

Article Figures & Data
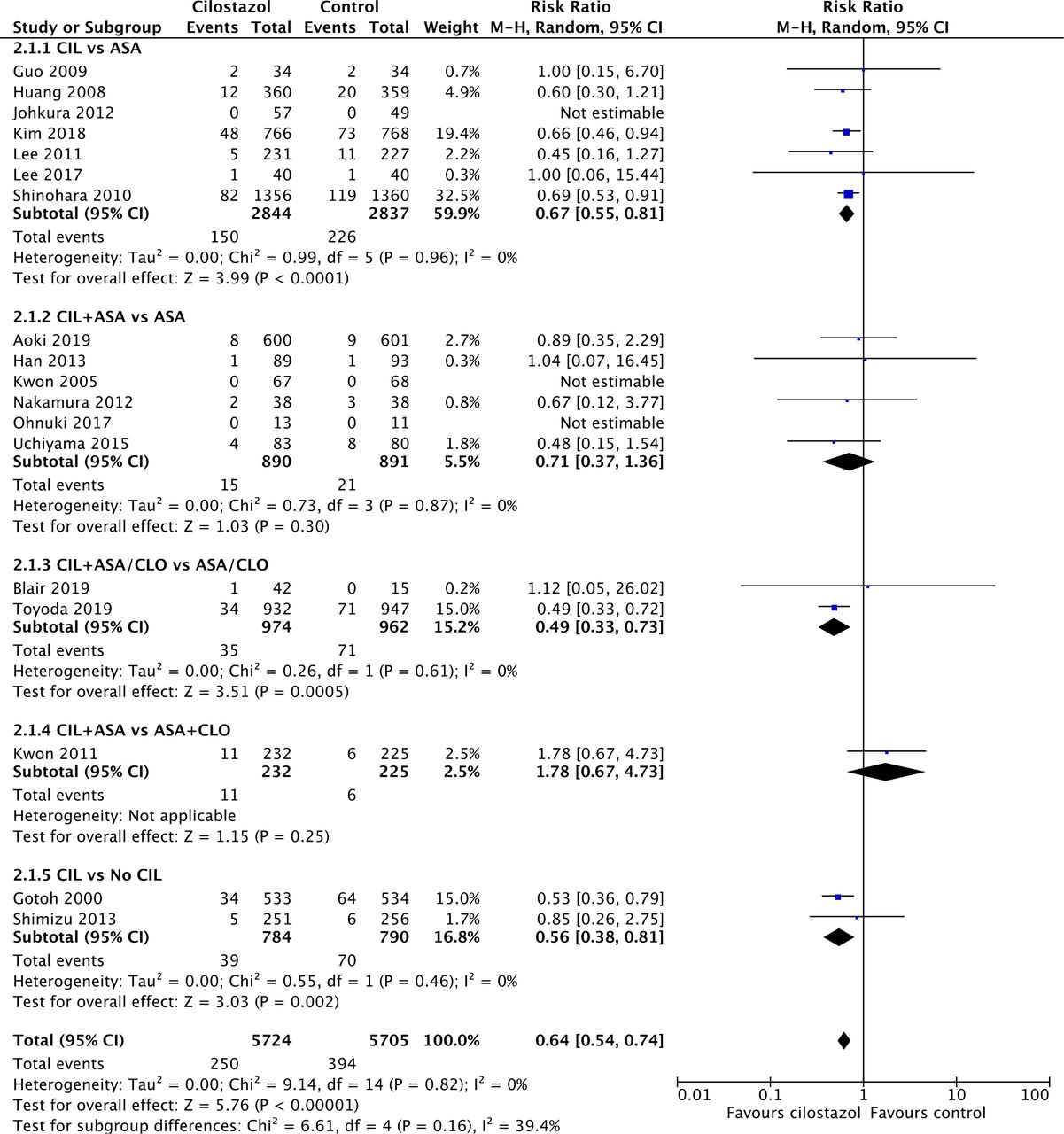
- Figure 1
Forest plot depicting risk of ischaemic stroke recurrence. ASA, aspirin; CIL, cilostazol; CLO, clopidogrel; No CIL, placebo or best medical therapy.
