

Abstract
Background Edaravone dexborneol is believed to be a novel cytoprotective drug, demonstrating a synergistic combination of antioxidative and anti-inflammatory properties in animal models. The Treatment of Acute Ischaemic Stroke with Edaravone Dexborneol (TASTE) trial demonstrated its superior efficacy over edaravone alone for acute ischaemic stroke (AIS) patients. However, its efficacy in individuals undergoing endovascular therapy (EVT) remains uncertain.
Aim To clarify the rationale and design of the TASTE II (TASTE-2) trial.
Design The TASTE-2 is a multicentre, double-blind, randomised, placebo-controlled trial designed to evaluate the efficacy and safety of edaravone dexborneol in patients with AIS and large-vessel occlusion in the anterior circulation. The eligible participants, presenting with a National Institute of Health Stroke Scale score between 6 and 25 (range 0–42, with larger values suggesting severe neurological dysfunction) and an Alberta Stroke Program Early Computed Tomography Score ranging from 6 to 10 (range 0–10, with smaller values suggesting larger infarction) within the initial 24 hours after symptom onset, will be randomly allocated to either the edaravone dexborneol group or the placebo group in equal proportions prior to thrombectomy. The treatment will be continuously administered for a duration of 10–14 days. A follow-up period of 90 days will be implemented for all participants.
Study outcomes The primary efficacy outcome is defined as achieving favourable functional independence, measured by a modified Rankin Scale of 0–2 at 90 days. The primary safety outcome focuses on the incidence of serious adverse events.
Discussion The TASTE-2 trial will provide evidence to determine whether the administration of edaravone dexborneol in AIS patients undergoing EVT could yield significant improvements in neurological function.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Edaravone dexborneol has been proved to be cytoprotective in improving functional outcome of acute ischaemic stroke (AIS) patients when compared with edaravone alone, however, whether it is efficacious and safe in AIS patients who will undergo endovascular therapy (EVT) remains unclear.
WHAT THIS STUDY ADDS
The treatment of acute ischaemic stroke with edaravone dexborneol II is the first phase III trial of edaravone dexborneol prior thrombectomy in AIS patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Data obtained from this trial will offer valuable evidence of edaravone dexborneol in AIS patients with EVT.
Introduction and rationale
Reperfusion therapy, namely intravenous thrombolysis (IVT) and endovascular therapy (EVT), has been highly recommended to individuals diagnosed with major ischaemic stroke (IS), particularly those with large-vessel occlusion (LVO), however, the proportion of unfavourable functional outcome remains as high as 54% in the five classical trials of EVT.1 Brain cytoprotection, formerly known as neuroprotechtion, had been highly expected to improve functional outcome of IS but failed to show their benefits so far in randomised clinical trials.2 3 Considering the rapid advancement of thrombectomy techniques and devices aimed at improving functional outcome in patients with LVOs effectively in the era of reperfusion and to have maximum impact of cytoprotectants, the Stroke Treatment Academic Industry Roundtable (STAIR) recommended to clinically evaluate cytoprotective agents alongside reperfusion therapy, for which multiple mechanisms of brain ischaemia or reperfusion injury had been elucidated.4–6 Therefore, a strategy using multitarget cytoprotectant agents which act through various synergistic mechanisms to prevent ischaemic injury was recommended with priority.4–6
Edaravone, approved to treat amyotrophic lateral sclerosis by the US Food and Drug Administration, has proven to be cytoprotective through early scavenging of free radicals and later exerting anti-inflammatory effects to promote functional recovery and structural integrity in reperfusion animal models.7–9 Furthermore, a retrospective observational study has shown that edaravone was associated with greater functional independence in stroke patients who underwent EVT.10 While (+)-borneol was estimated to have potent cytoprotective effects through multiple mechanisms in IS models, like inhibiting neuronal excitotoxicity through potentiating ɑ2/ɑ3-containing GABAA receptors, regulating the expression of nitric oxide synthase, suppressing Ca2+ overload and reducing the release of reactive oxygen species.11–14 Being combined together with a ratio of 4:1, edaravone dexborneol has been demonstrated to be a brain cytoprotective agent that exhibits synergistically antioxidative and anti-inflammatory effects and downregulating ferroptosis to attenuate reperfusion injury in preclinical models15–18 and has been proved to be efficacious in improving functional recovery among IS patients within 48 hours when compared with edaravone alone in Treatment of Acute Ischaemic Stroke (AIS) with Edaravone Dexborneol (TASTE) trial.19 However, whether it is cytoprotective as a whole in those patients who are treated with EVT has not been confirmed.
