

Abstract
Objectives To establish a new ambulatory blood pressure (ABP) parameter (24-hour ABP profile) and evaluated its performance on stroke outcome in ischaemic stroke (IS) or transient ischaemic attack (TIA) patients.
Methods The prospective cohort consisted of 1996 IS/TIA patients enrolled for ABP monitoring and a 3-month follow-up for stroke recurrence as outcome. Profile groups of systolic blood pressure (SBP) were identified via an advanced functional clustering method, and the associations of the profile groups and conventional ABP parameters with stroke recurrence were examined in a Cox proportional hazards model.
Results Three discrete profile groups (n=604, 781 and 611 in profiles 1, 2 and 3, respectively) in 24-hour ambulatory SBP were identified. Profile 1 resembled most to the normal diurnal blood pressure pattern; profile 2 also dropped at night, but climbed earlier and with higher morning surge; while profile 3 had sustained higher nocturnal SBP without significant nocturnal SBP decline. The incidence of stroke recurrence was 2.9%, 3.9% and 5.5% in profiles 1, 2 and 3, respectively. After adjustment for covariates, profile 3 was significantly associated with higher risk of stroke recurrence with profile 1 as reference (HR 1.76, 95% CI: 1.00 to 3.09), while no significant difference was observed between profiles 2 and 1 (HR 1.22, 95% CI: 0.66 to 2.25). None of conventional ABP parameters showed significant associations with the outcome.
Conclusions Ambulatory 24-hour SBP profile is associated with short-term stroke recurrence. Profiles of ABP may help improve identification of stroke recurrence by capturing the additive effects of individual ABP parameters.
Introduction
Hypertension has been identified as the first leading modifiable risk factor for stroke.1 2 It is widely accepted that 24-hour ambulatory blood pressure (ABP) monitoring is superior to clinic and self-measurement of blood pressure (BP) in the diagnosis and prognosis of hypertension and risk assessment of cardiovascular and cerebrovascular disease.3 The conventional ABP parameters includes 24-hour mean BP, daytime and night-time BP, dipping status, morning surge (MS), nocturnal hypertension, BP variability (BPV) et al.4 Extensive studies have shown that above conventional ABP parameters are associated with stroke3 5–16 and its clinical outcome.17–21 However, individual ABP parameter might only represent a specific characteristic of the whole ABP profiles, and different parameter play distinct role on stroke prognosis. For example, disturbed dipping status, especially reverse dippers, the long-lasting high BP level could cause impairment of the arterial wall structure and endothelium leading to acceleration of vascular remodelling and atherosclerosis of the artery, which promote subsequent stroke events.22 An exaggerated morning BP surge could induce plaque instability through increased inflammatory reaction and leading to plaque rupture triggered by increased mechanical pressure and shear stress of an exaggerated fluctuation of blood flow on the vessel wall.23 24
Moreover, despite extensive existing data on individual ABP parameters in relation to the risk of developing stroke, the literature is relatively limited regarding the association between ABP profiles and stroke outcome. Most previous studies that focused on analyses of individual ABP parameters neglected the temporal nature of the 24-hour ABP data and the additive effects of multiple ABP characteristics. Profile analysis of 24-hour ABP, incorporating all the ABP parameters with the minimum information lost, may be better for evaluating its performance on stroke outcome. A piecewise linear random effects model has been recently proposed to identify 24-hour ABP profile clusters25; however, this model has not been used for clinical evaluation of stroke patients. In this study, we aimed to identify clusters of stroke patients with similar ABP profile patterns, characterise the circadian rhythm parameters in the profile groups and examine the association of 24-hour ABP profiles with the clinical outcome measured as stroke recurrence.
Methods
Study cohort
The Blood pressure and clinical Outcome in Stroke Survivors study is a nationwide, hospital-based, longitudinal, prospective cohort study conducted in 61 hospitals in China. Details of the design, rationale and baseline characteristics were described previously.26 In brief, 2608 patients of acute ischaemic stroke (IS) and transient ischaemic attack (TIA) within 7 days of the index event, aged 18 years or older, were enrolled from October 2012 to February 2014 at baseline for ABP monitoring (ABPM) and followed for 3 months for stroke recurrence as outcome. In this study cohort, 199 patients with incomplete baseline data and 376 patients with incomplete ABP data were excluded, and 37 patients were lost to follow-up. A total of 1996 patients formed the current study cohort.
