

Article Figures & Data
Figures
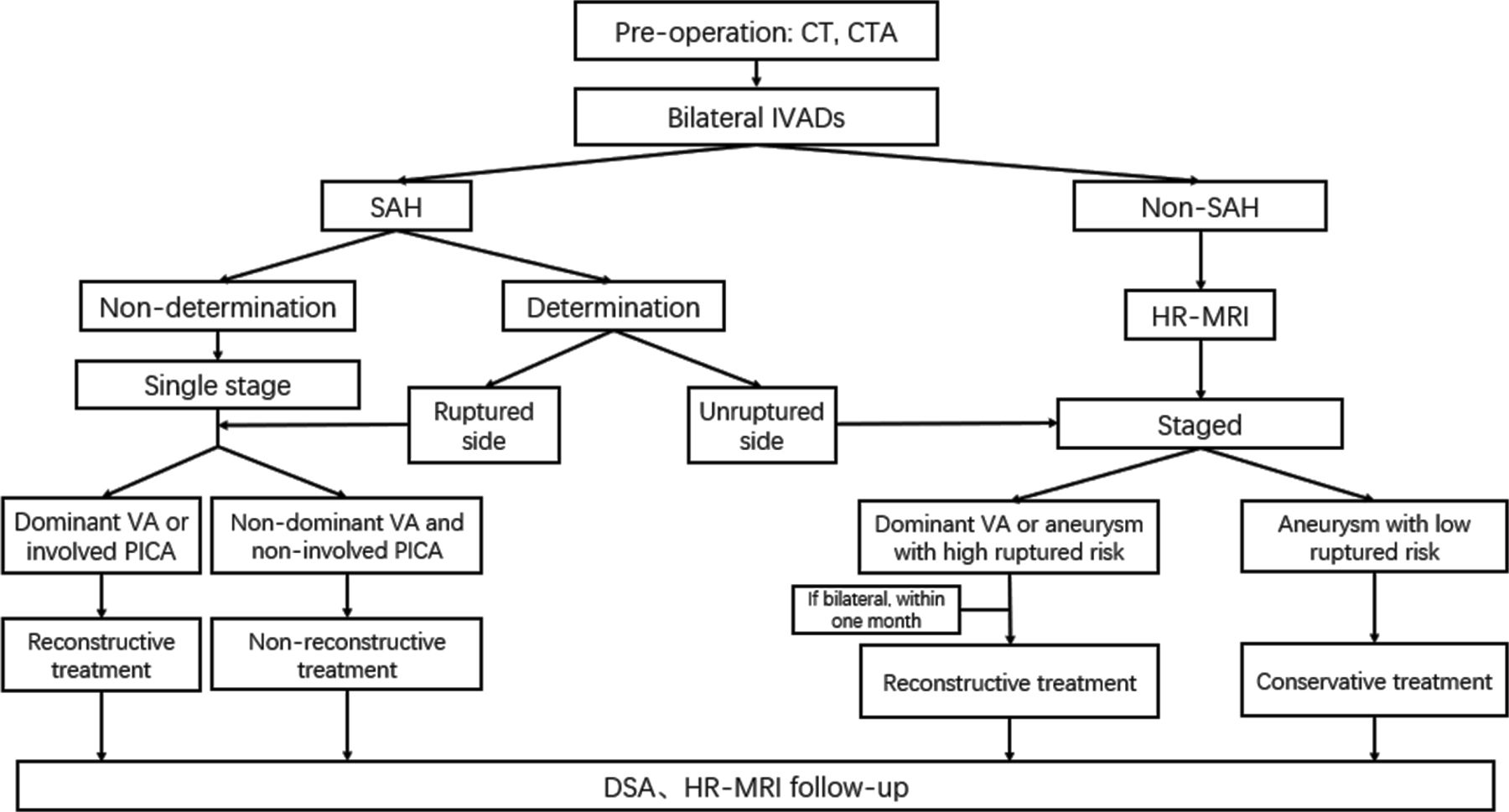
- Figure 1
Algorithm showing endovascular treatment protocol for bilateral IVADAs. CTA, CT angiography; DSA, digital subtraction angiography; HR-MRI, high-resolution MRI; IVADAs, intracranial vertebral artery dissecting aneurysms; ; PICA, posterior inferior cerebellar artery; SAH, subarachnoid haemorrhage; VA, vertebral artery.
