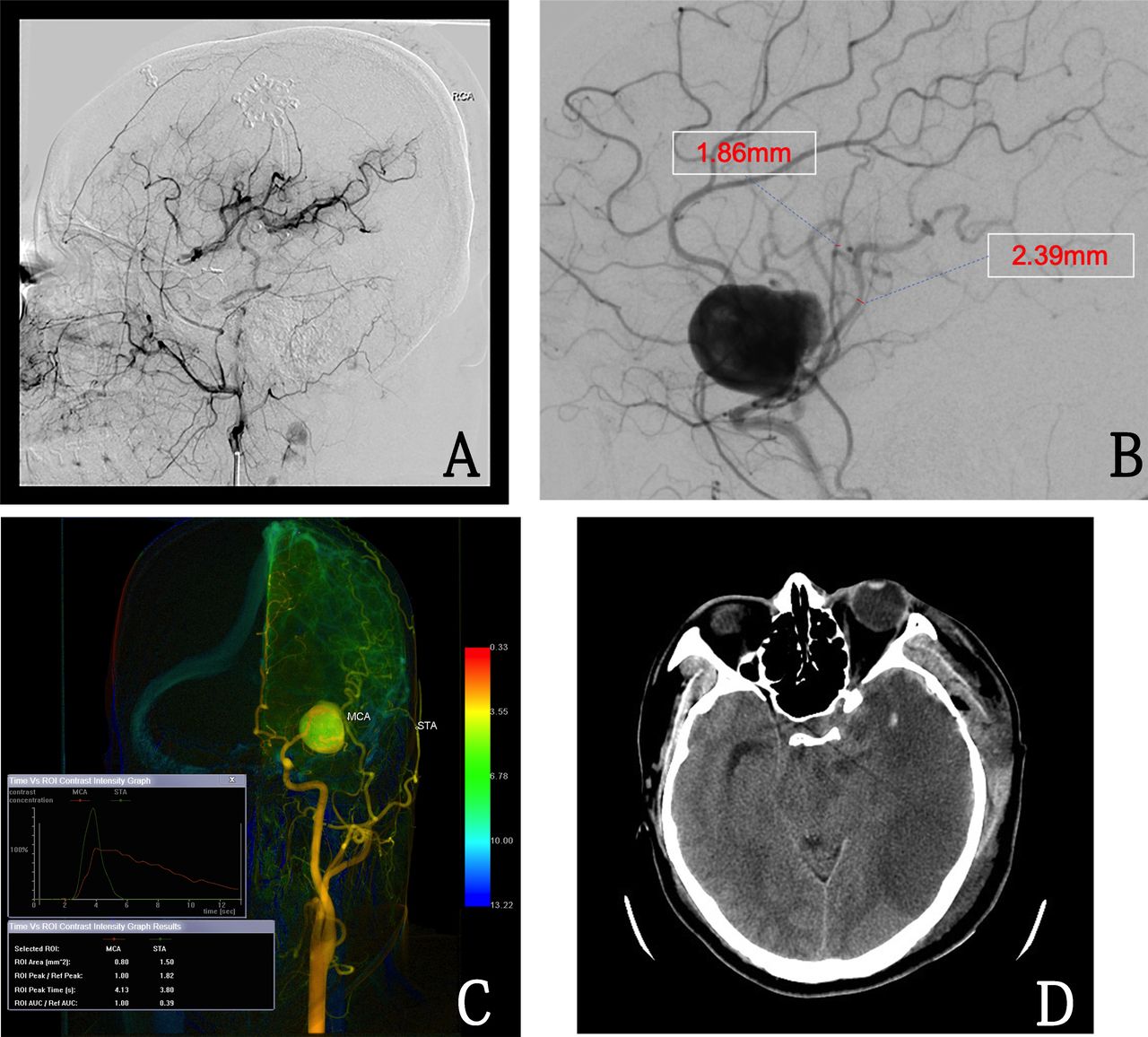
A middle-aged man (patient 13) presented with a severe headache. CT showed SAH, and angiography revealed a 25 mm saccular aneurysm involving the left MCA. He underwent left frontotemporal craniotomy, and the proximal afferent artery and distal efferent artery of the aneurysm were clipped. The parietal branch of the STA was anastomosed to the M2 segment. Postoperative DSA confirmed complete obliteration of the aneurysm and patency of the graft vessel (figure 4A). The diameters of the donor and recipient artery measured by the 2D DSA were 1.86 mm and 2.39 mm, respectively (figure 4B). The RDFI was 2.6, according to the QDSA (figure 4C). Postoperative CT showed a territory infarction in the left hemisphere (figure 4D). He was discharged with hemiparesis on the right side. After 12-month rehabilitation, his hemiparesis improved dramatically. He was dependent on his activities of daily living at the last follow-up.