From January 2015 to December 2015, a total of 746 patients with IS were enrolled for ABPM in Neurology Department of Beijing Tiantan Hospital, Capital Medical University. These patients who did not have information on the clinical outcome were used as a validation cohort for the ABP profile cluster analysis. In this validation cohort (mean age=56.1±12.7 years, 28.3% female), 41.9% had a history of hypertension and a median of National Institute of Health Stroke Scale of 3 with an IQR of 1–8.
The study was approved by the central Institutional Review Board at Beijing Tiantan Hospital. All patients or the designated relatives gave written consent when enrolled.
BP measurements
For stroke patients, to avoid BP elevation during the stress period after stroke onset, 24-hour ABPM was completed within 3–14 days after the index event; however, for TIA patients, because TIA does not generally cause stress hypertension, ABPM could be evaluated from onset to 14 days. The frequency of measurements was set every 15 min during daytime and every 30 min during night-time. Daytime was defined from 06:00 to 21:59 and night-time from 22:00 to 05:59. If the recorded BP readings were less than 80% of expected measurements, the ABPM should be repeated. Participants were instructed to keep a diary of their daily activities during the measurements.
Definition of the conventional ABP parameters
In this study, all ABP parameters were calculated based on systolic blood pressure (SBP).6 The percentage of nocturnal decline in SBP was calculated as ((daytime SBP−night-time SBP)/daytime SBP)×100%. Daytime and night-time SBP was defined as the mean SBP during daytime and night-time episodes. Night-time dipping was classified as follows: extreme dipper (nocturnal decline ≥20%), dipper (10%≤nocturnal decline <20%), non-dipper (0%≤nocturnal decline <10%) and reverse dipper (nocturnal decline <0%). Morning SBP was defined as the average of SBP readings during the first 2 hours of the daytime (06:00 to 08:00). The sleep-trough (ST) SBP was defined as the lowest SBP during night-time. MS was defined as ST-MS calculated by the morning SBP minus the ST SBP. SBP variability was evaluated by coefficient of variation defined as 100×SD/mean SBP.
Clinical outcomes
Patients were followed up for clinical outcomes at 3 months through face-to-face interview and at 12 months by telephone. Follow-up through telephone or face to face was conducted by trained site coordinators. In this study, the clinical outcome was stroke recurrence during the 3 months. Stroke recurrence was defined as a new stroke event (ischaemic or haemorrhagic stroke). If stroke event occurred before ABPM, it would not be included in the statistical analysis.
Statistical analysis
The functional clustering method was implemented to group the cluster of BP profiles. To facilitate the computation, we preprocessed the ABP readings so that the measurement times are equally spaced on the 15-min grids. The detailed preprocessing steps were described in Section S.2.1 in the online supplemental material. We treated each resulting BP curve as a function of time and assumed that the profiles in the same cluster share the same mean value. Then we used the Fourier expansion in combination with the iterative k-centres clustering method.27 Essentially, the algorithm was developed to minimise the errors between observed curves and their cluster sample means. Since wrong clustering would lead to larger errors than the true one did, the minimisation algorithm forced the estimated clusters approaching the underlying truth when the sample size increased. The technical details are presented in Section S.2.2 in the online supplemental material.
Supplementary data
The associations of ambulatory SBP parameters and profiles with the clinical outcome were then examined using a Cox proportional hazards model with adjustment for confounding variables. All statistical analyses were performed with SAS V.9.4 (SAS Institute Inc). A two-sided p<0.05 was considered statistically significant.
