

Abstract
Objective Gastrointestinal (GI) bleeding in patients who had a stroke is strongly associated with a higher risk of death and loss of independence. However, it is unknown whether GI bleeding increases risk for recurrence of stroke. In this study, we assess the potential relationship between GI bleeding and stroke recurrence in patients within 12 months of an acute ischaemic stroke (AIS), using the China National Stroke Registry (CNSR).
Methods This study included 22 216 patients who had an ischaemic stroke included in the CNSR from 2007 to 2008. We analysed baseline patient characteristics, GI bleeding and outcomes of patients who had an AIS, specifically stroke recurrence at 3, 6 and 12 months. We used multivariable logistic regression to evaluate a possible association between GI bleeding and stroke recurrence.
Results Of the 12 415 patients included in our study, 12.3%, 15.5% and 17.7% had a stroke recurrence at 3, 6 and 12 months, respectively. GI bleeding was an independent stroke recurrence risk factor in patients after ischaemic stroke at 3 months (adjusted OR 1.481, 95% CI 1.118 to 1.962), 6 months (adjusted OR 1.448, 95% CI 1.106 to 1.896) and 12 months (adjusted OR 1.350; 95% CI 1.034 to 1.763).
Conclusion GI bleeding was associated with the increased risk of stroke recurrence after an AIS.
Introduction
Patients hospitalised with an acute ischaemic stroke are susceptible to multiple medical complications, which may increase rates of mortality and disability.1–7 One of the major medical complications of stroke is gastrointestinal (GI) bleeding.
GI bleeding during stroke hospitalisation is associated with poor outcomes in patients who had an acute ischaemic stroke (AIS).6–10 An association between GI bleeding and a higher risk of death or loss of independence in patients with stroke has been shown previously using data from the China National Stroke Registry (CNSR).11 12 Aside from one study suggesting the GI bleeding is not related to stroke recurrence,6 little data exist regarding the impact of GI bleeding on stroke recurrence. Therefore, we assessed the association between GI bleeding during hospitalisation and recurrent stroke within 12 months of AIS onset.
Methods
Data collection and study population
The CNSR was a prospective, national cohort study that has been detailed extensively in prior literature.13 Patients who had an acute stroke were included in the CSNR if they were: (1) male or female adults, (2) diagnosed with acute stroke using WHO International Classification of Diseases, 10th Revision criteria and confirmed by brain CT or MRI, (3) within 14 days after stroke onset and (4) either by themselves or via their surrogate, consented to participate in the study. We only included patients who had an AIS in this study and excluded patients with other stroke aetiologies such as transient ischaemic attack (TIA), undetermined stroke, intracerebral haemorrhage or subarachnoid haemorrhage. The CNSR study recruited patients between September 2007 and August 2008 and followed up with patients in August 2009. We collected data for our study at baseline (stoke onset) and at 3, 6 and 12 months after the stroke onset. National Institute of Health Stroke Scale (NIHSS) score was used to determine the severity of neurological impairment.14 The interviews conducted at baseline were performed for all patients by a trained investigator, and patients’ clinical characteristics including demographic information, medical history, stroke family history and baseline NIHSS scores were recorded. GI bleeding and other relevant clinical patient data were recorded during hospitalisation, typically directly from the patient or from their caregivers or surrogates. Our study divided patients into two groups based on the presence or absence of in-hospital GI bleeding.
Definition of GI bleeding
We defined GI bleeding as the presence of coffee-ground emesis, haematemesis, blood in the nasogastric tube, melena or blood in the rectum that occurred during hospitalisation and required blood transfusion or palliative intervention. All participating clinical centres used these criteria for GI bleeding diagnosis.11
Stroke recurrence assessment
The recurrence of stroke was the primary clinical outcome in this study, defined as an aggravated primary neurological deficit, a new neurological deficit or rehospitalisation with a diagnosis of ischaemic or haemorrhagic stroke15 that occurred any time from the patient’s hospital discharge until the end of the 12-month follow-up period. Once a recurrent stroke was reported by the patients, their caregivers or surrogates during the follow-up period, stroke certificates were faxed to Beijing Tiantan Hospital. Clinical coordinators and the principal investigator of the research assessed and verified suspected recurrent stroke.
