

Article Figures & Data
Figures
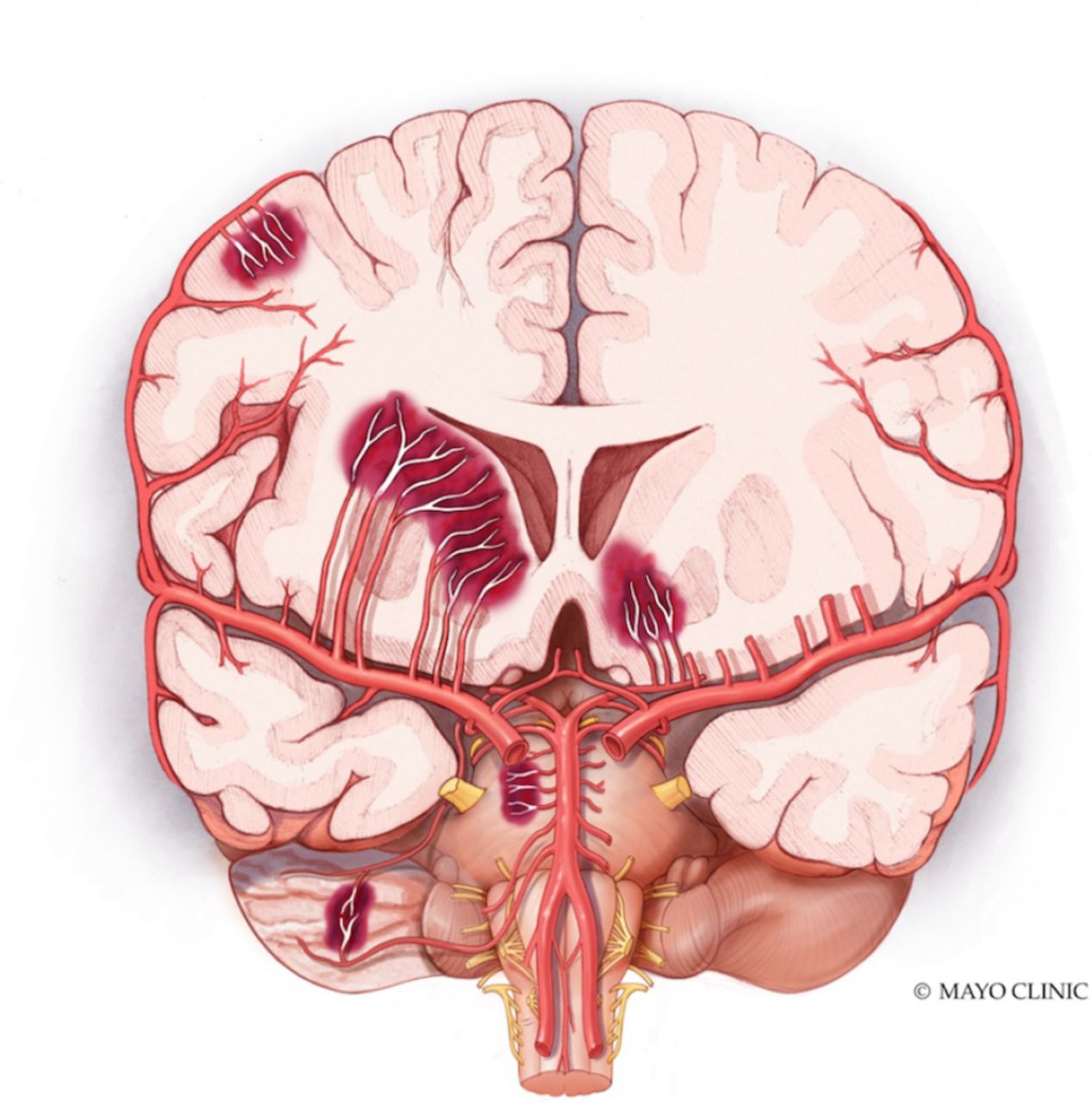
- Figure 2
Coronal section illustrating the different locations of intracerebral haemorrhage, special attention to lobar and deep-seated haemorrhages. Mayo clinic foundation for medical illustration and Research.