Results
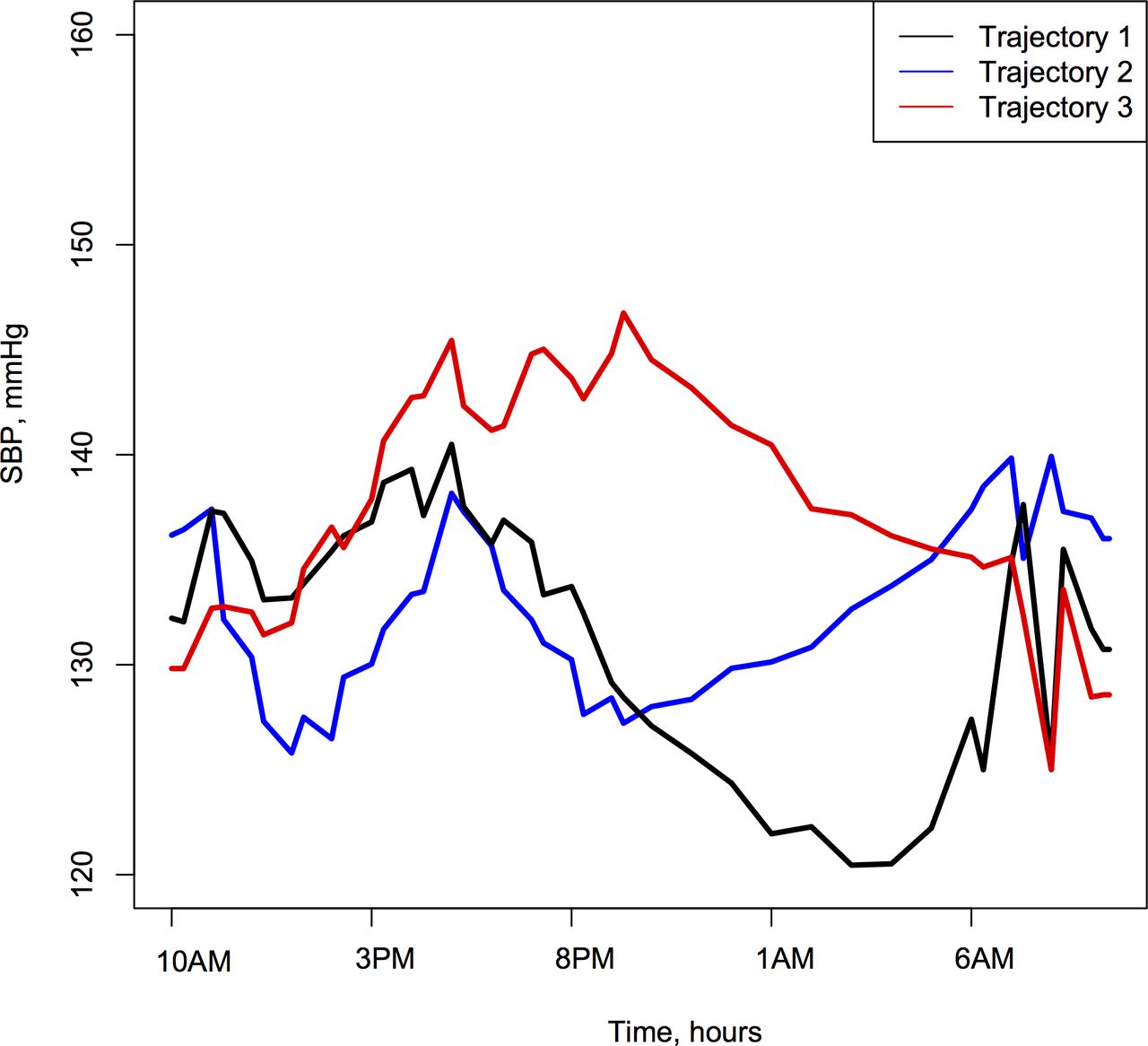
Three discrete profile groups in 24-hour ambulatory SBP were identified using functional clustering method (figure 1). Profile 1 (n=781) resembled most to the normal diurnal BP pattern; profile 2 (n=611) also dropped at night, but climbed earlier (the trough SBP was seen around 04:00 in profile 1 and around 24:00 in profile 2) and with higher MS; while profile 3 (n=604) had sustained higher nocturnal SBP without significant nocturnal SBP decline. Moreover, differences in daytime SBP were not as big as those in night-time SBP between the three groups. The validation cohort produced considerably similar profile patterns of SBP, especially at night-time (figure 2).

Ambulatory systolic blood pressure (SBP) profiles in the three cluster groups.