- Figure 2
Forest plot depicting risk of any stroke recurrence. ASA, aspirin; CIL, cilostazol; CLO, clopidogrel; No CIL, placebo or best medical therapy.
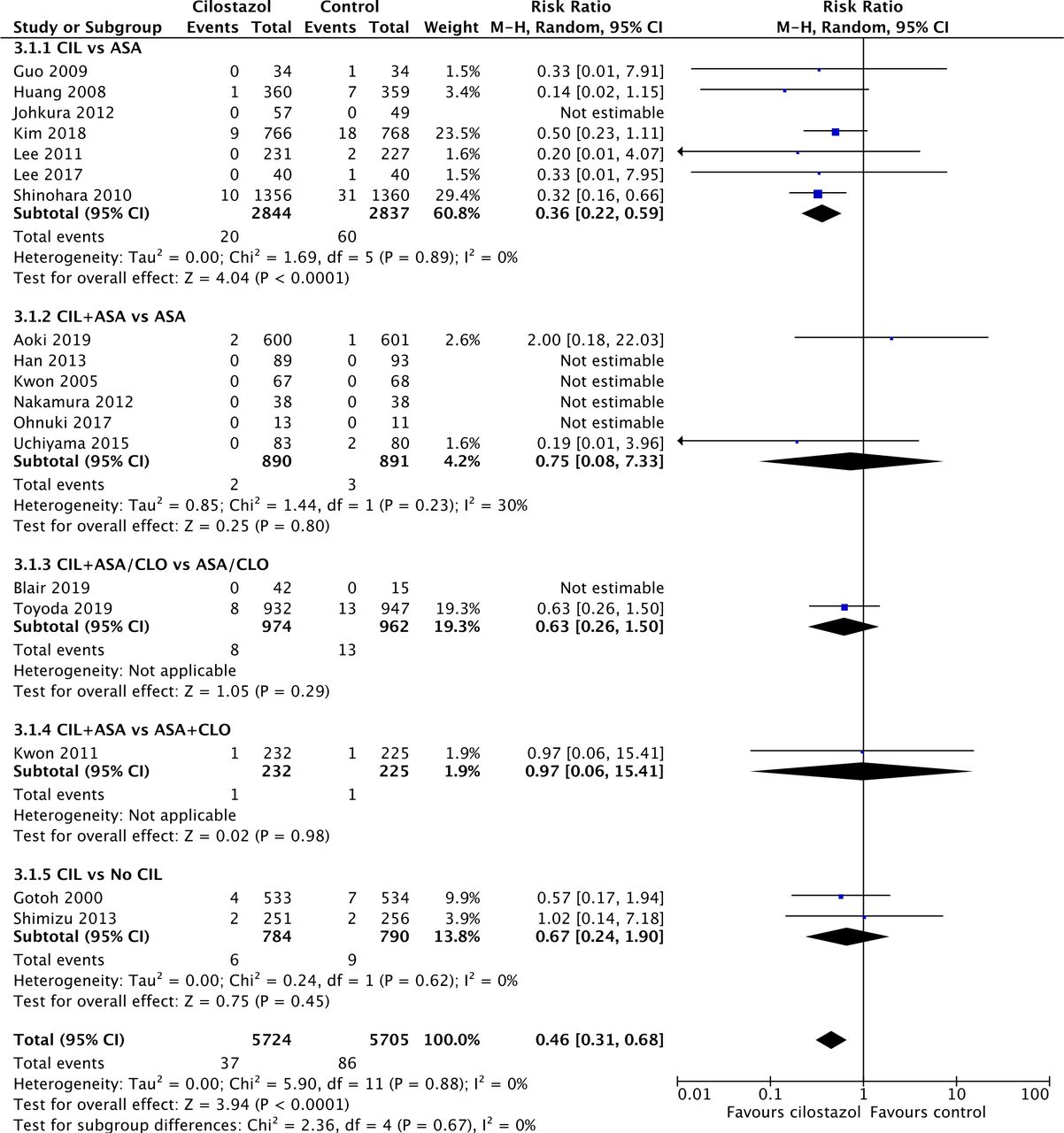
- Figure 3
Forest plot depicting risk of intracranial haemorrhage. ASA, aspirin; CIL, cilostazol; CLO, clopidogrel; No CIL, placebo or best medical therapy.