- Figure 1
Summary of primary and secondary causes of ICH. *Vascular malformations: arteriovenous malformations, cavernous malformation, fistula. CAA, cerebral amyloid angiopathy; ICH, intracerebral haemorrhage.
- Figure 3
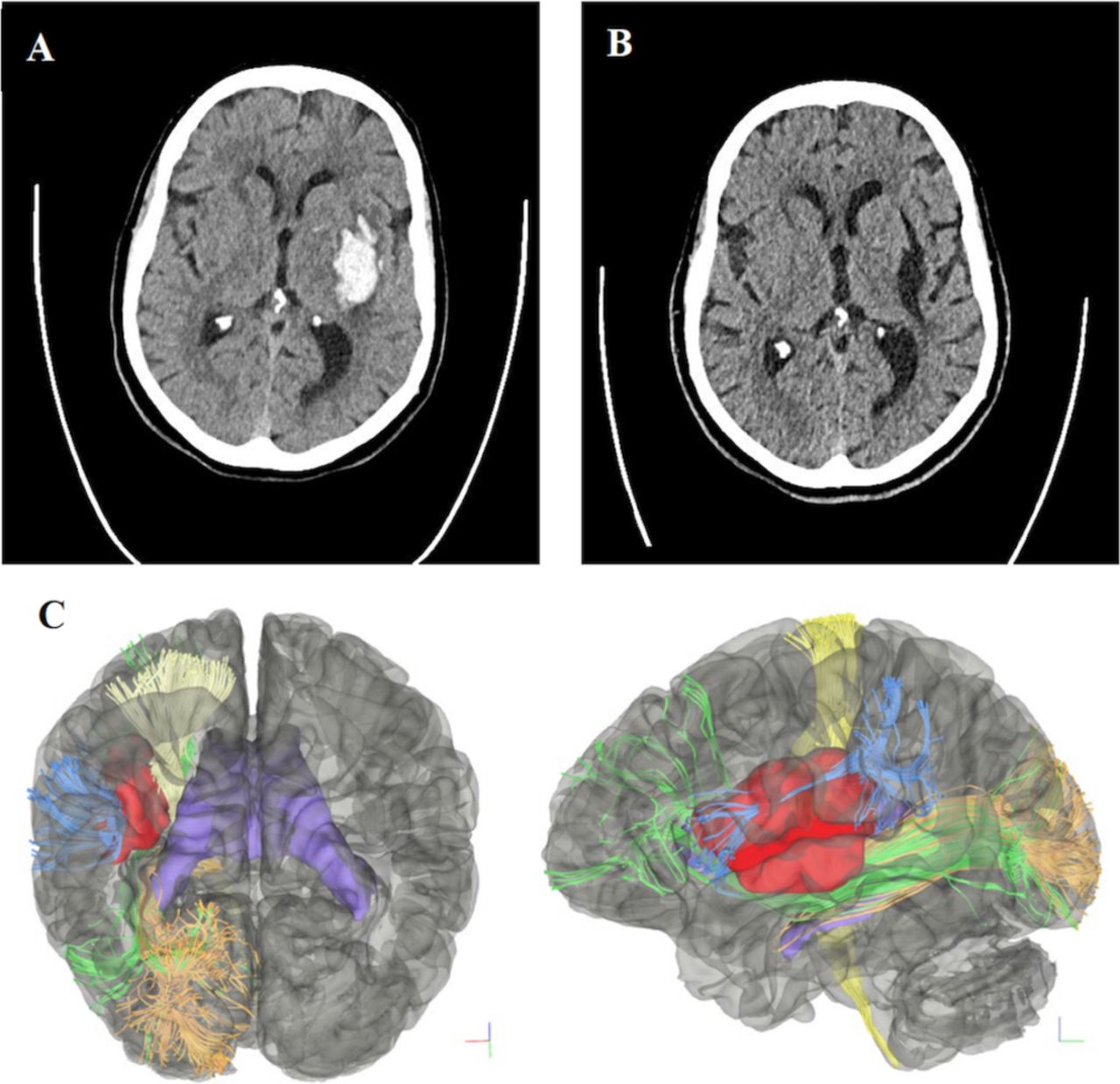
Patient 1. ICH in the left basal ganglia and left temporal lobe. (A) Preoperative non-contrast CT showing left-sided intraparenchymal haemorrhage within the insular region without midline shift. (B) Non-contrast CT 3 months post-op showing a stable residual cystic cavity from haematoma evacuation. (C) Coronal (left) and sagittal (right) DTI-generated preoperative simulated 3D tractography of patient 1. The location of the clot (red) is shown relative to the corticospinal tract (light yellow), inferior fronto-occipital fasciculus (green), optic radiations (orange) and lateral portion of the superior longitudinal fasciculus (SLF 3) (sky blue). Lateral ventricles (purple) are showed as reference. DTI, diffusion tensor imaging; ICH, intracerebral haemorrhage.