Representative case. (A) Left internal carotid artery (ICA) lateral angiographic injection confirmed the patency of the graft. (B) Left ICA lateral angiographic injection showed the diameters of STA and MCA were 1.86 mm and 2.39 mm, respectively. (C) Quantitative DSA showed the recipient/donor flow index was 2.6. (D) CT showed a territory infarction in the MCA area. AUC, area under the curve; DSA, digital subtraction angiography; MCA, middle cerebral artery; ROI, region of interest; STA, superficial temporal artery.
Discussion
Although the volume of open aneurysm surgery is declining and endovascular therapy plays an increasingly important role in the treatment of intracranial aneurysms, complex aneurysms still require open microsurgery. There is heavy reliance on indirect aneurysm occlusion plus bypass techniques in treating this challenging intracranial aneurysm subtype.16 In this study, we used QDSA haemodynamic analysis to calculate the ratio of recipient to donor cerebral blood volume (CBV) and determined an RDFI to represent whether the donor and recipient matched. In our cohort, the IRS was significantly associated with RDFI >2.3, rather than the value of RDDI. Moreover, the RDFI is based on the ratio of the recipient and donor arteries. Therefore, theoretically, it is not affected by some factors influencing the pixel value in angiographic studies, including differences in kiloelectron volt level settings among patients or the iodine concentration of the contrast medium.
Complex aneurysms are not frequently observed in intracranial aneurysms. However, it is usually symptomatic due to its large size and intraluminal thrombus. Our previous study reported a poor prognosis for these patients if the aneurysms were left untreated.17 Currently, indirect aneurysm occlusion with bypass techniques is considered the ‘first-line’ management approach for complex aneurysms. Although the STA-MCA bypass is a convenient procedure that replaces lost flow from the MCA sacrificed,18 owing to its limited blood flow, its effectiveness is sceptical when the ICA is occluded.19 The external carotid artery-to-MCA (ECA-MCA) (the RA was used as a graft), on the other hand, has been used when a larger amount of blood flow is necessary.20 In one of the largest experiences with 54 bypass procedures, Sughrue et al 16 reported that the ECA-MCA bypass is the most common high-flow bypass, while the STA-MCA bypass is the most common low-flow bypass in their cohort. However, they did not comment on the selection criteria for the two bypass procedures and evaluation of the artery flow. Matsukawa et al 21 used a backup STA to MCA bypass to measure the intraoperative MCA pressure after temporary clamping of the ICA and release of the RAG bypass. They demonstrated that patients with postoperative watershed infarctions had lower intraoperative MCA pressure. The insufficient graft flow led to stroke, even if the graft was patent. However, the measurement of intraoperative MCA pressure might increase the technical difficulty and prolong the operation time. Moreover, it was intraoperative rather than a preoperative evaluation. Whether the graft flow is sufficient remains uncertain until the bypass procedure is complete.
Planning a bypass entails pairing the recipient artery in need of revascularisation with a donor artery. It is generally believed that bypasses with a donor artery whose size matches that of the recipient artery will replace the flow lost in the sacrificed or occluded artery.22 However, according to Poiseuille’s law,23 blood flow depends not only on the diameter of the vessels but also on the perfusion pressure. Pairing the recipient artery and donor artery according to size alone may be inappropriate. Our results showed that there was no significant difference in RDDI between patients with and without postoperative IRS. Using QDSA haemodynamic analysis, we obtained time-attenuation intensity curves of the contrast media passing through the donor and recipient arteries. The calculated AUC is the total amount of contrast media passed, which corresponds to passing the CBV. To our knowledge, the present study shows for the first time that preoperative RDFI values higher than 2.3 are associated with postoperative IRS. On the other hand, RDFI can be detected preoperatively, evaluating whether the graft flow is sufficient before the operation to guide the operator in choosing the appropriate bypass procedures.
