

Abstract
Background and aim In-stent restenosis (ISR) belongs to an infrequent but potentially serious complication after carotid angioplasty and stenting in patients with severe carotid stenosis. Some of these patients might be contraindicated to repeat percutaneous transluminal angioplasty with or without stenting (rePTA/S). The purpose of the study is to compare the safety and effectiveness of carotid endarterectomy with stent removal (CEASR) and rePTA/S in patients with carotid ISR.
Methods Consecutive patients with carotid ISR (≥80%) were randomly allocated to the CEASR or rePTA/S group. The incidence of restenosis after intervention, stroke, transient ischaemic attack myocardial infarction and death 30 days and 1 year after intervention and restenosis 1 year after intervention between patients in CEASR and rePTA/S groups were statistically evaluated.
Results A total of 31 patients were included in the study; 14 patients (9 males; mean age 66.3±6.6 years) were allocated to CEASR and 17 patients (10 males; mean age 68.8±5.6 years) to the rePTA/S group. The implanted stent in carotid restenosis was successfully removed in all patients in the CEASR group. No clinical vascular event was recorded periproceduraly, 30 days and 1 year after intervention in both groups. Only one patient in the CEASR group had asymptomatic occlusion of the intervened carotid artery within 30 days and one patient died in the rePTA/S group within 1 year after intervention. Restenosis after intervention was significantly greater in the rePTA/S group (mean 20.9%) than in the CEASR group (mean 0%, p=0.04), but all stenoses were <50%. Incidence of 1-year restenosis that was ≥70% did not differ between the rePTA/S and CEASR groups (4 vs 1 patient; p=0.233).
Conclusion CEASR seems to be effective and save procedures for patients with carotid ISR and might be considered as a treatment option.
Trial registration number NCT05390983.
WHAT IS ALREADY KNOWN ON THIS TOPIC
In-stent restenosis is relatively prevalent complication after carotid stenting.
Optimal management of in-stent restenosis is controversial.
WHAT THIS STUDY ADDS
Both carotid endarterectomy and repeat percutaneous transluminal angioplasty with or without stenting are safe procedures.
Both interventions have comparable low risk of perioperative complications.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Carotid endarterectomy is second level option for in-stent restenosis.
It might be considered after repeated angioplasty failure.
Introduction
Carotid angioplasty and stenting (CAS) is a safe and effective alternative to carotid endarterectomy (CEA) that is widely used for primary and secondary stroke prevention in patients with severe symptomatic or asymptomatic carotid artery stenosis, especially in patients at high risk for complications during or after CEA because of co-morbidities, anatomic variations or contraindications.1–5 In-stent restenosis (ISR) is an infrequent but potentially serious complication after CAS that occurs in 3.5%–14% of patients and causes an ischaemic event in up to 2% of patients.3–11 Data from the largest randomised controlled trials in which the safety and efficacy of CAS and CEA were determined reported the incidence of ISR at the upper end of this range, that is, 11.1% in the SPACE trial3 and 12.2% in the CREST trial.4 Thus, ISR is one of factors limiting the long-term efficacy of CAS.
Nevertheless, the optimal management of patients with carotid ISR is controversial due to a lack of consensus with respect to definitions, intervention indications, type of intervention and technical strategies.12–14 Usually, reintervention with repeated endovascular procedures is recommended for patients with ISR.13–15 Restenosis should be first treated with in-stent balloon inflation (repeated percutaneous transluminal angioplasty; rePTA), and if necessary, with the implantation of a new stent, that is, stent-in stent. However, both methods (especially rePTA) are sometimes associated with unsatisfactory long-term results due to high rates of repeated ISR.3–11 Moreover, rePTA with or without stenting (rePTA/S) might be contraindicated or technically problematic in some patients. Therefore, other treatment methods are being investigated. Carotid endarterectomy with stent removal (CEASR) is one of these methods but clinical randomised trials demonstrating its safety and efficacy compared with rePTA/S are still lacking.2 6 16–18
The aim of this randomised study was to compare the safety and effectiveness of CEASR and rePTA/S in patients with carotid ISR.
Methods
All consecutive patients with ISR after CAS treated at the University Hospital Ostrava between July 2017 and June 2021 were selected for the study. The inclusion criteria were as follows:
ISR in the carotid artery (80%–99%).
Indication for carotid reintervention.
18–80 years of age.
Functionally independent with a modified Rankin score value of 0–2 points.