Therefore, we launched the TASTE II (TASTE-2) trial to test the efficacy and safety of edaravone dexborneol in improving functional outcome for those patients undergoing EVT because of LVO.
Methods
Study design and patient population
The TASTE-2 is a multicentre, double-blind, randomised, placebo-controlled trial aiming to evaluate the efficacy and safety of edaravone dexborneol in AIS individuals who will receive EVT. All enrolled patients will be randomised with 1:1 to edaravone dexborneol or placebo within 24 hours of symptom onset and receive continuous application for 10–14 days. All these participants will receive standard medical care afterwards and be followed up for 3 months (figure 1).

TASTE-2 study design. EVT, endovascular therapy; mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; TASTE-2, Treatment of Acute Ischaemic Stroke with Edaravone Dexborneol II.
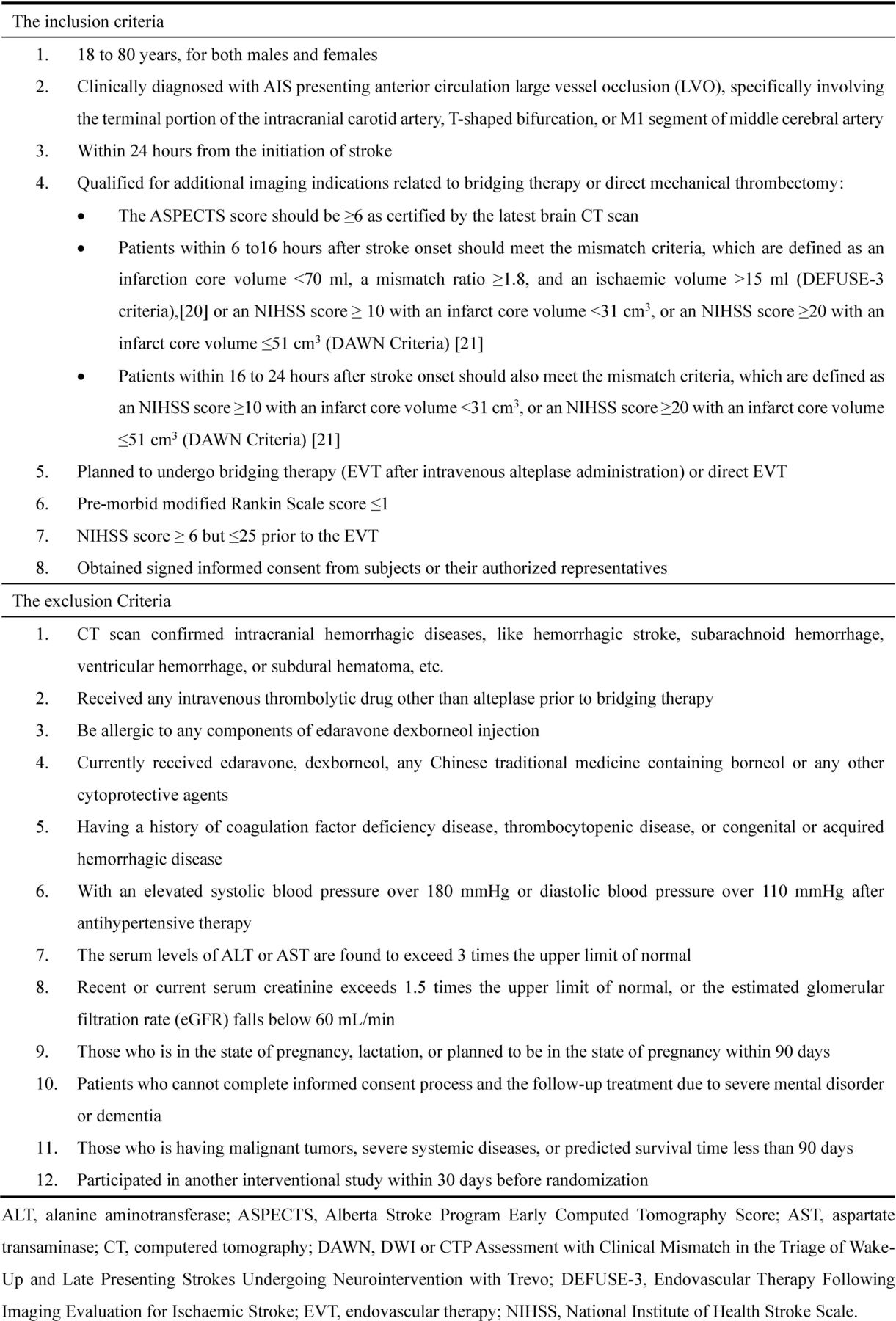
This trial will include patients who are diagnosed with AIS, aged between 18 and 80 years, with a National Institutes of Health Stroke Scale (NIHSS) score between 6 and 25 (range 0–42, with lager values suggesting severe neurological dysfunction) and an Alberta Stroke Program Early Computed Tomography Score (ASPECTS) of 6–10 (range 0–10, with smaller values suggesting larger infarction). All these patients should be characterised with an anterior LVO at intracranial internal carotid artery, T-shaped bifurcation or the M1 segment of middle cerebral artery and are to undergo treatment with EVT within 24 hours after symptom onset, however, prior or concomitant IVT with alteplase is not prohibited if indicated. Additionally, an imaging evaluation of mismatch should be performed through an automated software and the criteria of DEFUSE-320 or DAWN21 should be met for those within 6–24 hours after symptom onset. This software will be used to calculate the infarct core volume, mismatch ratio and mismatch volume (figure 2), of which rationale and details (Patents no. ZL202110266924.6 and ZL202110226735.6) has been described elsewhere.22

The inclusion and exclusion criteria of the TASTE-2 trial. TASTE-2, Treatment of Acute Ischaemic Stroke with Edaravone Dexborneol II.
Patients will be excluded if CT scan indicating intracranial haemorrhagic diseases, being given any IVTs other than alteplase before EVT, being allergic to any components of edaravone dexborneol injection, having a history of congenital or acquired haemorrhagic disease, with an elevated systolic blood pressure surpassing 180 mm Hg or diastolic blood pressure exceeding 110 mm Hg after therapy, being in cases where the serum levels of alanine aminotransferase or aspartate transaminase are found to exceed three times the upper limit of normal, or if the current serum