Statistical analysis
Categorical variables are expressed as percentages, while continuous variables are shown as shown as mean±SD or median with IQR. We used t-tests for continuous variables and the χ2 test for categorical variables to assess differences between patients with and without GI bleeding. Univariate logistic regression analyses were used to identify the relationship between patient characteristics and recurrent stroke as well as GI bleeding and recurrent stroke, and data were expressed using unadjusted ORs with corresponding 95% CIs. Adjusted potential covariates included sex, age, baseline NIHSS, hyperlipidaemia, hypertension, atrial fibrillation, coronary heart disease, diabetes mellitus, history of TIA or stroke, family history of stroke, history of heavy drinking, history of smoking and antithrombotic treatment. We analysed data using SAS statistical software, V.9.4. A two-tailed p value <0.05 was deemed statistically significant.
Study protocol approval and patient informed consent
Before screening subjects for the CNSR, the study design and procedures were approved in each participating facility following institutional review. All participants or their legal guardians gave written informed consent to participate in the study.
Results
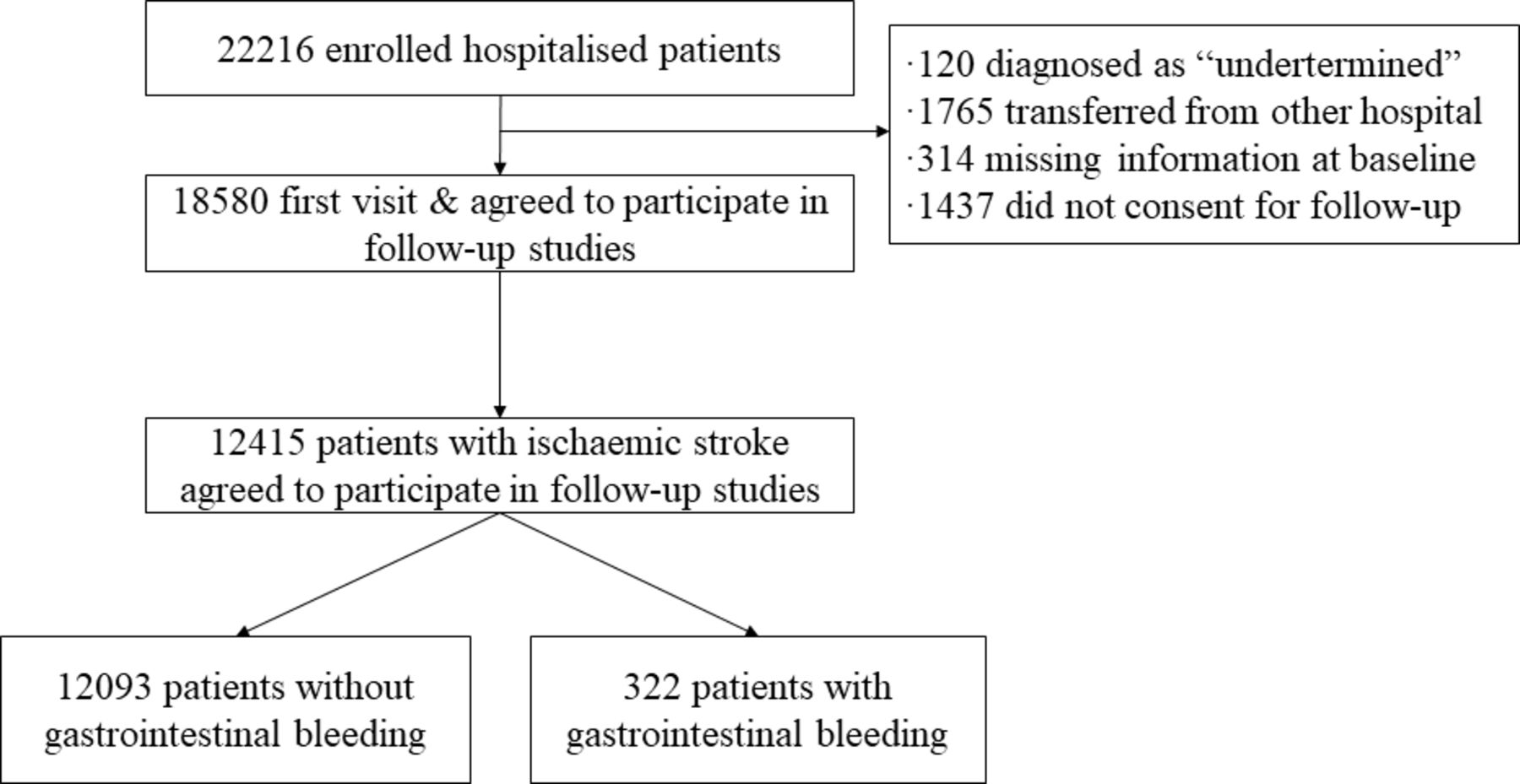