Ambulatory systolic blood pressure (SBP) profiles in the three cluster groups of the validation cohort.
The characteristics in the total cohort of 1996 patients and by three profile groups were shown in table 1. The mean age was 62.7±10.9 years; 32.9% were females; 88.2% was IS patients in the total cohort. Patients in profile groups 2 and 3 were older and had more coronary heart disease than those in group 1. Group 2 had less alcohol drinkers than group 1. Group 3 had less dyslipidaemia than group 1. More patients in group 3 (71.4%) took antihypertensive therapy at discharge than those in group 1 (65.4%). Other characteristics did not differ significantly between the three profile groups. Comparison of characteristics between the included and excluded patients is given in online supplemental table S1.
Characteristics of the participants by profile groups
Table 2 presents ambulatory SBP parameters of all participants and by profile groups. Daytime, night-time, morning and trough SBP, and ST-MS showed significant differences between groups in different directions. 24-hour SBP variability did not differ significantly between groups. Compared with group 1, groups 2 and 3 had significantly less dippers and more non-dippers and reverse dippers. Group 3 had the highest incidence of stroke recurrence (5.5%).
Ambulatory SBP parameters of the participants by profile groups
In table 3, profile patterns, mean 24-hour SBP, night-time SBP, morning SBP and trough SBP were found to be significantly associated with 3-month stroke recurrence without adjustment for covariates. However, after adjustment for age, sex, risk factors and secondary prevention medication in model 2 and with additional adjustment for mean 24-hours SBP in model 3, profile group 3 was still significantly associated with stroke recurrence with group 1 as reference; but other associations became non-significant.
HR of SBP parameters for 3-month stroke recurrence
Finally, table 4 shows ambulatory SBP parameters by profile groups in the validation cohort. Differences in mean 24-hour SBP, daytime SBP, night-time SBP, morning SBP, trough SBP, ST-MS, 24-hour SBP variability and night-time dipping patterns were very similar to those as shown in table 2.
Ambulatory blood pressure parameters by profile groups in the validation cohort
Discussion
In the present study, we characterised the 24-hour ABP profiles in 1996 IS and TIA patients using a novel functional clustering method, in relation to stroke recurrence as the outcome. Three different profile groups in ABP were identified. The most characteristic cluster was the patients in group 3 who had significantly higher nocturnal SBP than those in group 1. The validation cohort produced a substantially similar profile pattern. The incidence of stroke recurrence was significantly higher in group 3 (5.5%) than in group 1 (2.9%). The ABP profile cluster of group 3 was significantly associated with a higher risk of stroke recurrence; but individual ABP parameters did not show significant associations with the outcome after adjustment for covariates. These findings support the notion that the profile cluster is a more strongly associated with the clinical outcome of stroke patients by capturing the additive effects of individual ABP parameters.
ABPM that continuously monitors changes in BP during daytime and night-time can generate a large number of readings with multiple characteristics of BP.28 Extensive studies have demonstrated that higher MS, non-dipping and reverse dipping and increased diurnal levels and variability of BP are associated with the risk of developing stroke.3 5–11 However, the literature relating these ABP parameters to clinical outcomes of stroke patients remained relatively limited, and the results were inconsistent.17–19 29 30 In the current study, we did not find conventional ABP parameters to be significantly associated with the 3-month stroke recurrence after adjustment for covariates. The observations from this and previous studies suggest that individual ABP parameters might have a limited statistical power to predict stroke recurrence of stroke patients. Previous studies of ABP focused analysis of single readings ignored the temporal nature of the data. Advanced statistical techniques that incorporate the information of multiple ABP characteristics may help improve comprehensive BP assessment for stroke patients.
BP as an important cardiovascular function parameter displays a circadian rhythm, with clear day–night variability in a 24-hour cycle controlled by the central circadian clock.31 The profile of diurnal changes in BP is constituted by 24-hour BP levels, variability and circadian rhythms. The trajectory patterns of short-term and long-term visit-to-visit BP have been established and have shown to be associated with cardiovascular events.32 Recently, a piecewise linear random effects model has been proposed to identify 24-hour ABP trajectory groups25; however, this model has not been applied for prediction of stroke outcomes. In the present study, we developed a novel profile clustering method, and three distinct ABP profile groups were identified. Stroke patients in group 3 who had sustained higher nocturnal SBP compared with those in group 1 showed an increased risk of stroke recurrence. However, when individual ABP parameters were analysed separately with adjustment for covariates, none of them was significantly associated with stroke recurrence. These findings suggest that our novel profile clustering approach is superior to the traditional analysis of individual ABP parameters in relation to stroke outcome.