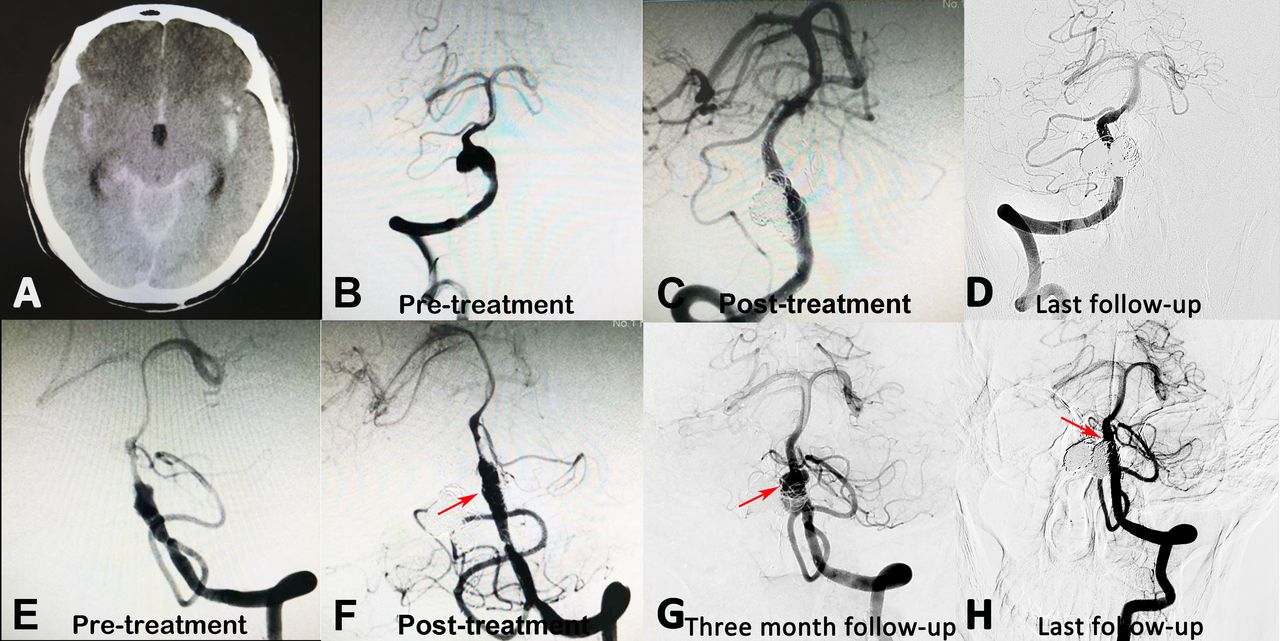
- Figure 2
(A) A patient showing subarachnoid haemorrhage on CT imaging. (B and E) Digital subtraction angiography showed bilateral IVADAs. The ruptured side could not be determined based on the CT scan. (C and F) Thus, for this ruptured patient, both aneurysms were treated with stent-assisted coil embolisation at one stage, and a near-complete obliteration was achieved. (G) At the 3-month follow-up, the left IVADA recanalised, and the right IVADA was stable. The recanalised IVADA was further retreated with recoiling. (D and H) Both IVADAs were stable at the last follow-up angiography. IVADAs, intracranial vertebral artery dissecting aneurysms.