creatinine exceeds 1.5 times the upper limit of normal, or if the estimated glomerular filtration rate falls below 60 mL/min, etc (figure 2). Patients who have recently been administered or are currently receiving any Chinese traditional medicine containing borneol should also be excluded. Prior to enrolling patients, the trial must receive the endorsement from the Institutional Review Board at Beijing Tiantan Hospital, Capital Medical University and it is imperative to obtain written informed consent from every participant or their legally designated representative.
Randomisation
The randomisation sequence will be produced by SAS V.9.4 software at the Statistical and Data Center of the National Clinical Research Center for Neurological Diseases in China prior to the trial’s commencement, using a fixed-size block randomisation method. Each unique sequence number will be uniformly labelled on all the packages of the drug thereafter. This number will serve as the identifier of the drug in the smallest packaging unit and does not contain group information. All packaged drugs will be mailed to each site in randomisation sequence order with a minimum of one block. The eligible patients will be stratified based on the participating hospitals and randomly allocated to either the edaravone dexborneol group or the placebo group in equal proportions. After randomisation, the interventional drug should be given as soon as possible before the EVT is performed. Blinding will be maintained throughout the study.
Intervention
Patients allocated to the intervention group will be given intravenous edaravone dexborneol 37.5 mg, comprising 30 mg of edaravone and 7.5 mg of (+)-dexborneol, two times a day over a consecutive period of 10–14 days lasting for 30 min each time. Meanwhile, patients allocated to the control group will be given intravenous placebo of edaravone dexborneol in the same manner. The placebo contains all ingredients except the active edaravone and (+)-dexborneol. The first dose injection of edaravone dexborneol or placebo must precede the treatment of EVT and no later than the puncture of femoral artery. IVT with alteplase will not be prohibited neither before nor after randomisation if indicated. For this trial, EVT will be performed as a fundamental treatment and the reperfusion status of occluded large vessels will be evaluated using the 7-point extended Thrombolysis in Cerebral Infarction (eTICI) scoring system, and a higher eTICI score suggests a more significant reperfusion. Successful reperfusion is determined by reaching an eTICI score of 2b50 or higher, indicating a minimum of 50%–66% restoration of blood flow.23 Other standard of care can be used in both groups except those drugs that seem to be brain cytoprotective.