A total of 22 216 patients who had a stroke hospitalised in 132 participating centres were included in the original CNSR study. A total of 18 580 of these patients agreed to participate in follow-up studies after their first visit. Of this group, 12 415 patients were diagnosed with AIS (figure 1) and 322 (2.59%) had in-hospital GI bleeding.

Selection of study population from CNSR database. CNSR, China National Stroke Registry.
The baseline characteristics of AIS patients with or without in-hospital GI bleeding is shown in table 1. The median age of the patients was 65 years old, 61.7% of which were male and 38.3% were female. Patients with GI bleeding were significantly older, had higher NIHSS scores, suffered from hypertension, coronary heart disease, atrial fibrillation, had a history of stroke and suffered from in-hospital pneumonia or urinary tract infection, compared with those who did not have GI bleeding. Whereas gender, hyperlipidaemia, diabetes mellitus, history of TIA, family history of stroke, history of smoking, history of heavy alcohol use and antiplatelet therapy did not significantly impact incidence of GI bleeding.
Baseline characteristics of patients with initial ischaemic stroke (n=12 415)
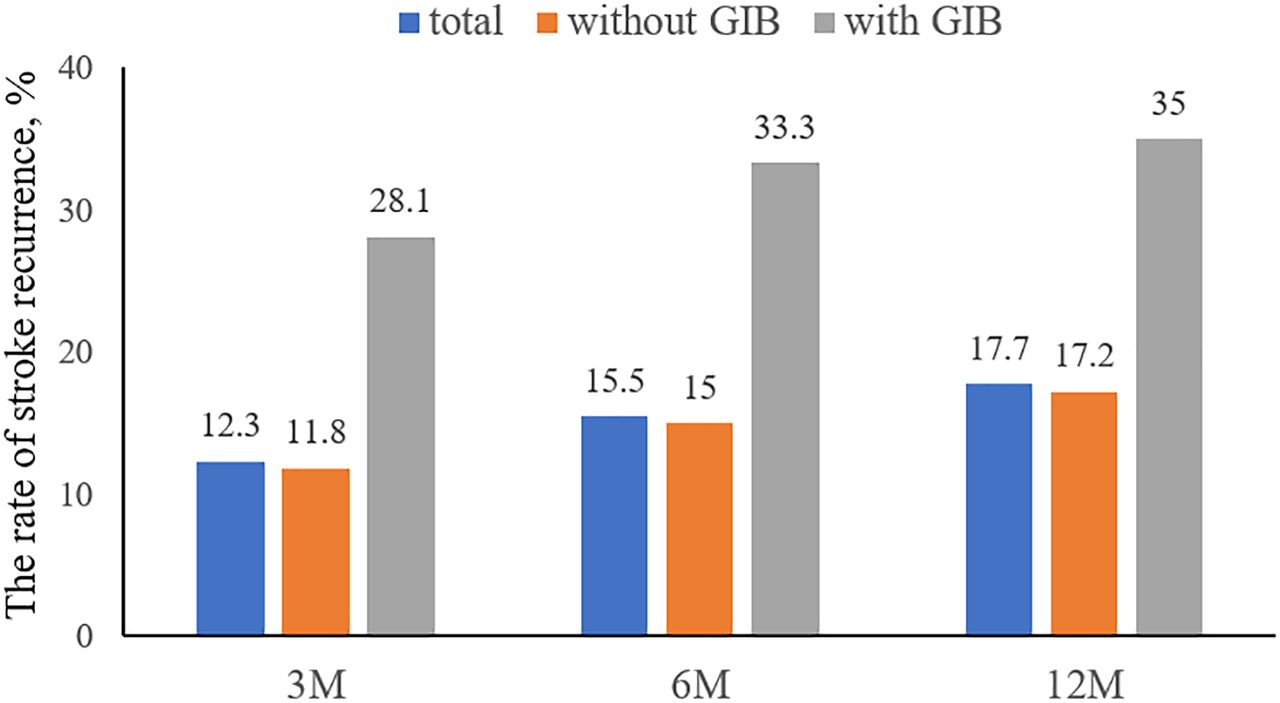