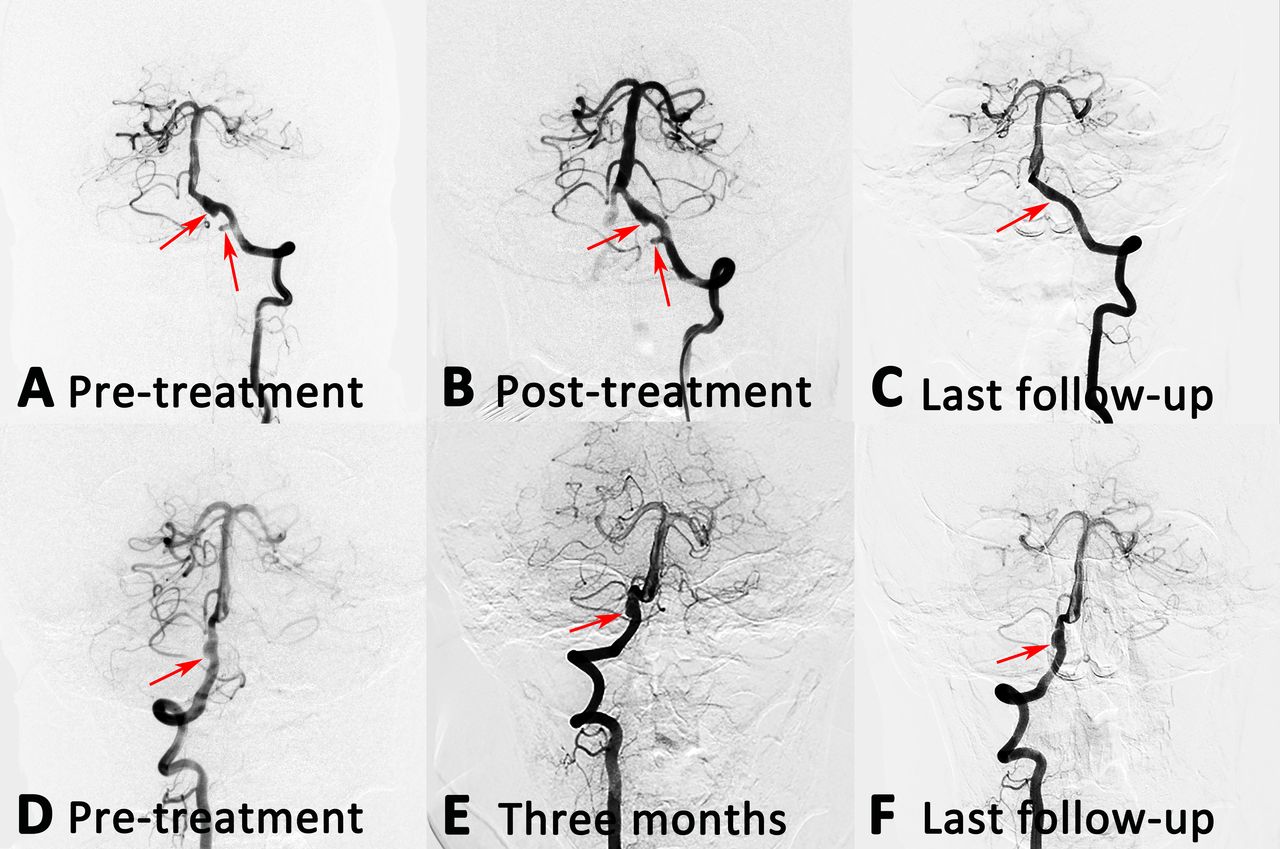
- Figure 3
(A and D) An unruptured patient with bilateral IVADAs. This patient received a two-stage treatment. (E) At the first stage, the right aneurysm was treated with PED alone, and partial obliteration was achieved immediately. (F) Three months later, the right aneurysm was completely obliterated, while no compensatory blood flow was supplied to the left vertebral artery. (B) At the same time, the left aneurysm was also treated with PED alone, and partial obliteration was achieved immediately. (G) At the last follow-up DSA, the right aneurysm remained stable. The left posterior inferior cerebellar artery received compensatory blood flow from the right vertebral artery, while the left parent artery disappeared (C). No clinical symptoms were found. DSA, digital subtraction angiography; IVADAs, intracranial vertebral artery dissecting aneurysms; PED, Pipeline Embolization Device.