Outcomes
The primary efficacy outcome is defined as achieving favourable functional independence, which is indicated by a modified Rankin Scale (mRS, a scale of 0–6, scores 0–2 representing independence and scores 3–6 indicating dependence or death) score of 0–2 at 90 days. This score will be assessed in person, or by a real-time video if a face-to-face visit is not feasible, by a certified rater who is blind to the group assignments. This rater will be trained periodically under a theoretical guidance.24 The secondary efficacy outcomes encompass shift analysis of mRS, excellent functional outcome characterised by an mRS score of 0–1 at 90 days, the change in NIHSS score from 10 to 14 days to baseline, a decrease of NIHSS score ≥4 from 10 to 14 days to baseline, and the occurrence of new ischaemic or haemorrhagic stroke within 90 days. The primary safety outcome is the proportion of serious adverse events (SAEs) that occur throughout the entire study period. The secondary safety outcomes include all-cause mortality within 90 days, symptomatic intracranial haemorrhage within 36 hours, deterioration in neurological deficit defined as a ≥4-point increase in the NIHSS score from day 1 to baseline, and the proportion of AEs within 90 days. All SAEs will be evaluated by an independent clinical events committee. The study will also involve the collection of blood samples for further investigation into potential mechanisms (table 1).
The assessment flow chart
Data Safety and Monitoring Board
To uphold ethical standards and prioritise patient safety, the data safety and monitoring board (DSMB) will convene according to the established protocol to carefully monitor the trial’s progress. The DSMB, consisting of non-trial participants, will be entrusted with specific responsibilities outlined by the trial executive committee before its commencement. Following each meeting, DSMB will furnish written recommendations to the trial steering committee chairs.
Sample size
According to the findings of the TASTE trial,19 the edaravone dexborneol group showed a 13.9% relative increase in neurological improvement compared with the edaravone alone group. Taking into account the positive effect of edaravone as a control in the TASTE trial, it is assumed that there will be a 20% relative increase in neurological improvement when comparing edaravone dexborneol with placebo in the upcoming TASTE-2 trial. In ANGLE-ACT, a large cohort study including Chinese patients treated with EVT, 45.4% of patients achieved mRS scores of 0–2 within 90 days.25 Therefore, it is estimated that in TASTE-2, this proportion in the interventional group will be approximately 54% and 45% in the control group. Based on these assumptions, an estimated total sample size of 1362 patients (with a dropout rate of 5%) and an equal distribution of 681 patients per group will provide at least a power of 90% to detect superiority of edaravone dexborneol over placebo in improving neurological function at a two-sided alpha significance level of p=0.05.
Interim analysis
Given the safety report of edaravone dexborneol in clinical studies19 26 as well as the anticipated pace of trial inclusion in China, this study will not conduct interim analyses.
Statistical analyses
The primary efficacy evaluation will be conducted based on an intention-to-treat analysis, while the analysis of safety will use the safety dataset. Differences in the proportion of mRS 0–2 at 90-day between study groups will be assessed through a logistic regression model, with trial centres considered as a random effect. The results will be presented as OR with a 95% CI. Additionally, we will examine whether the treatment effects vary across predefined subgroups by testing the interaction effect between treatment and subgroup using logistic regression models. Similar strategies to those used for analysing the primary outcome will be applied to other categorical outcomes. For shift analysis, an ordinal logistic regression model will calculate a common OR along with its 95% CI for the ordinal 90-day mRS score. All hypothesis tests will adopt a two-sided alpha level of significant set at 0.05 (α=0.05).
A prespecified subgroup analysis will be conducted to assess heterogeneity of treatment effect, with subgroups defined based on the following variables: gender (male or female), age (≤65 or >65), medical history (hypertension, hypercholesterolaemia, diabetes mellitus, stroke and coronary heart disease status, separately) (yes or no), time interval between last known well and randomisation (≤6 hours or >6 hours), NIHSS score range (6–15 or >15), ASPECTS score range (8–10 or 6–7), mismatch(yes or no), bridging therapy administration before EVT procedure (with alteplase or without alteplase), location of LVO site within the intracranial internal carotid artery versus M1 segment of middle cerebral artery, and reperfusion status of occluded vessels after EVT procedure according to eTICI scale categories 2b-3 vs 0–2 a.
The statistical analyses will be conducted by using SAS V.9. 4 or a higher version of the statistical software, in accordance with a predetermined statistical analysis plan that we will provide before the database is unmasked and locked.