Incidence of stroke recurrence at 3, 6 and 12 months post-stroke are shown in figure 2. Overall stroke recurrence for patients at 3, 6 and 12 months after onset was 12.3%, 15.5% and 17.7%, respectively. While the stroke recurrence for patients with GI bleeding was always much higher during follow-up period (28.1%, 33.3% and 35% at 3, 6 and 12 months, respectively)

Stroke recurrence at 3, 6 and 12 months after stroke onset. GIB, gastrointestinal bleeding; M, months.
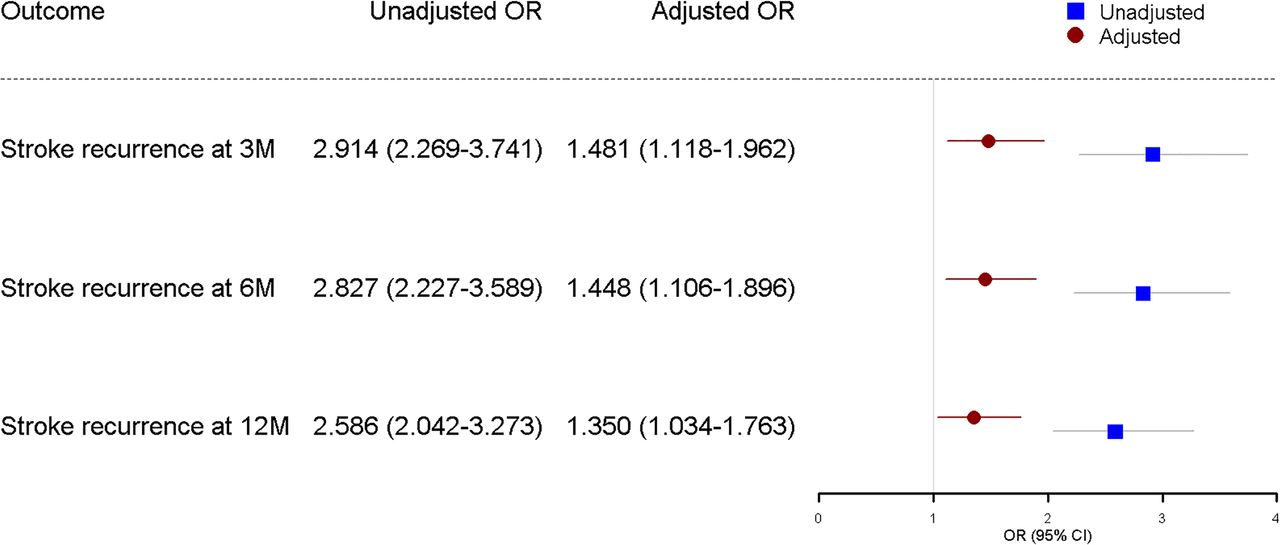
Univariate logistic regression analysis revealed that age, male gender, baseline NIHSS, high blood pressure, diabetes mellitus, coronary heart disease, atrial fibrillation, history of TIA or stroke, antithrombotic therapy, and in-hospital pneumonia or urinary tract infection were all associated with stroke recurrence at 3, 6 and 12 months following an initial AIS (table 2). GI bleeding during hospitalisation was associated with a higher risk of stroke recurrence in analyses adjusted for age, gender, baseline NIHSS, hypertension, hyperlipidaemia, diabetes mellitus, coronary heart disease, history of TIA or stroke, family history of stroke, atrial fibrillation, history of smoking, history of heavy alcohol use and antithrombotic therapy (figure 3). The adjusted ORs of recurrent stroke were approximately 1.5, 1.5 and 1.4-fold higher in patients with GI bleeding at 3, 6 and 12 months, respectively.