Signed informed consent.
The exclusion criteria were as follows:
Contraindication to general anaesthesia.
Contraindication to angiography (eg, iodine allergy).
Technically impossible to perform angioplasty with or without stenting.
Participation in another clinical study within 60 days.
Technically impossible to perform carotid endarterectomy (according to surgeon discretion, eg, high cervical position of ISR).
Patients with ISR of the carotid artery and an indication for carotid intervention who met all inclusion and exclusion criteria were randomly allocated using computer-based randomisation system into the rePTA/S or CEASR groups.
CEA with stent removal
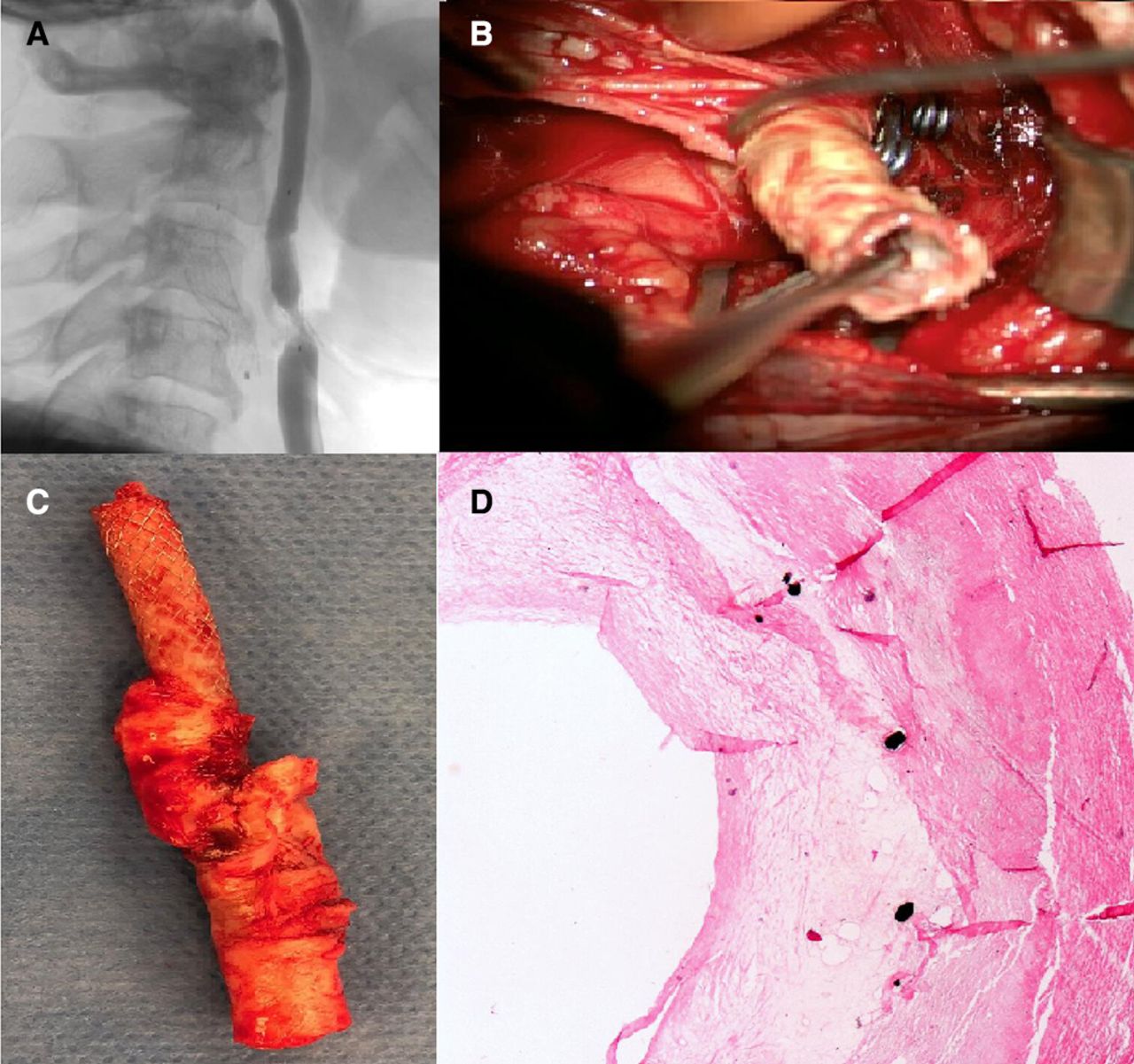
Surgery was performed using general anaesthesia using a cut at the front angle of the sternomastoid muscle by one experienced surgeon (˃700 CEA during 10 years). The common carotid artery (CCA), then the internal carotid artery (ICA) and external carotid artery (ECA) were isolated. The CCA, ICA and ECA were temporarily closed. Using a longitudinal cut to the CCA and ICA, a stent with an atherosclerotic plaque was visualised. The stent and plaque were withdrawn under microscopic control and a suture for the arteriotomy was placed using a monofilament, non-absorbent 6/0 fibre. Before completing the procedure, haemostasis was controlled and drainage was set. Surgery was completed by suturing the subcutis and cutis. Unfractionated heparin (100 IU/kg of body weight) was administered to all patients just before the arteriotomy. In cases with insufficient collateral flow into the middle cerebral artery after clipping of the CCA and ICA, a temporal shunt was used. Antiplatelet therapy (clopidogrel (75 mg/day) or acetylsalicylic acid (100 mg/day)) was used continuously in all patients (figure 1).