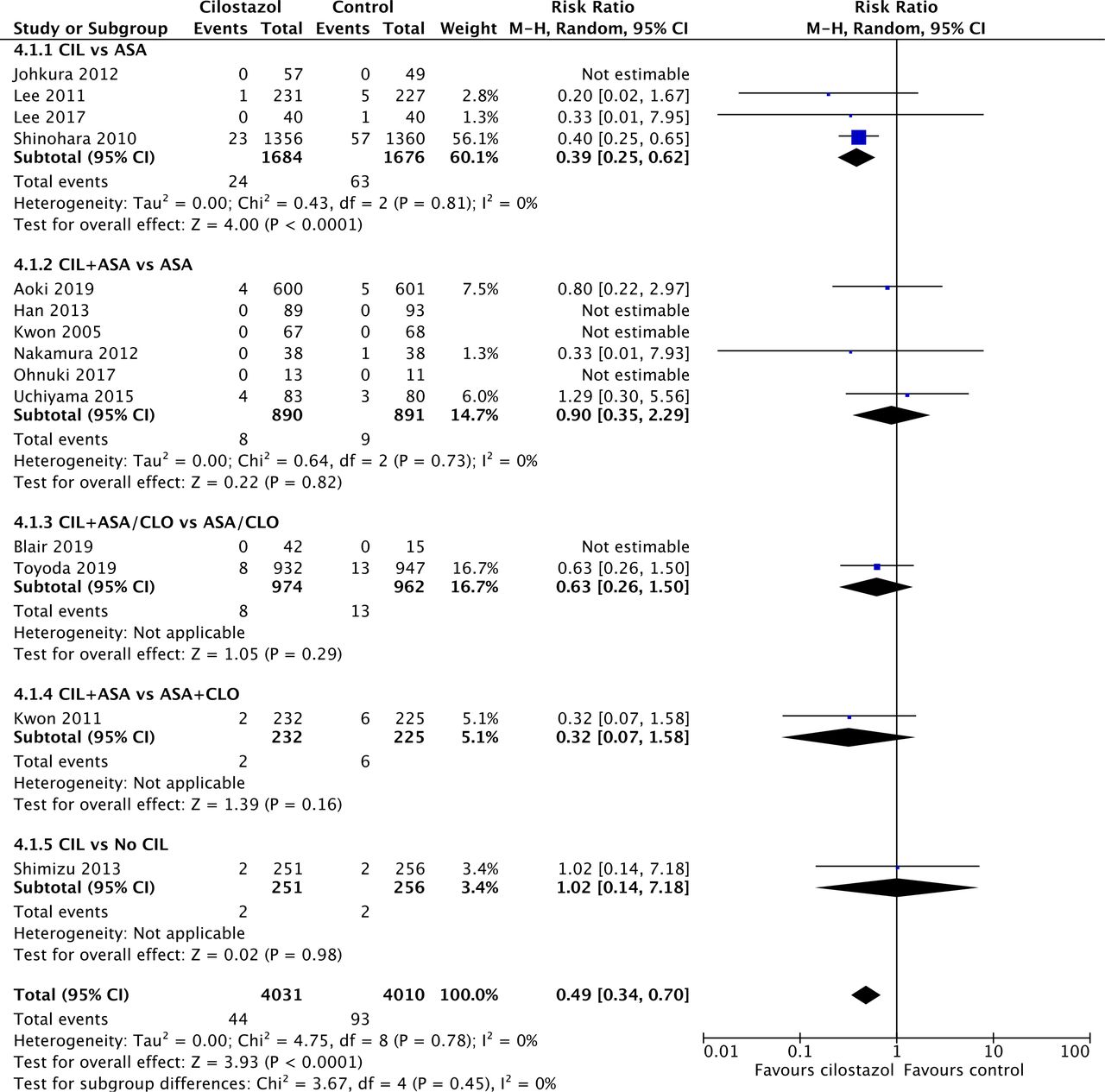
- Figure 4
Forest plot depicting risk of major haemorrhagic events. ASA, aspirin; CIL, cilostazol; CLO, clopidogrel; No CIL, placebo or best medical therapy.