Univariate logistic regression analysing the effect of confounders on stroke recurrence at 3, 6 and 12 months after initial ischaemic stroke

Unadjusted and adjusted ORs of stroke recurrence in patients with gastrointestinal bleeding following acute ischaemic stroke. *Adjusted for age, sex, baseline NIHSS, hypertension, diabetes mellitus, hyperlipidaemia, history of coronary heart disease, history of TIA, family history of stroke, atrial fibrillation, history of smoking, history of heavy alcohol use and antithrombotic therapy. M, months; NIHSS, National Institute of Health Stroke Scale; TIA, transient ischaemic attack.
We also assessed the impact of antithrombotic therapy on stroke recurrence in patients with and without GI bleeding (table 3). Patients with in-hospital GI bleeding were less likely to have received antithrombotic therapy compared with those without in-hospital GI bleeding, during the 12 months after initial AIS hospitalisation.
Antithrombotic therapy usage within 12 months of initial stroke
Discussion
This study examined the impact of in-hospital GI bleeding on stroke recurrence in patients who had an AIS from the CNSR. The CNSR is the most extensive stroke registry in China and includes patients who had an acute stroke from all over the country. The prevalence of in-hospital GI bleeding in patients who had an AIS form this national prospective cohort was about 2.6%. We identified an association between in-hospital GI bleeding and increased risk of stroke recurrence in patients who had an AIS in the initial 12 months after hospitalisation.
The prevalence of GI bleeding in patients who had an AIS varies between 1.24% and 8.1% in prior studies,6–11 16–18 which may be due to geographically distinct study populations and the different AIS treatment approaches in these settings.
Limited data exist regarding risk factors for poststroke GI bleeding. Using data from the CNSR, Ji et al 19 identified advanced age, male gender, history of peptic ulcer or previous GI bleeding, history of hypertension, prestroke lack of independence, admission stroke severity, impaired consciousness and middle cerebral artery territory ischaemia as risk factors for GI bleeding after AIS. In their study, hepatic cirrhosis and posterior circulation stroke were associated with poststroke GI bleeding.19 Rumalla and Mittal identified a few previously undescribed predictors of poststroke GI bleeding, such as fluid and electrolyte imbalance, paralysis, alcohol abuse and deficiency anaemia.7
The different antithrombotic therapy may have different impacts on GI bleeding, including antiplatelet therapy and anticoagulant therapy.