Carotid endarterectomy with stent removal in patients with carotid in-stent restenosis. Carotid in-stent restenosis on digital subtraction angiography before surgery (A), stent removal during carotid endarterectomy (B), removed stent with atherosclerotic plaque after carotid endarterectomy (B) and histology of atherosclerotic plaque with a stent (B).
Repeated carotid percutaneous transluminal angioplasty with or without stenting
Endovascular interventions were performed under local anaesthesia via femoral access in the department with 100–150 performed CAS per year by two experienced interventional radiologists. Unfractionated heparin (100 IU/kg of body weight) was administered to all patients. The procedure began with a diagnostic angiography. On verification of severity and morphology of the in-stent stenosis, a 90 cm 6F sheath was introduced into the CCA. The procedure was performed using distal filter protection (FilterWire EZ; Boston Scientific, Natick, Massachusetts, USA). ISR was treated preferentially with a 5 mm diameter drug-eluting balloon (Sequent Please OTW, B. Braun Melsungen AG, Melsungen, Germany; off label use). In patients with gracile arteries or more severe stenoses, predilation with a 3 mm or 4 mm diameter balloon (according to the decision of the radiologist) was carried out. Atropine (<1.0 mg) was administered intravenously to prevent serious bradycardia during dilation. The single-layer stent (Carotid Wallstent, Boston Scientific, Santa Clara, California, USA) was placed within the previous stent in patients with a suboptimal result after angioplasty at the discretion of the interventionist. Whenever possible, a double-layer technology stent (Roadsaver, Terumo, Tokyo, Japan) was used to ensure maximum wall coverage. The distal filter was removed, followed by completion of the angiogram, including the intracranial arteries. Dual-antiplatelet therapy (clopidogrel (75 mg/day) and acetylsalicylic acid (100 mg/day)) was administered for at least 6 weeks postprocedure. All patients underwent preprocedural laboratory testing to determine clopidogrel resistance. Clopidogrel was replaced by prasugrel or ticagrelor in clopidogrel non-responders (figure 2).

Repeat percutaneous transluminal angioplasty in patient with carotid in-stent restenosis. Carotid in-stent restenosis on digital subtraction angiography before angioplasty (A) and residual in-stent stenosis after angioplasty (B).
Clinical examinations
Standard physical and neurological examinations using the National Institutes of Health Stroke Scale and modified Rankin scale were performed before intervention (CEASR or rePTA/S), and at 24 hours, after 30 days and 1 year after the CEA by blinded certified vascular neurologist.
The primary end-point was defined as combined end-point of any vascular event (stroke, transient ischaemic attack, amaurosis fugax, retinal infarction, myocardial infarction or vascular death) within 30 days after intervention, restenosis ˃50% or occlusion of intervened artery within 1 year after intervention and local complications associated with CEASR or rePTA/S within 30 days after intervention.
Neurosonology examination
A standard neurosonology examination was performed prior to intervention, 30±3 days and 1 year±14 days after intervention by certified neurosonologist. Specifically, the examination included duplex sonography of the carotid and vertebral arteries with evaluation of residual stenosis or restenosis in the intervened artery, and transcranial colour-coded duplex sonography with evaluation of blood flow in the main arteries of the circle of Willis. Criteria published by Setacci et al 19 and von Reutern et al 20 were used for evaluation of the severity of restenosis. Criteria for 80% restenosis were: average peak systolic velocity (PSV) 370 cm/s, poststenotic PSV <30 cm/s, end diastolic velocity >140 cm/s, present collateral flow and carotid ratio (ICA/CCA) >4.