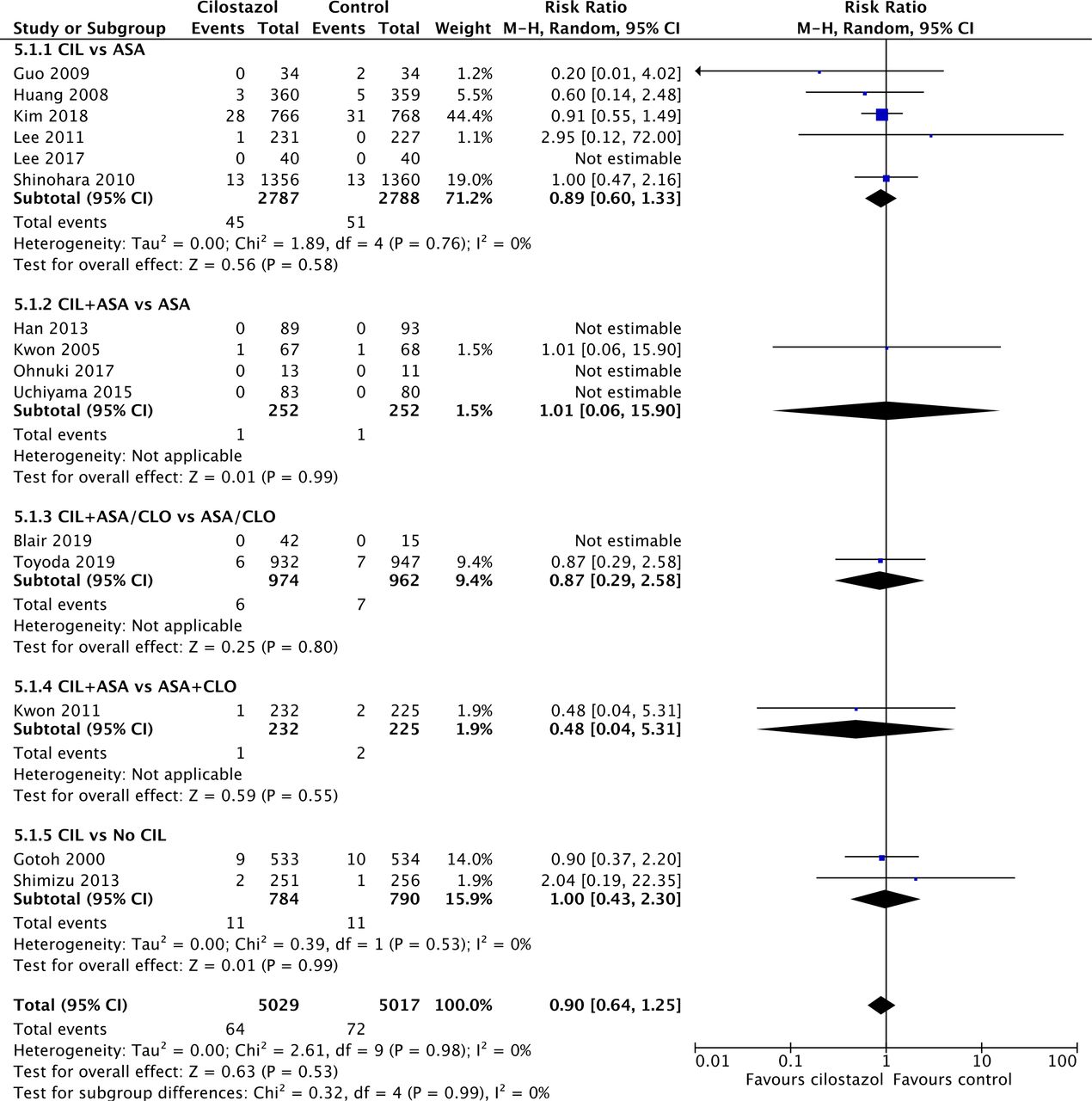
- Figure 5
Forest plot depicting risk of mortality. ASA, aspirin; CIL, cilostazol; CLO, clopidogrel; No CIL, placebo or best medical therapy.