Elevated nocturnal BP or non-dippers at night have long been recognised as a strong predictor of cardiovascular and cerebrovascular disease in numerous clinical and epidemiologic studies.8 33–36 The current study aimed to assess the predictive value of the ABP profile patterns as well as individual BP parameters for stroke recurrence. The most characteristic feature of the profile pattern of group 3 classified in this study was significantly lower daytime SBP and increased nocturnal SBP with 68.1% reverse dippers. It is obvious that the association between the profile pattern of group 3 and stroke recurrence was mainly driven by the consistently higher night-time SBP levels. However, it is worthy to be noted that night-time SBP, ST SBP, non-dippers and reverse dippers at night did not significantly predict the risk of stroke recurrence after adjusting for confounding variables. Our results suggest an idea that the significant association between circadian BP profile patterns and stroke recurrence depends on not only the elevated nocturnal BP but also other ABP parameters with weak additive effects.
Another important finding was that MS may not have enough predictive power for stroke recurrence. Our result showed that profile 2 with higher MS did not have significant higher risk of stroke recurrence compared with profile 1. Moreover, the amplitude of MS of profile 3, which had the highest risk of stroke recurrence was lowest among three profiles. In fact, previous studies concerning the predictive value of MS for stroke also showed conflicting results.37–39 And some study revealed that the reverse dippers were associated with blunted MS, so it is reverse dippers but not the accompanying blunted MS accounting for stroke risk.40 This, in other hand, emphasise the importance of the elevated night-time BP (NBP) on stroke prognosis rather than MS. While, previous study also reported that the prognostic predictive value of MS could only be found in the dippers rather than non-dippers.8 Considering the high prevalence of non-dippers in the three profiles, MS might have little effect on stroke risk prediction. Higher NBP might partly explained the higher stroke risk of profile 2 in contrast to profile 1, although the difference was insignificant. It could be due to the relatively small difference between the NBPs of the two profiles, and larger samples might be needed.
Our study had some limitations. First, there may be enrolment bias in our study population, which have more mild stroke patients, and low proportion of atrial fibrillation enrolled. Therefore, our findings may not be generalisable to all stroke patients. Second, the number of patients included in this study seemed to be low to justify the lack of prognostic value of conventional individual ABP parameters (dipping pattern, MS, etc). Third, follow-up data were unavailable in the validation group, we could not examin the prognostic significance of the new obtained profile.
Conclusions
Of note, night-time SBP, ST SBP, non-dippers and reverse dippers at night did not significantly predict the risk of stroke recurrence after adjusting for covariates. These results suggest that ambulatory 24-hour SBP profile pattern is more strongly associated with short-term stroke recurrence in stroke patients compared with individual ABP parameters. Profile patterns of ABP may help improve identification of stroke patients at a high risk of adverse clinical outcomes by capturing the additive effects of individual ABP parameters.
Data availability statement
Data are available upon reasonable request. All data are available to researchers on request for purposes of reproducing the results or replicating the procedure by directly contacting the corresponding author.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors were involved in the interpretation of study results and approval of the final version of the manuscript. YW had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. JX, HS and YW contributed to the study concept and design. JX, JM and ZC contributed to the drafting of the manuscript. FJ, HZ, YG and JT contributed to the acquisition of data. AW, HS, TZ and WC contributed to statistical analysis. AX, BL, BH, YZ, XZ, YW and HL contributed to critical revision of the manuscript for important intellectual content.
Funding This study was funded by National Natural Science Foundation of China, Beijing Municipal Science & Technology Commission, China Postdoctoral Science Foundation, National Science and Technology Major Project, Young Scientist Program of Beijing Tiantan hospital and National Key R&D Program of China.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}