Statistical analysis
An estimate for the minimum sample size calculation to demonstrate non-inferiority was based on a 40% difference in composite end-point with an alpha level of 5% and a power of 80%. A prestudy statistical calculation determined that a minimum sample size of 30 patients was required to complete the study. Assuming that 25% of screened patients will not meet all inclusion criteria or will not complete the study, a minimum of 40 patients were needed to screen for study eligibility.
All statistical tests were performed at the Centre for Health Research (Faculty of Medicine, University of blinded). The normality of the distribution of all data was checked using the Shapiro-Wilk test. Data with a normal distribution are reported as the mean±SD. Parameters not fitting a normal distribution are presented as the mean, median and IQR. Categorical variables in the two arms were compared using the Pearson χ2 or Fisher’s exact test. Continuous variables were compared by the Student’s t-test for normally distributed values or the two-sample Wilcoxon rank sum (Mann-Whitney) test. All tests were carried out at a 0.05 alpha level of significance using STATA V.17 (StataCorp).
Results
Of 40 screened patients (24 males and 16 females; mean age, 68.5±6.0 years) with carotid artery stenosis (˃80%), 31 (19 males and 12 females; mean age, 67.6±6.2 years) fulfilled all inclusion criteria. Fourteen and 17 patients were randomly allocated to the CEASR and rePTA/S groups, respectively. New stents were implanted in six patients in the rePTA/S group; the other patients underwent angioplasties. The demographic data are shown in table 1. There was no statistically significant difference between groups for any parameter. All patients in both groups who underwent ISR procedures were asymptomatic prior to randomisation (table 2).
Demographic data
Study results
Both interventions were safe, no periprocedure vascular events were recorded 30 days and 1 year after intervention and combined end-point was recorded in only 21.4% patients in CEASR group and 29.4 % patients in rePTA/S group, respectively (table 2). The implanted stent in carotid restenosis was successfully removed in one peace with atherosclerotic plaque without vessel wall damage in all patients in the CEASR group. Only one patient in the CEASR group had asymptomatic occlusion of the intervened carotid artery within 30 days. One patient died due to COVID-19 infection in the rePTA/S group within 1 year after intervention. Residual stenosis after intervention was significantly greater in the rePTA/S group (mean, 20.9 %) than the CEASR group (mean 0 %, p=0.04). Nevertheless, residual stenosis ≥50% was not detected in any patient in either group. Restenosis (≥70 %) after 1 year was not significant more often in the rePTA/S group compared with the CEASR group (4 vs 1 patient; p=0.233; table 2). No intimal injuries were observed.
Discussion
The current randomised pilot study showed that both rePTA/S and CEASR are safe procedures for treating carotid ISR. No patient in any group had a stroke, transient ischaemic attack or myocardial infarction within 1 year after intervention.
Although CEA is still the method of first choice in patients with severe symptomatic or asymptomatic stenosis, in recent years CAS has become a completely equivalent method to CEA in many such patients.1–5 In some cases, such patients at high surgical risk or in patients in whom a CEA cannot be performed for technical reasons, CAS is clearly the first choice.8 The advantages of CAS include the cosmetic effect, avoidance of cranial nerve palsy and a shorter hospitalisation time.8 21 22
ISR after CAS is one of the more serious complications associated with this procedure.3–11 The incidence of ISR is relatively rare and varies significantly between studies. One of the reasons for the variations in incidence is the inconsistent definition of ISR.12 The definition of ISR depends not only on the minimum percentage of restenosis, which is already evaluated as ISR, but also on the time of the evaluation, that is, the time since CEA, and the examination method.