- Table 1
Characteristics of included studies
Study ID Country Sample size, ITT (% male) Age (intervention) Age (control) Intervention Control Aoki 2019 (ADS)*22 Japan 1201 (66%) 69 (IQR 60–77) 69 (IQR 61–78) Cilostazol 200 mg + aspirin 81–200 mg Aspirin 81–200 mg Blair 2019 (LACI-1)23 UK 57 (68%) Mean of all participants: 66.1 (11.1) Cilostazol 100 mg BD + aspirin/clopidogrel Aspirin/clopidogrel Gotoh 2000 (CSPS)24 Japan 1067 (66%) 65.2 (8.7) 65.1 (8.8) Cilostazol 100 mg BD Placebo Guo 200925 China 68 (35%) 59.44 (10.63) 62.02 (11.12) Cilostazol 100 mg BD Aspirin 100 mg Han 2013 (ECLIPse)26 Korea 182 (25%) 64.63 (9.07) 65.48 (9.92) Cilostazol 100 mg BD + aspirin 100 mg Aspirin 100 mg Huang 2008 (CASISP)27 China 719 (69%) 60.14 (10.05) 60.31 (9.71) Cilostazol Aspirin Johkura 201228 Japan 106 (43%) 76.7 (9.8) 73.7 (9.4) Cilostazol 200 mg Aspirin 100 mg Kim 2018 (PICASSO)29 South Korea, Hong Kong, Philippines 1534 (62%) 65.5 (10.9) 65.8 (10.7) Cilostazol 100 mg BD Aspirin 100 mg Kwon 2005 (TOSS)30 South Korea 135 (61%) 62.28 (10.42) 62.54 (8.97) Cilostazol 100 mg BD + aspirin 100 mg Aspirin 100 mg Kwon 2011 (TOSS-2)31 4 East Asian countries 457 (51%) 66.42 (11.33) 64.58 (11.11) Cilostazol 100 mg BD + aspirin 75–150 mg Clopidogrel 75 mg + aspirin 75–150 mg Lee 2011 (CAIST)32 Korea 458 (61%) 63 (12) 63 (12) Cilostazol 200 mg Aspirin 300 mg Lee 201733 Korea 80 (65%) 57.4 (12.7) 59.5 (11.7) Cilostazol 100 mg BD Aspirin 100 mg Nakamura 201234 Japan 76 (74%) 66 (12) 67 (10) Cilostazol 100 mg BD + aspirin 300 mg Aspirin 300 mg Ohnuki 201735 Japan 24 (71%) 60.5 (10) 63.6 (9.1) Cilostazol 200 mg + aspirin 100 mg Aspirin 100 mg Shimizu 201336 Japan 507 (67%) 66.2 (9.4) 66.6 (8.9) Cilostazol 200 mg + optimal medical treatment Optimal medical treatment Shinohara 2010 (CSPS 2)37 Japan 2716 (72%) 63.5 (9.2) 63.4 (9.0) Cilostazol 100 mg BD Aspirin 81 mg Toyoda 2019 (CSPS.com)38 Japan 1879 (70%) 69.6 (9.2) 69.7 (9.2) Cilostazol 100 mg BD + aspirin 81–100 mg/ clopidogrel 50–75 mg Aspirin 81–100 mg/ clopidogrel 50–75 mg Uchiyama 2015 (CATHARSIS)39 Japan 163 (66%) 68.3 (range 45–84) 68.3 (range 50–82) Cilostazol 200 mg + aspirin 100 mg Aspirin 100 mg All data are in mean (SD) or median (IQR/range).