The patency of all grafts was confirmed using intraoperative DSA or ICG-VA in the present study. However, more than half of the patients developed postoperative IRS (10 of 20, 50%). All operations were performed by experienced neurosurgeons in our institution (our institution is one of the largest neurovascular centres in China, with approximately 2000 operations per year). The high incidence of IRS might not be attributed to operational errors caused by the operator’s inexperience. Given the rarity of this disease, only 20 patients were enrolled in the present study. However, it should be noted that 56 patients with complex aneurysms underwent bypass procedures between 2012 and 2020 at our institution. Of these, 36 were excluded because of the lack of available DSA for postprocessing. The incidence of IRS was 35.7% (20 of 56), which is comparable with that reported in previous studies.24 The selection of the bypass type may be another reason.20 In the present study, all patients underwent STA branch-M2 bypass or STA trunk-RA-M2 bypass. The low-flow STA-MCA bypass procedure might provide limited flow when managing complex ICA aneurysms, for example, when the distal ICA is deliberately occluded. Among the seven patients with ICA aneurysms, 71.4% (5 of 7) developed IRS, while the incidence of IRS was 53.8% (7 of 13) in patients with MCA aneurysms. Hyperperfusion syndrome is one of the most common complications after revascularisation; it has also been observed in aneurysms with high-flow bypass.25 26 Thus, performing a high-flow ECA-MCA bypass for all patients seems inappropriate. In addition, high-flow ECA-MCA bypass requires long interposition grafts at the RAG limit. Not all patients are able to collateralise the hand through an incompetent palmar arch, or the RA may be unavailable due to atherosclerosis or trauma, or just the RA may be too short. It is necessary to base donor and recipient pairings on preoperative quantitative blood flow measurements and make an individual bypass plan for each patient. Also, there are several other factors that may contribute to postoperative ischaemic complications, such as the temporary occlusion time. Thus, the intraoperative electrophysiological monitoring was routinely applied. In our cohort, 10 patients’ motor evoked potential remain unchanged after the temporary occlusion while the other 10 patients’ motor evoked potential dropped after the temporary occlusion. In patients with dropped motor evoked potentials, four patients recovered to the baseline after the completion of the bypass and removal of the temporary occlusion while six patients recovered only partly. However, it should be noted that not only the long temporary occlusion time but also the insufficient blood flow affects the result of intraoperative electrophysiological monitoring. Thus, there may be a combination of long temporary occlusion time and insufficient blood flow of the bypass artery in these patients. Further studies were essential to distinguish the IRS more precisely.
Another issue worthy of attention is graft patency during follow-up. Almost all previous studies reported a graft patency rate of approximately 90% in their cohort.16 21 However, these data are based on intraoperative DSA, ICG-VA or short-term postoperative CTA. Yoon et al 27 reported the long-term bypass patency in a large cohort. They showed an overall cumulative patency rate of 97%, and the low-flow bypass had a significantly higher patency rate than high-flow bypasses. In addition, patients who presented with aneurysms had a lower patency rate than those with moyamoya disease or chronic vessel occlusion. Thus, due to its uncertain long-term endurance, high-flow bypass may not be suitable for all patients with complex aneurysms. The association between antiplatelet therapy and bypass patency has rarely been reported in the literature. In some institutions, aspirin is started postoperatively on the day of surgery and continues indefinitely.22 This is consistent with our institution’s experience. A randomised clinical trial that enrolled 500 patients with coronary artery bypass grafting demonstrated that ticagrelor plus aspirin significantly increased graft patency after 1 year compared with aspirin alone.28 However, for patients with complex aneurysms, whether the use of aspirin and antiplatelet agents added to aspirin can improve graft patency after bypass procedures remains unclear.
Our study quantified the pairing between the recipient and the donor artery using an RDFI, the ratio of the recipient to donor CBV obtained from QDSA analysis of patients with complex aneurysm. In addition to the traditional DSA angioarchitecture analysis, we emphasised the critical role of QDSA. The results indicate that RDFI, but not RDDI, appears to be a major factor in IRS. Further research using an alternative method for more accurate quantification of the recipient and donor CBV, such as quantitative magnetic resonance angiography, is required to prove this hypothesis.
There are several limitations to the study that need to be noted for the accurate interpretation of our data. Because of the small number of cases and non-randomised, single-centre retrospective study design, we identified that RDFI was associated with IRS, but the power could not be determined; thus, further studies with a larger number of cases are warranted. However, our study provides a feasible quantitative approach to base donor and recipient pairings.
Conclusion
QDSA enables preoperative evaluation of CBV without additional invasion, contrast medium or irradiation. RDFI >2.3, rather than RDDI, was significantly associated with postoperative IRS. This preoperative evaluation allows appropriate decisions regarding the treatment strategy for preventing postoperative IRS.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the IRB of Beijing Tiantan Hospital, Capital Medical University. All patients gave their informed consent before participation.
Footnotes
Contributors JL designed the study, wrote the manuscript, researched the data and contributed to the discussion. CX and XH designed the study, researched the data and edited the manuscript. YZ, DZ and JZZ contributed to the discussion and edited the manuscript. XC designed the study, researched the data, reviewed/edited the manuscript and contributed to the discussion.
Funding This study is supported by the National Key Technology Research and Development Program of the Ministry of Science and Technology of China (2015BAI12B04), Beijing Science and Technology Supporting Plan (D16110000381605), Beijing Municipal Administration of Hospitals’ Mission Plan (SML20150501), Beijing Municipal Administration of Hospitals Incubating Program (PX2016034) and National Natural Science Foundation of China (81571110, 81771234).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}