- Figure 4
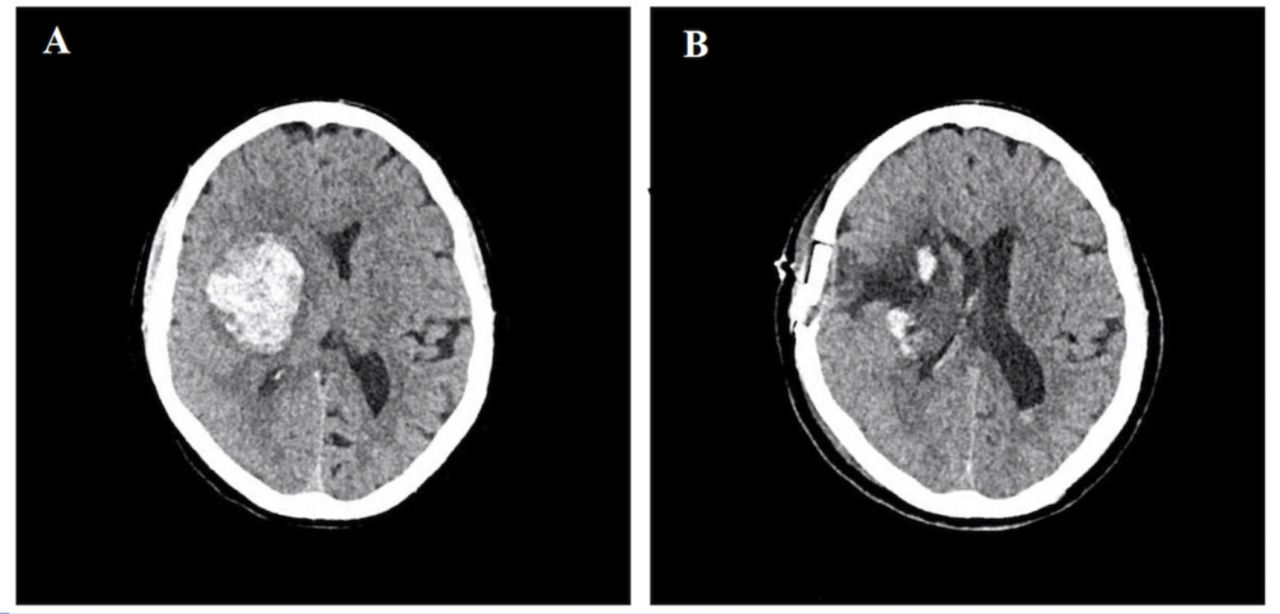
Patient 2, with right basal ganglia deep brain parenchymal haematoma. (A) Initial non-contrast head CT showing a right haemispheric parenchymal haematoma centred in the basal ganglia with extension into the frontal lobe/insular region and effacement of the right lateral ventricle. (B) Postoperative CT without contrast on day 2 after haematoma evacuation showing good clot evacuation without rebleeding.