*After 14 days, both arms were swapped to cilostazol 200 mg until 3 months. Where possible, we analysed data at 14 days instead of 3 months.
ITT, intention to treat.
- Table 2
Details of included studies
Study ID Time to randomisation/treatment Duration of treatment/ follow-up Type of stroke Cilostazol Control Aoki 2019 (ADS)22 Within 48 hours
Cilostazol: 10.1 hours (IQR 4.6–20.0)
Control: 11.5 hours (IQR 4.8–20.9)14 days, 3 months Symptomatic ICAS (23%)
Large-artery atherosclerosis (13%),
LACI (46%), branch atheromatous disease (13%)Symptomatic ICAS (22%)
Large-artery atherosclerosis (15%),
LACI (43%), branch atheromatous disease (16%)Blair 2019 (LACI-1)23 Within 4 years
Median: 203 days (range 6–920)Treatment: 6–9 weeks
Follow-up: 11 weeksLACI LACI Gotoh 2000 (CSPS)24 1–6 months
Cilostazol: 83.0 days (range 7–1805)
Control: 82.4 days (range 8–1079)Mean follow-up duration:
Cilostazol: 651.8 days
Control: 569.7 days
Treatment duration:
Cilostazol: 632.2 (467.7) days Control: 695.1 (456.3) daysAtherothrombotic (14.1%), LACI (75.0%), mixed (9.0%) Atherothrombotic (13.1%), LACI (73.8%), mixed (11.4%) Guo 200925 1–6 months 12 months Han 2013 (ECLIPse)26 Within 7 days
Median: 5 days (78.3% of patients were randomised within 7 days)90 days LACI LACI Huang 2008 (CASISP)27 1–6 months
Cilostazol: 77.26 (50.05) days
Control: 79.72 (51.96) days12–18 months (average: 740 person-years) Johkura 201228 1–6 months 6 months Kim 2018 (PICASSO)*29 Within 180 days
Cilostazol: 18 days (IQR 8–40)
Control: 17 days (IQR 7–35)1.9 years (IQR 1.0–3.0) Ischaemic stroke (95%), TIA (5%) Ischaemic stroke (94%), TIA (6%) Kwon 2005 (TOSS)30 Within 2 weeks 6 months ICAS ICAS Kwon 2011 (TOSS-2)31 Within 2 weeks
Cilostazol: 8.03 (3.34) days
Control: 7.82 (3.15) days7 months ICAS ICAS Lee 2011 (CAIST)32 Within 48 hours
Cilostazol: 33 (12) hours
Control: 35 (11) hours90 days Large-artery disease (32%), small-vessel disease (55%), cardioembolism (1%), other determined aetiology (<1%), undetermined (12%) Large-artery disease (25%), small-vessel disease (62%), cardioembolism (1%), other determined aetiology (<1%), undetermined (12%) Lee 201733 Within 7 days 3 months Atherosclerosis (9.4%), small-artery disease (87.5%), TIA (3.1%) Atherosclerosis (2.9%), small-artery disease (87.5%), TIA (5.9%), unknown (8.8%) Nakamura 201234 Within 48 hours
Cilostazol: 25 (12) hours
Control: 23 (14) hours6 months Large-artery atherosclerosis (21%), small-vessel occlusion (47%), other determined or undetermined aetiology (32%) Large-artery atherosclerosis (18%), small-vessel occlusion (47%), other determined or undetermined aetiology (34%) Ohnuki 201735 Within 7 days 4 weeks Atherothrombosis (15%), LACI (62%), TIA (8%), unknown (15%) Atherothrombosis (45%), LACI (45%), TIA (9%) Shimizu 201336 Within 24 hours 3 months Atherothrombotic (30.7%), LACI (64.1%), others (5.2%) Atherothrombotic (25.0%), LACI (70.7%), others (4.3%) Shinohara 2010 (CSPS 2)37 Within 26 weeks (6 months) 1–5 years
Mean: 29 (16) monthsAtherothrombotic (33%), LACI (65%), others (3%) Atherothrombotic (31%), LACI (65%), others (3%) Toyoda 2019 (CSPS.com)†38 8–180 days
Cilostazol: 27 days (IQR 13–63)
Control: 25 days (IQR 13–64)0.5–3.5 years
Median: 1.4 (IQR 0.8–2.2)ICAS (30%), ECAS (12%)
Atherothrombotic (42%), LACI (50%), others/unknown (8%)ICAS (29%), ECAS (14%)
Atherothrombotic (42%), LACI (49%), others/unknown (9%)Uchiyama 2015 (CATHARSIS)39 2 weeks to 6 months 2 years
Mean: 762 daysICAS ICAS Data are in median (IQR), mean (range) or mean (SD) unless otherwise stated.