- Figure 4
(A and D) A patient with bilateral IVADAs, who was treated only one side. (B) The left aneurysm was treated with PED alone, and partial obliteration was achieved immediately. (E) Three months later, the right aneurysm remained stable. (C and F) At the last follow-up angiography, the left aneurysm was completely obliterated, and the right aneurysm remained stable. IVADAs, intracranial vertebral artery dissecting aneurysms; PED, Pipeline Embolization Device.




Tables
- Table 1
Clinical and radiographic characteristics of bilateral IVADAs with single-stage endovascular treatment
Case no. Presentation Side, PICA-involving, ruptured Configuration H-H Admission mRS score Treatment Immediate angiography* Complication (days) Follow-up angiography* (months) Last mRS
score (months)1 Acute headache R, involving, not determined
L, involving, not determinedPearl and string sign
FusiformⅡ 4 SAC
SACNear-complete obliteration
Near-complete obliteration– Recanalisation (3)→recoiling→ stable (6)
Complete obliteration (3)1 (6) 2 Headache L, no involving, unruptured
R, no involving, unrupturedPearl and string sign
Fusiform– 1 SAC
TrappingNear-complete obliteration
Complete obliterationMuscle weakness of left limbs (3 days) Complete obliteration (6)
Complete obliteration (6)3 (48) 3 Dizziness R, no involving, unruptured
L, no involving, unrupturedPearl and string sign
Pearl and string sign– 1 SAC
SACComplete obliteration
Complete obliterationSudden unconsciousness (2 months) Complete obliteration (2)
Complete obliteration (2)3 (36) 4 Incidence R, no involving, unruptured
L, no involving, unrupturedPearl and string sign
Fusiform– 0 SAC
Stent aloneComplete obliteration
Partial obliteration– Complete obliteration (6)
Complete obliteration (6)1 (30) *Angiography results are classified as follows: stable, no interval changes of the dissecting aneurysm in size or shape; complete obliteration, complete occlusion of the dissecting aneurysm sac with reconstruction of the parent artery; near-complete obliteration, neck remnant of the dissecting aneurysm.
H-H, Hunt-Hess; IVADAs, intracranial vertebral artery dissecting aneurysms; L, left; mRS, modified Rankin Scale; PICA, posterior inferior cerebellar artery; R, right; SAC, stent-assisted coiling.
- Table 2
Clinical and radiographic characteristics of bilateral IVADAs with staged endovascular treatment
Case no. Presentation Side, PICA-involving, ruptured Configuration H-H Admission mRS score First treatment Interval time (months) Second treatment Last mRS score (months) Side, treatment Immediate angiography* Follow-up angiography* (months) Complication Side, treatment Immediate angiography* Follow-up angiography* Complication (months) 1 Acute headache R, involving, ruptured
L, no involving, unrupturedPearl and string sign
Pearl and string signⅡ 4 R, SAC Near-complete obliteration Recanalisation (1)→recoiling→stable (7) – 1 L, SAC Near-complete obliteration Complete obliteration (6) – 1 (7) 2 Headache L, no involving, unruptured
