

Stroke happens to people of all ages and has become the leading cause of disability in the world.1 It is also the leading cause of death in China and fifth-leading cause of death in the USA.2 3 Prevention of stroke is the best treatment. The use of antiplatelet therapy is one of the main prevention strategies. Aspirin is the only antiplatelet drug indicated for primary or secondary stroke prevention. Since the invention of aspirin nearly 120 years ago, more antiplatelet agents are available. Clinicians can select one antiplatelet drug or the combination for a specific patient with a specific subtype of ischaemic stroke. This kind of precision antiplatelet therapy can maximise the benefit and lower the risk of haemorrhagic complications.
By acetylating serine 530 of cyclooxygenase-1, aspirin inhibits platelet generated thromboxane A2 and renders its antiplatelet effect. Aspirin is indicated for primary prevention of cardiovascular events in population between the age 40 and 59 with >10% risk over 10 years and low risk of gastrointestinal or intracranial haemorrhage.4
For secondary ischaemic stroke prevention, there are many choices, used either as a mono or dual therapy. The antiplatelet effect of dipyridamole is through its inhibition of phosphodiesterase activated through platelet cyclic AMP. From the European Stroke Prevention Study 2 trial, the combination of aspirin plus extended-release dipyridamole (ASA-ERDP) was 23% more effective than aspirin alone in secondary stroke prevention.5 However, the findings in the Aspirin and Extended-Release Dipyridamole vs Clopidogrel for Recurrent Stroke trial showed that ASA-ERDP and clopidogrel had similar rate of stroke recurrence (9.0% vs 8.8%) and ASA-ERDP group had slightly more major haemorrhagic events (4.1% vs 3.6%).6 Currently, the use of ASA-ERDP has significantly decreased in the clinical setting due to its two times per day dose regimen and relatively higher price.
Like dipyridamole, cilostazol exerts its antiplatelet function by inhibiting phosphodiesterase activity and suppressing the cAMP degradation. Its secondary stroke prevention was studied in Japan mainly in the cilostazol for prevention of secondary stroke (CSPS 2), in which the annual rate of recurrent stroke was 2.76% (n=82) in the cilostazol group and 3.71% (n=119) in the aspirin group (HR 0.743, 95% CI 0.564 to 0.981; p=0.0357).7
Clopidogrel, one of the two thienopyridines on the market, is a prodrug that requires to be metabolised in the body to its active metabolite. It will then inhibit the binding of ADP to its platelet P2Y12 receptor and the subsequent ADP-mediated activation of the glycoprotein IIb/IIIa complex (GPIIbIIIa), thereby inhibiting platelet aggregation. In the trial of clopidogrel versus aspirin in patients at risk of ischaemic events, clopidogrel outperformed aspirin in secondary stroke, myocardial infarction and vascular death prevention by 8.7% (relative risk reduction).8
Unlike the thienopyridine drugs, ticagrelor is a cyclopentyltriazolopyrimidine. It directly and reversibly blocks ADP receptor of subtype P2Y12 without the need of hepatic activation. Advantages of ticagrelor include avoiding the variability seen with the drugs that metabolise through the CYP450 system and not being affected in CYP2C19 polymorphism. Its antiplatelet effect is more consistent and reversible, hence no need to stop for 5–7 days prior to a surgical procedure. However, using ticagrelor alone for secondary stroke prevention lacks the evidence. In the Ticagrelor versus Aspirin in Acute Stroke or Transient Ischemic Attack (SOCROTES) trial, the 90-day recurrent ischaemic stroke occurred in 5.8% of patients on ticagrelor and 6.7% on aspirin, with no difference in haemorrhagic events (0.5% vs 0.6%).9
Dual antiplatelet therapy (DAPT) has been widely prescribed for secondary stroke prevention since the publication of Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack (CHANCE) and Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA (POINT) trials. Both trials showed the benefit of aspirin plus clopidogrel (21–90 days) in the prevention of stroke in patients with a minor stroke (National Institute of Health Stroke Scale (NIHSS) <3) or high-risk TIA. For those with an NIHSS <5, the rate of recurrent stroke was slightly lower in patients treated with 30-day ticagrelor-aspirin (5%) vs aspirin (6.3%) in the Ticagrelor and Aspirin or Aspirin Alone in Acute Ischaemic Stroke or TIA trial.10
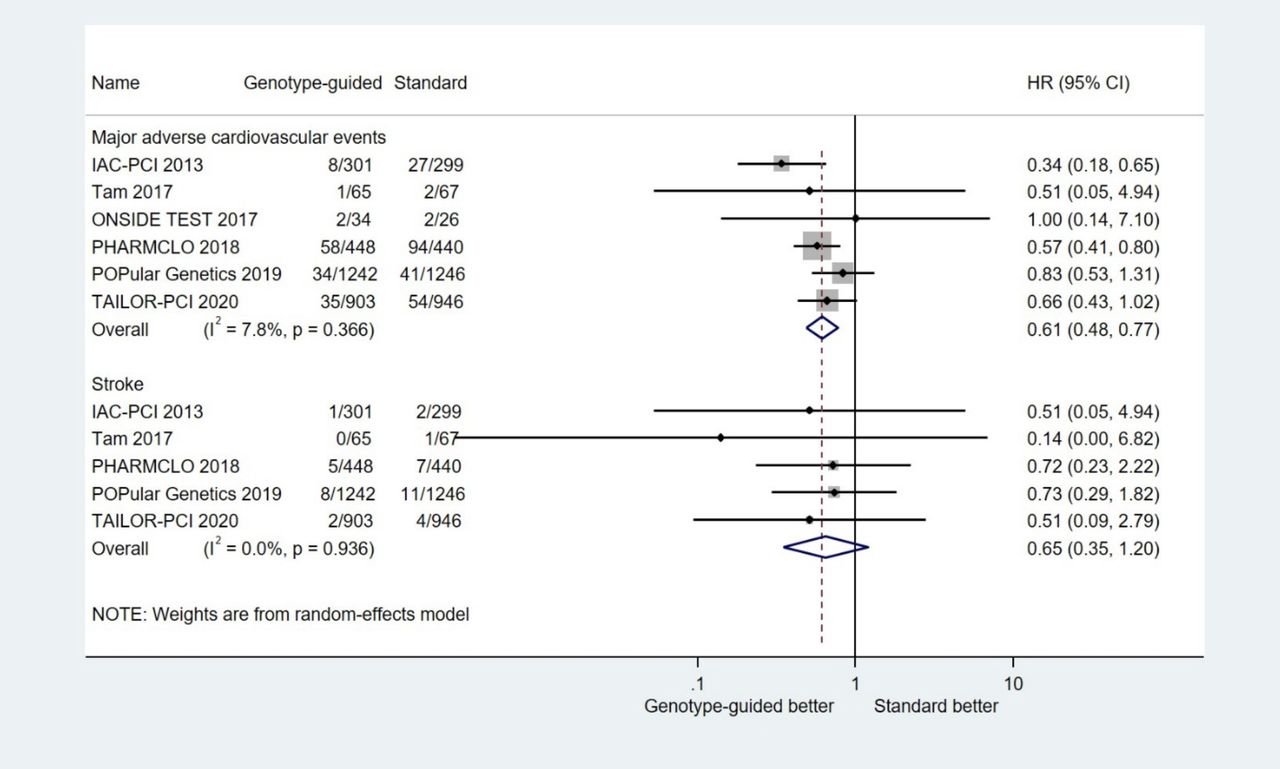
The challenge lies in the ineffectiveness of clopidogrel in patients who are CYP2C19 carriers. However, such carrier status seemed to have no impact on ticagrelor. Ticagrelor versus clopidogrel in CYP2C19 Loss-of-Function Carriers with Stroke or TIA (CHANCE II) enrolled patients with minor strokes (NIHSS <3) or high risk TIAs but were carries of CYP2C19. After 90-day treatment with either ticagrelor–aspirin or clopidogrel–aspirin, the rate of recurrent stroke in the ticagrelor-aspirin group was 6.0% vs 7.6% in those treated with clopidogrel–aspirin (HR 0.77; 95% CI 0.64 to 0.94; p=0.008). There was no difference in the rate of moderate or severe haemorrhagic events between the two treatment groups (0.3% vs 0.4%).11 However, the overall haemorrhagic events were higher in ticagrelor–aspirin group (5.3%) vs clopidogrel–aspirin group (2.5%). Like the findings in patients with acute coronary syndrome or those undergoing percutaneous coronary intervention (figure 1), the results in the CHANCE-2 trial indicated that patients with ischaemic stroke or TIA may benefit from genotype-guided strategy for secondary event prevention. Since the benefit of aspirin-ticagrelor is in patients who are carrier of CYP2C19, it may be prudent that stroke patients who are potential carriers should be tested for the carrier status before prescribing the antiplatelet drug.