Study organisation
This study will be carried out within approximately a hundred centres around mainland China from February 2022 and last about 24 months. To control centre effect, each centre must be experienced in EVT and has performed at least 50 thrombectomy therapies in the past calendar year and the median door-to-puncture time must be ≤120 min. During the study, an exit mechanism will be performed. All patients included will be observed to check their reactions to the treatment and can withdraw the informed content at any time for any reason based on the principles of Good Clinical Practice. Responsibility for the trial’s organisation lies with the executive and steering committees. The executive committee, led by the principal investigator and assisted by the steering committee, will supervise all the trial activities including protocol development and amendment during the study period. The executive committee is situated at the TASTE-2 Trial Coordinating Centre, which is part of the China National Clinical Research Centre for Neurological Diseases. Meanwhile, the steering committee will consist of recognised experts in neurology and statistics, providing professional supervision and strategic advice. The committee is scheduled to convene semiannually. Trained assessors, who are unaware of the treatment assignment, will adjudicate outcomes, SAEs and brain imaging.
Version modification
The protocol V.1.0 underwent a minor modification, resulting in the current version being 1.1. In this updated version, we included shift analysis of mRS at 90 days as an additional measure of secondary efficacy outcome without any disruption or impact on the trial’s executive processes.
Discussion
TASTE-2 will address a significant challenge in providing cytoprotection during in-hospital prethrombectomy for AIS patients in the new era of reperfusion therapy. The rationale and design of this study are based on multiple preclinical and clinical studies, adhering to the STAIR recommendations.4–6 The two primary reperfusion treatments for brain ischaemia, namely thrombolysis and mechanical thrombectomy therapy, have the potential to yield favourable functional outcomes for patients by fully or partially restoring the blood flow within a suitable time window. However, considering the pathophysiology of recanalised blood flow, it may be worth exploring the use of a multitarget cytoprotectant as a viable intervention to mitigate subsequent injury caused by ischaemia and reperfusion.
Recently, the publication of the efficacy and safety of nerinetide for the treatment of AIS (ESCAPE-NA1) trial demonstrated that nerinetide, a postsynaptic density protein 95, did not improve functional outcomes for patients undergoing EVT when compared with placebo.27 The lack of positive outcome could potentially be explained by the plasmin-mediated enzymatic breakdown of nerinetide within the alteplase layer. In our search on PubMed and Web of Science for this trial design, we found no evidence suggesting edaravone dexborneol is affected by alteplase; however, experimental thrombosis models indicate edaravone can accelerate thrombolysis with alteplase.9 Therefore, patients with alteplase are not prohibited and the subgroup analysis of efficacy for patients with or without alteplase before EVT will be performed in this trial. Although DL-3-n-Butylphthalide, a new cytoprotectant, was demonstrated to be efficacious in improving functional outcome for patients with AIS receiving reperfusion therapy, the specific molecular mechanism of action of butylphthalide was unknown and the rate of EVT was rather low.28 An ongoing phase-III trial of a sublingual tablet containing edaravone dexborneol was designed to evaluate its efficacy and safety in terms of functional outcomes in AIS patients . However, the trial excluded patients undergoing EVT.29
In conclusion, TASTE-2 represents the pioneering phase-III trial designed to evaluate the efficacy and safety of edaravone dexborneol in AIS patients undergoing EVT. This study will generate robust data regarding the effectiveness of this cytoprotective drug in individuals receiving reperfusion treatment.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Central Institutional Review Board at Beijing Tiantan Hospital, Capital Medical University (KY2021-177-01). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Data and safety monitoring board: Hui Zhi (HK), Dongsheng Fan, Bin Peng. Independent adjudication committee: David Z. Wang (USA). Independent statistician: Yingyu Jiang.
Footnotes
X @hqgu
Contributors CW drafted the manuscript, CW, H-QG, QD, AX, NW, YY, FW and YW contributed to the study design and H-QG contributed to statistical analysis. All authors contributed to critical revision of the manuscript for important intellectual content. YW is the guarantor.
Funding This trial was funded by Simcere Pharmaceutical Group, the Ministry of Science and Technology of the People’s Republic of China (2022YFC2504902, 2022YFC2504904), the National Natural Science Foundation of China (81801152, 92046016), CAMS Innovation Fund for Medical Sciences (2019-I2M-5-029) and Beijing Municipal Committee of Science and Technology (Z201100005620010, Z211100002921064). All drugs and placebos were provided by Simcere Pharmaceutical Group.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References




{kind=link}
{kind=link}