*Only patients with asymptomatic or previous intracerebral haemorrhage were included.
†Only patients with high-risk ischaemic stroke were included.
ICAS, intracranial arterial stenosis; LACI, lacunar infarction; TIA, transient ischaemic attack.
- Table 3
Summary of outcomes
Subgroup N Cilostazol Control RR (95% CI) P value I2 (%) Test for subgroup differences Ischaemic stroke recurrence A Overall 18 217/5724 317/5705 0.69 (0.58–0.81) <0.0001 0 NA B CIL SAPT vs SAPT 7 131/2844 168/2837 0.78 (0.62–0.97) 0.03 0 χ3 2=7.50, p=0.06, I2=60.0% CIL DAPT vs SAPT 8 43/1864 82/1853 0.52 (0.36–0.75) 0.0005 0 CIL DAPT vs DAPT 1 10/232 6/225 1.62 (0.60–4.37) 0.34 NA CIL vs No CIL 2 33/784 61/790 0.54 (0.36–0.82) 0.003 0 C Stroke onset <3 days 4 16/1120 24/1122 0.67 (0.36–1.25) 0.20 0 χ1 2=0.01, p=0.93, I2=0% Stroke onset >3 days 14 201/4604 293/4583 0.69 (0.56–0.84) 0.0002 8 D Short term (<3 months) 3 7/655 8/627 0.78 (0.29–2.12) 0.63 0 χ1 2=0.07, p=0.80, I2=0% Long term (≥3 months) 15 210/5069 309/5078 0.68 (0.58–0.81) <0.0001 0 E Symptomatic ICAS 3 14/382 12/373 1.10 (0.45–2.68) 0.84 24 χ2 2=1.33, p=0.52, I2=0% LACI 2 2/131 1/108 1.08 (0.14–8.56) 0.95 0 Others/mixed/unknown 13 201/5211 304/5224 0.67 (0.56–0.79) <0.00001 0 Any stroke recurrence A Overall 18 250/5724 394/5705 0.64 (0.54–0.74) <0.00001 0 NA B Stroke onset <3 days 4 20/1120 29/1122 0.70 (0.39–1.23) 0.21 0 χ1 2=0.11, p=0.75, I2=0% Stroke onset >3 days 14 230/4604 365/4583 0.63 (0.54–0.74) <0.00001 0 C Short term (<3 months) 3 9/655 9/627 0.91 (0.37–2.24) 0.83 0 χ1 2=0.61, p=0.43, I2=0% Long term (≥3 months) 15 241/5069 385/5078 0.63 (0.54–0.74) <0.00001 0 D Symptomatic ICAS 3 15/382 14/373 0.96 (0.27–3.45) 0.95 65 χ2 2=0.71, p=0.70, I2=0% LACI 2 2/131 1/108 1.08 (0.14–8.56) 0.95 0 Others/mixed/unknown 13 233/5211 379/5224 0.62 (0.53–0.73) <0.00001 0 Intracranial haemorrhage A Overall 18 37/5724 86/5705 0.46 (0.31–0.68) <0.0001 0 NA B Stroke onset <3 days 4 4/1120 5/1122 0.91 (0.24–3.53) 0.89 0 χ1 2=1.05, p=0.31, I2=4.8% Stroke onset >3 days 14 33/4604 81/4583 0.43 (0.29–0.65) <0.0001 0 C Short term (<3 months) 3 2/655 1/627 2.00 (0.18–22.03) 0.57 NA χ1 2=1.48, p=0.22, I2=32.3% Long term (≥3 months) 15 35/5069 