The most common method with which to evaluate ISR is duplex sonography. It is necessary, however, to take into account the change in hemodynamics of the stent and modify the criteria for evaluating the severity of stenosis according to flow rates.2 19 23–25 Digital subtraction angiography is the gold standard for evaluating DSA, but it is limited by invasiveness, while CT angiography and MR angiography are limited by stent artefacts.26 27
The risk of clinical manifestation of stenosis are as follows: the risk of an ischaemic cerebrovascular event, including transient ischaemic attack, ischaemic stroke, ischaemia of the eyeball (amaurosis fugax and retinal infarction) and the haemodynamic risk of injury (reduced local perfusion) to the brain, especially the risk of accelerating the progression of cognitive function decline with the risk of developing dementia.7 8
Currently, there are several treatment options for ISR. The best medical treatment is one of the intervention methods. Recently, cilostazol is tested for a reduction of ISR risk.28 29 At present, rePTA is used more often than rePTAS and different drug-coated baloons are tested. However, there is still no clear evidence of effectiveness of drug-coated balloons.13 30 31 CEASR is the next method of choice, especially in patients in whom rePTA/S has failed or this method cannot be performed due to technical obstacles.6 13 17 18 31 Rarely, carotid bypass or external beam radiotherapy can also be used.14 The results of published meta-analyses were similar to our results. Specifically, CEASR is a comparable method to rePTA/S with a low risk of perioperative vascular events. A recent meta-analysis with >1000 patients with intervention for ISR from 11 studies demonstrated that both rePTA/S (85% of the cohort) and CEASR (15% of the cohort) had similarly low rates of perioperative vascular events (1% vs 2 %), death (0% vs 3 %) and restenosis after the second intervention (0% vs 0 %); the procedures were equally feasible and effective for treating ISR.13 No statistically significant differences were found in the incidence of the other severe complications. Ten patients in the rePTAS group had a documented deformation or kinking of the stent as a shortcoming of CAS.13 These results are comparable with results of our randomised study where no vascular events or death were recorded.
Although rePTA/S remains the method of first choice, CEASR can be considered in patients with repeated rePTA/S failure, in patients with contraindication or high risk of rePTA/S, for example, in patients with severely calcified plaques or preocclusive stenosis.6 17 18 Contrary, a relative contraindication to CEASR might be a patient with a high risk for open surgery or a technically difficult procedure, for example, if the stent is long enough or placed in a distal position of ISR beyond the surgeon’s control.27 There were limitations to this study that need to be considered. First, the number of included patients was relatively low. The sample size calculation was performed to show non-inferiority of tested methods in combined end-point. The incidence of ISR was low and a randomised clinical trial comparing rePTA/S and CEASR with a higher number of included patients is still missing. However, due to the positive results of this pilot study, a multicentre clinical randomised trial is being prepared. The second limitation was the impossibility of comparing rePTA with rePTAS because the stent was implanted according to technical possibilities at the discretion of the interventional radiologist and was not randomised or mandatory. The last limitation was the follow-up time. Patients were followed for 1 year, thus it was not possible to determine the long-term risk of restenosis.
Conclusions
Both CEASR and PTA/S appear to be safe and effective methods for the treatment of carotid ISR with a comparable low risk of perioperative complications and long-term risk of vascular events.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in accordance with the ethical standards of our Institutional Ethics Committee (approved by the Ethics Committee of the University Hospital of Ostrava on 25 May 2017; approval no. 497/2017). Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors TH performed carotid endarterectomies with stent removal, made a substantial contribution to the concept and design, analysis and interpretation of data, drafted the article, approved the version to be published, is responsible for the overall content as the guarantor. JF performed carotid endarterectomies with stent removal, made a substantial contribution to the concept and design, analysis and interpretation of data, drafted the article, approved the version to be published. VP performed percutaneous transluminal angioplasty with or without stenting, made a substantial contribution to the concept and design, revised article critically for important intellectual content, approved the version to be published. TJ evaluated radiological data, made a substantial contribution to the concept and design, revised article critically for important intellectual content, approved the version to be published. MR performed neurological examinations, made a substantial contribution to the concept and design, revised article critically for important intellectual content, approved the version to be published. DP made a substantial contribution to the concept and design, revised article critically for important intellectual content, approved the version to be published. DV performed neurological examinations, made a substantial contribution to the concept and design, revised article critically for important intellectual content, approved the version to be published. DN made a substantial contribution to the concept and design, revised article critically for important intellectual content, approved the version to be published. TH performed statistical analyses, made a substantial contribution to the study design, analysis and interpretation of data, revised article critically for important intellectual content, approved the version to be published. DS made a substantial contribution to the concept and design, acquisition of data, approved the version to be published.
Funding This work was supported by the Ministry of Health of the Czech Republic (grants number NV-19-04-00270, NV-19-08-00362 and NU22-04-00389).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References




{kind=link}
{kind=link}