Meta-analysis of genotype-guided strategy in patients with acute coronary syndrome or undergoing percutaneous coronary intervention. IAC-PCI: Individual Applications of Clopidogrel After Percutaneous Coronary Intervention (ChiCTR-TRC-11001807); Tam et al (2017) (NCT01994941); ONSIDE TEST: Optimal Antiplatelet Pharmacotherapy Guided by Bedside Genetic or Functional Testing in Elective Percutaneous Coronary Intervention (NCT01930773); PHARMCLO: Pharmacogenetics of Clopidogrel in Patients With Acute Coronary Syndromes (NCT03347435); POPular Genetics: CYP2C19 Genotype Guided Antiplatelet Therapy in ST-Segment Elevation Myocardial Infarction Patients-Patient Outcome After Primary PCI (NCT01761786); TAILOR-PCI: Tailored Antiplatelet Therapy Following PCI (NCT01742117).
Other DAPT includes cilostazol plus aspirin and cilostazol plus clopidogrel. Both showed a reduced annual incidence of recurrent ischaemic stroke by half compared with monotherapy (2.2% dual therapy with cilostazol vs 4.5% monotherapy) in the CSPS.COM trial.12 This trial has a lower level of evidence since it was an open label design, unable to be completed, about 7% of patients lost to follow-up, and had a low event rate. CSPS.COM did not specify NIHSS score in patients enrolled. However, one of the enrolling criteria was to have >50% either intra or extra cranial large artery stenosis.
In conclusion, for primary stroke prevention, the use of aspirin in population between 40 and 59 years old must show a 10-year vascular risk is >10%, can live for >10 years and a low risk of haemorrhage. For secondary stroke prevention, patients with a minor stroke or high-risk TIA (NIHSS <3) and who are not carriers of CYP2C19, 21–90 days of clopidogrel–aspirin is indicated. If their NIHSS is <5, ticagrelor–aspirin for 30 days can be considered. If they are CYP2C19 caries, then 90-day ticagrelor–aspirin offers better stroke prevention. Cilostazol–aspirin or cilostazol–clopidogrel can be an alternative. If clopidogrel or aspirin cannot be tolerated, cilostazol alone is the option. Precision genotype-guided antiplatelet therapy for stroke prevention will likely be the new standard.
Ethics statements
Patient consent for publication
Footnotes
Contributors DW is the sole author of the contribution.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.





{kind=link}