85/5078 0.44 (0.30–0.66) <0.0001 0 D Symptomatic ICAS 3 1/382 3/373 0.46 (0.06–3.57) 0.46 0 χ1 2=0.00, p=1.00, I2=0% LACI 2 0/131 0/108 NA NA NA Others/mixed/unknown 13 36/5211 83/5224 0.46 (0.31–0.68) 0.0001 0 Major haemorrhagic events A Overall 14 44/4031 93/4010 0.49 (0.34–0.70) <0.0001 0 NA B Stroke onset <3 days 4 7/1120 13/1122 0.60 (0.24–1.52) 0.28 0 χ1 2=0.23, p=0.63, I2=0% Stroke onset >3 days 10 37/2911 80/2888 0.47 (0.32–0.69) 0.0001 0 C Short term (<3 months) 3 4/655 5/627 0.80 (0.22–2.97) 0.74 NA χ1 2=0.59, p=0.44, I2=0% Long term (≥3 months) 11 40/3376 88/3383 0.47 (0.32–0.68) <0.0001 0 D Symptomatic ICAS 3 6/382 9/373 0.67 (0.17–2.59) 0.56 37 χ1 2=0.24, p=0.62, I2=0% LACI 2 0/131 0/108 NA NA NA Others/mixed/unknown 9 38/3518 84/3529 0.47 (0.32–0.68) <0.0001 0 Mortality A Overall 15 64/5029 72/5017 0.90 (0.64–1.25) 0.53 0 NA B Stroke onset <3 days 2 3/482 1/483 2.33 (0.34–15.82) 0.39 0 χ1 2=0.98, p=0.32, I2=0% Stroke onset >3 days 13 61/4547 71/4534 0.87 (0.62–1.22) 0.43 0 C Short term (<3 months) 2 0/55 0/26 NA NA NA NA Long term (≥3 months) 13 64/4974 72/4991 0.90 (0.64–1.25) 0.53 0 D Symptomatic ICAS 3 2/382 3/373 0.67 (0.11–4.06) 0.66 0 χ1 2=0.11, p=0.74, I2=0% LACI 2 0/131 0/108 NA NA NA Others/mixed/unknown 10 62/4516 69/4536 0.91 (0.65–1.27) 0.58 0 MACE A Overall 13 184/3826 276/3842 0.67 (0.56–0.81) <0.0001 0 NA B Stroke onset <3 days 4 25/1120 33/1122 0.76 (0.45–1.27) 0.30 0 χ1 2=0.18, p=0.67, I2=0% Stroke onset >3 days 9 159/2706 243/2720 0.67 (0.52–0.86) 0.002 20 C Short term (<3 months) 2 12/613 12/612 1.00 (0.45–2.21) 1.00 NA χ1 2=1.03, p=0.31, I2=3.0% Long term (≥3 months) 11 172/3213 264/3230 0.66 (0.55–0.79) <0.0001 0 D Symptomatic ICAS 2 17/299 12/293 1.38 (0.67–2.85) 0.38 0 χ2 2=4.22, p=0.12, I2=52.6% LACI 1 1/89 1/93 1.04 (0.07–16.45) 0.98 NA Others/mixed/unknown 10 166/3438 263/3456 0.64 (0.53–0.77) <0.00001 0 CIL, cilostazol; DAPT, dual antiplatelet therapy; ICAS, intracranial arterial stenosis; LACI, lacunar infarction; No CIL, placebo or best medical therapy; RR, risk ratio; SAPT, single antiplatelet therapy.
Supplementary Materials
Supplementary data
Additional Files
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}