Many studies suggest that patients who had a stroke are susceptible to GI bleeding, which may be associated with poor patient outcomes.6–10 The influence of GI bleeding on stroke outcomes has been discussed in prior studies, but the focus of prior work has primarily been on the impact of GI bleeding on mortality and disability.6–8 10–12 16 17 The aforementioned study from Rumalla and Mittal found that the death rate of patients who had an ischaemic stroke was 1.8-fold higher in patients with a GI bleed compared with those without.7 Earlier work from our group corroborated this finding, as we found similar increases in risk of death in stroke patients with a GI bleed.11 Other studies have shown that stroke patients with a GI bleed had a greater risk of losing functional independence poststroke versus those without GI bleeding.6–8 10 12 Our data help further quantify the impact of in-hospital GI bleeding in stroke patients by showing that this subset of patients has approximately a 1.5-fold higher risk of stroke recurrence at 3, 6 and 12 months after initial stroke hospitalisation.
The exact mechanism of how in-hospital GI bleeding increases the risk of recurrent stroke remains unclear. The presence of GI bleeding usually causes clinicians to stop the use of antithrombotic therapy, which may leave the patient in a prothrombotic state. This could cause platelet and coagulation cascade activation, thereby increasing the risk of thrombotic events.20 To reduce the risk of stroke recurrence, antithrombotic medication is recommended as a secondary prevention therapy after an ischaemic stroke of presumed arterial origin.21–23 Because antithrombotic therapy in essential in patients who had an ischaemic stroke, in-hospital GI bleeding that leads to a cessation of antithrombotic therapy could be a candidate mechanism explaining our findings. This hypothesis is supported by observed differences in antithrombotic therapy compliance of patients with and without in-hospital GI bleeding. A significant GI bleeding also influences haemodynamic stability, which is likely to increase the risk of developing an ischaemic stroke. Another mechanism may be related with the severity of stroke. Patients with severe stroke would have more complications including GI bleeding and increased risk of stroke recurrence. We did not directly assess this possible mechanism as a cause of stroke recurrence in our study, and further investigation is necessary to develop appropriate therapeutic approaches aimed at reducing stroke recurrence in patients with GI bleeding.
Our study has several limitations. First, we included patients in this study solely based on a diagnosis of GI bleeding during hospitalisation but did not extensively evaluate the therapies they were given to reduce GI bleeding, which may impact stroke recurrence. Second, patients with new GI bleeds after initial hospitalisation were not included in our study. This limited our ability to evaluate the relationship between recurrent stroke and a new GI bleed that occurred during the follow-up period. Third, the time of GI bleeding after index stroke onset, the detailed antithrombotic therapy including antiplatelet and anticoagulation medication and how long antithrombotic therapy not used were missing in the data collection. This information might have some impact on stroke recurrence. Fourth, we also did not extensively evaluate the psychological and cognitive functions of patients after AIS, which may also affect their antithrombotic medication usage.
Conclusion
We found that in patients who had an AIS, in-hospital GI bleeding significantly increased the chance of stroke recurrence. This may be indirectly caused by decreased antithrombotic therapy usage in patients having GI bleeding. Thus, approaches used to prevent and treat GI bleeding after stroke should be carefully considered to help avoid increased risk of stroke recurrence.
Footnotes
PW and YW contributed equally.
Contributors YoW and PW are co-corresponding author. Study concept and design: YoW, PW and WD. Provision of study materials or patients: all authors. Drafting of the manuscript: YoW, PW and WD. Critical revision of the manuscript for important intellectual content: GL and RJ. Statistical analysis: AW, YP and HG. Study supervision and organization of the project: YoW, XZ, YiW, LL and KD.
Funding This study was supported by grants from the National Key Research and Development Program from the Ministry of Science and Technology of China (2018YFC1312400), the Ministry of Science and Technology of the People’s Republic of China (2016YFC0901002, 2016YFC0901001, 2017YFC1310901, 2017YFC1307905 and 2018YFC1312903), grants from Beijing Municipal Administration of Hospitals’ Mission Plan (SML20150502), grants from National Natural Science Foundation of China (81600999), grants from Beijing Municipal Science & Technology Commission (D171100003017002 and D151100002015003) and grants from National Science and Technology Major Project (2017ZX09304018).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by ethics committee at Beijing Tiantan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}
{kind=link}