R, no involving, unrupturedFusiform
Pearl and string sign– 1 R, SAC Near-complete obliteration Complete obliteration (3) – 3 L, SAC Complete obliteration Complete obliteration (6) – 0 (9) 3 Numbness of limbs L, no involving, unruptured
R, no involving, unrupturedFusiform
Fusiform– 2 L, stent alone Partial obliteration Complete obliteration (9) – 3 R, stent alone Partial obliteration Complete obliteration (6) – 1 (9) 4 Incidence L, no involving, unruptured
R, no involving, unrupturedPearl and string sign
Pearl and string sign– 0 R, SAC Complete obliteration Complete obliteration (9) – 3 L, SAC Complete obliteration Complete obliteration (6) – 0 (9) 5 Headache L, no involving, unruptured
R, no involving, unrupturedPearl and string sign
Fusiform– 1 L, SAC Complete obliteration Complete obliteration (10) – 3 R, SAC Near-complete obliteration Complete obliteration (7) – 0 (9) 6 Headache L, involving, unruptured
R, involving, unrupturedFusiform
Fusiform– 1 L, stent alone Partial obliteration Near-complete obliteration (1) – 1 R, stent alone Partial obliteration Stable (3) – 0 (9) 7 Dizziness L, involving, unruptured
R, involving, unrupturedFusiform
Fusiform– 2 R, stent alone Partial obliteration Complete obliteration (6) – 3 L, stent alone Partial obliteration Stable (3) – 0 (6) 8 Headache R, involving, unruptured
L, involving, unrupturedFusiform
Fusiform– 1 L, PED alone Partial obliteration Complete obliteration (6) – 2.5 R, PED alone Partial obliteration Complete obliteration (3.5) – 0 (6) 9 Dizziness R, involving, unruptured
L, involving, unrupturedPearl and string sign
Fusiform– 1 L, PED alone Partial obliteration Complete obliteration (9) – 2 R, PED alone Partial obliteration Complete obliteration (7) – 0 (9) 10 Dizziness R, involving, unruptured
L, involving, unrupturedPearl and string sign
Fusiform– 1 R, PED alone Partial obliteration Complete obliteration (9) – 3 L, PED alone Partial obliteration Complete obliteration (6) Parent artery occlusion (6) 0 (9) 11 Headache R, no involving, unruptured
L, no involving, unrupturedPearl and string sign
Fusiform– 1 R, SAC Complete obliteration Complete obliteration (7) – 2 L, PED alone Partial obliteration Complete obliteration (6) – 0 (8) 12 Headache R, no involving, unruptured
L, involving, unrupturedFusiform
Fusiform– 1 R, PED alone Partial obliteration Complete obliteration (7) – 1 L, PED alone Partial obliteration Complete obliteration (6) – 0 (7) *Angiography results are classified as follows: stable, no interval changes of the dissecting aneurysm in size or shape; complete obliteration, complete occlusion of the dissecting aneurysm sac with reconstruction of the parent artery; near-complete obliteration, neck remnant of the dissecting aneurysm; partial resolution, any opacification of the dissecting aneurysm sac.
H-H, Hunt-Hess; IVADAs, intracranial vertebral artery dissecting aneurysms; L, left; mRS, modified Rankin Scale; PED, Pipeline Embolization Device; PICA, posterior inferior cerebellar artery; R, right; SAC, stent-assisted coiling.