Tables
- Table 1
Comparison of different innovative minimally invasive techniques for ICH
Study Type of study Method of ICH evacuation No of patients Neurological outcome ICH score Preoperative volume (cm3) % ICH removal % ICH-related mortality Procedure-related complications Limitations BrainPath Prybylowski et al41 Retrospective
case seriesEAME with BrainPath System 11 36% functionally independent at 90-day follow-up, 2 mildly functional independent 2 (range:1–4) 51 (range 9–168) 87% (38%–99%) 36 Haemorrhage: n=1 Small sample size, retrospective nature Bauer et al42 Prospective, single-centre study (pilot) BrainPath system 18 GCS increase preoperatively 10–14 pts 2.4 (SD 1.0) 52.7 mL (SD 22.9) 95.7 (SD 5.8) 5.60 None reported Small sample size, single centre Labib et al46 Retrospective multicentre study Mi SPACE approach 39 Increased GCS from 10 to 15 pts 2 (range: 0–3) 36 (range: 27–65) >90% in 72% of patients, 75%–89% in 23% of patients and 50%–75% in 5% of patients 0 Rebleed (n=1), middle cerebral artery perforator infarct (n=1) Retrospective nature Griessenauer et al52 Retrospective matched cohort BrainPath system 5 Preoperatively GCS 10, postoperatively GCS 3 2 (1–3) 42.3 (SD 9.1) – 2 (40) None reported Retrospective nature, small sample size, delayed treatment time Apollo System Spiotta et al50 Multicentre, retrospective case series Apollo System 29 Acute neurological deficits (n=12), chronic neurological deficits(n=2) – 45.4 (SD 30.8) 54.1% (SD 39.1) 13.80 Rebleeding and increased oedema, decompressive craniectomy (n=2) Retrospective, delayed TTT Griessenauer et al52 Retrospective Matched cohort Apollo System 5 Preoperative GCS 9, postoperative GCS 10 3 (range: 1–4) 50.7 (SD 23.9) – 40 (2) No postoperative complications Retrospective nature, small sample size, delayed TTT Kellner et al51 Retrospective case series SCUBA with Apollo System 47 – – 42.6 (SD 29.7) 88.2% (SD 20.8) – Bleeding: IO,6.4% (n=3) and PO, 2.1% (n=1). Functional outcome /ICH characteristics not in article Goyal et al49 Retrospective case–control study Apollo System 18 – 2.2 (SD 0.9) 40 (range: 21–52) 60% (median: 24 cm3) 28 – Retrospective, assessment of imaging ICH volumes not adjudicated. Disparities in withdrawal of care Catheter-based pharmacological techniques Hanley et al57 Multicentre, phase II clinical trial MISTIE II 96 (54 MIS +alteplase, 42 SMC) Admission GCS: 3–8 pts (n=17), 9–12 pts (n=12), 13–15 pts (n=17) – 48.2 (SD 19.6) 57% (SD 25) 9.50 Symptomatic bleeding (n=5), asymptomatic haemorrhage (n=3) Small trial size and low screening yield. Did not evaluate efficacy Hanley et al58 Multicentre,
open-label
phase III clinical trialMISTIE III 499 (250 MIS+alteplase, 249 SMC) Admission GCS: 3–8 pts (n=64), 9–12 pts (n=111), 13–15 pts (n=75 – 41.8 (range: 30.8–54.5) 69% 9 Symptomatic bleeding (n=6), bacterial infections (n=2)
30% serious adverse event at 30 daysOpen-label design, use of different sizes and surgeons to perform the procedure GCS, Glasgow Coma Scale; ICH, intracerebral haemorrhage; MIC, minimally invasive surgery; SMC, standard medical care.





{kind=link}
{kind=link}
{kind=link}
{kind=link}