- Table 3
Clinical and radiographic characteristics of bilateral IVADAs with unilateral endovascular treatment
Case no. Presentation Side, PICA-involving, ruptured Configuration H-H Admission mRS score Treatment Immediate angiography* Complication Follow-up angiography* (months) Last mRS
score (months)1 Dizziness L, no involving, unruptured
R, no involving, unrupturedPearl and string sign
Fusiform– 1 SAC
–Near-complete obliteration
–– Complete obliteration (6)
Stable (6)0 (6) 2 Headache L, no involving, unruptured
R, no involving, unrupturedPearl and string sign
Fusiform– 2 SAC
–Near-complete obliteration
–– Complete obliteration (8)
Stable (6)0 (8) 3 Headache L, no involving, unruptured
R, no involving, rupturedFusiform
Pearl and string signⅠ 3 –
SAC–
Near-complete obliteration– Stable (3)
Stable (3)0 (6) 4 Dizziness L, no involving, unruptured
R, involving, unrupturedPearl and string sign
Pearl and string sign– 1 –
SAC–
Near-complete obliteration– NA 0 (6) 5 Dizziness L, no involving, unruptured
R, no involving, unrupturedFusiform
Pearl and string sign– 1 –
SAC–
Near-complete obliteration– Stable (6)
Complete obliteration (6)0 (6) 6 Dizziness L, no involving, unruptured
R, no involving, unrupturedPearl and string sign
Fusiform– 1 SAC
–Complete obliteration
–– Complete obliteration (6)
Stable (6)0 (3) 7 Incidence L, no involving, unruptured
R, no involving, unrupturedFusiform
Fusiform– 0 SAC
–Complete obliteration
–– Complete obliteration (6)
Stable (6)0 (6) 8 Incidence L, involving, unruptured
R, no involving, unrupturedFusiform
Pearl and string sign– 0 PED alone
–Partial obliteration
–– Complete obliteration (3)
Stable (3)0 (3) 9 Incidence L, involving, unruptured
R, no involving, unrupturedFusiform
Fusiform– 0 PED alone
–Partial obliteration
–– Complete obliteration (6)
Stable (6)0 (6) 10 Incidence L, no involving, unruptured
R, involving, unrupturedFusiform
Fusiform– 0 –
PED alone–
Partial obliteration– Stable (6)
Complete obliteration (6)0 (6) 11 Dizziness L, no involving, unruptured
R, no involving, unrupturedFusiform
Fusiform– 0 PED alone
–Partial obliteration
–– Complete obliteration (5)
Stable (5)0 (5) *Angiography results are classified as follows: stable, no interval changes of the dissecting aneurysm in size or shape; complete obliteration, complete occlusion of the dissecting aneurysm sac with reconstruction of the parent artery; near-complete obliteration, neck remnant of the dissecting aneurysm, partial resolution, any opacification of the dissecting aneurysm sac.
H-H, Hunt-Hess; IVADAs, intracranial vertebral artery dissecting aneurysms; L, left; mRS, modified Rankin Scale; NA, not applicable; PED, Pipeline Embolization Device; PICA, posterior inferior cerebellar artery; R, right; SAC, stent-assisted coiling.
- Table 4
Comparison of the unruptured IVADAs with three different treatments
Variables Single-stage treatment
(A), n=6Staged treatment
(B), n=22P value (A vs B) One side treatment
(C), n=20P value (A vs C) P value (B vs C) Admission mRS score 0.67±0.58 1.09±0.54 0.24 0.60±0.70 0.78 0.07 Treatment method 0.05 0.01* <0.01* Conservative 0 (0) 0 (0) 10 (50.0) Trapping 1 (16.7) 0 (0) 0 (0) SAC 4 (66.7) 7 (31.8) 6 (30.0) Stent alone 1 (16.7) 6 (27.3) 0 (0) Flow diverter 0 (0) 9 (40.9) 4 (20.0) Thromboembolic complications 2 of 3 (66.7) 0 of 11 (0) <0.01* 0 of 10 (0) <0.01* – Immediate angiography 0.07 0.18 0.11 Partial obliteration 1 (16.7) 15 (68.2) 4 (40.0) Near-complete obliteration 1 (16.7) 2 (9.1) 4 (40.0) Complete obliteration 4 (66.7) 5 (22.7) 2 (20.0) Follow-up angiography 0.12 0.81 0.06 Improve 2 (33.3) 15 (68.2) 7 (38.9) Stable 4 (66.7) 7 (31.8) 11 (61.1) * Recanalisation 0 (0) 0 (0) 0 (0) Last mRS score 2.33±1.16 0.09±0.30 <0.01* 0±0 <0.01* 0.34 *One patient with bilateral IVADs had no follow-up.
IVADAs, intracranial vertebral artery dissecting aneurysms; mRS, modified Rankin Scale; SAC, stent-assisted coiling.





{kind=link}
{kind=link}
{kind=link}
{kind=link}