

Abstract
Introduction The risk of disability and mortality is high among recurrent stroke, which highlights the importance of secondary prevention measures. We aim to evaluate medication persistence for secondary prevention and the prognosis of acute ischaemic stroke or transient ischaemic attack (TIA) in China.
Methods Patients with acute ischaemic stroke or TIA from the China National Stroke Registry II were divided into 3 groups based on the percentage of persistence in secondary prevention medication classes from discharge to 3 months after onset (level I: persistence=0%, level II: 0%<persistence<100%, level III: persistence=100%). The primary outcome was recurrent stroke. The secondary outcomes included composite events (stroke, myocardial infarction or death from cardiovascular cause), all-cause death and disability (modified Rankin Scale score=3–5) from 3 months to 1 year after onset. Recurrent stroke, composite events and all-cause death were performed using Cox regression model, and disability was identified through logistic regression model using the generalised estimating equation method.
Results 18 344 patients with acute ischaemic stroke or TIA were included, 315 (1.7%) of whom experienced recurrent strokes. Compared with level I, the adjusted HR of recurrent stroke for level II was 0.41 (95% CI 0.31 to 0.54) and level III 0.37 (0.28 to 0.48); composite events for level II 0.41 (0.32 to 0.53) and level III 0.38 (0.30 to 0.49); all-cause death for level II 0.28 (0.23 to 0.35) and level III 0.20 (0.16–0.24). Compared with level I, the adjusted OR of disability for level II was 0.89 (0.77 to 1.03) and level III 0.82 (0.72 to 0.93).
Conclusions Persistence in secondary prevention medications, especially in all classes of medications prescribed by the physician, was associated with lower hazard of recurrent stroke, composite events, all-cause death and lower odds of disability in patients with acute ischaemic stroke or TIA.
Introduction
Stroke is one of the most common causes of death and disability, and China has the greatest stroke burden in the world with 39.3% risk of lifelong stroke for people over 25 years old.1 After experiencing one ischaemic stroke event, the risk of recurrence and death remains high,2–4 thus highlighting the importance of taking secondary prevention medications to decrease the risk of recurrence and to improve clinical outcomes.5–7 At present, studies about secondary prevention medications focus on the status and influence factors of persistence after ischaemic cerebrovascular diseases in China.8 9 Studies have also shown that combined secondary prevention medications after discharge was associated with a decreased risk of outcomes in patients with coronary artery disease.10 11 However, little is known about the relationship between the continuation of individual secondary prevention medications or combined medications over a period of time after discharge and the prognosis of patients with acute ischaemic stroke or transient ischaemic attack (TIA) in China.
The aim of this study was to explore data from the China National Stroke Registry II (CNSR II) to investigate the association between secondary prevention medication persistence and the hazard of recurrent stroke, composite events, all-cause death and the odds of stroke disability after acute ischaemic stroke or TIA.
Methods
Study design
Launched in 2012 by the Ministry of Health of China, CNSR II is a registry study of acute cerebrovascular events in 219 hospitals, selected from eligible secondary and tertiary hospitals around China to undergo sentinel surveillance.12 All hospitals voluntarily participated in the study. From June 2012 to January 2013, patients who met the following criteria were enrolled: (1) age >18 years; (2) diagnosis within 7 days of the index ischaemic stroke event, TIA, spontaneous intracerebral haemorrhage or subarachnoid haemorrhage; (3) direct hospital admission from a physician’s clinic or emergency department; (4) informed consent provided by the patient or a legally authorised representative.
Data collection
Trained research coordinators reviewed medical records to identify patients who provided informed consent and were continuously enrolled in each hospital. Patient-level and hospital-level characteristics were collected from medical records. Patient-level characteristics included age, sex, ethnicity, education level, health insurance status, family income per month, medical history, status at admission and discharge, medications and in-hospital death. Health insurance in China includes urban basic medical insurance schemes, new rural cooperative medical schemes and commercial insurance. In addition, some people need to pay for medical fees at their own expense. Hospital-level characteristics included hospital grade, geographical region, teaching status, stroke unit, hospital beds and neurological ward beds. The regional distribution of hospitals is divided into eastern, central and western regions, according to the Chinese Health Statistics Yearbook.13 Discharge medication information involved the related medications taken by patients without allergies or contraindications, including antiplatelet medications, warfarin, statins, antihypertensive medications, antidiabetic medications and so on, and the dosages and frequencies of each medication. Trained third-party investigators conducted telephone follow-up at 3, 6 and 12 months after initial symptom onset to collect research data, while patients who cannot be contacted after multiple attempts were considered lost to follow-up.
Assessment of secondary prevention medication persistence
Persistence is often defined as the duration of treatment.14 15 In our study, persistence was defined as continuing secondary prevention medication(s) from discharge to 3 months after initial symptom onset. Patients who were prescribed a specific medication at discharge but discontinued that medication at 3 months were defined as ‘non-persistent’. Persistence to the medication class was defined in the same way, and the medication class included antiplatelet, warfarin, statins, antihypertensive and antidiabetic medications. Antiplatelet medications included aspirin, clopidogrel, ozagrel, dipyridamole, ticlopidine and cilostazol. Antihypertensive medications included beta-blockers, ACE inhibitors, angiotensin receptor blockers, calcium-channel blockers and diuretics. Antidiabetic medications included insulin and oral diabetic agents. Patients were still considered persistent if they stopped one medication but then took another medication in the same class during the 3-month period. Composite persistence was defined as the percentage (0% to 100%) of discharge medication classes that patients were still taking at 3 months.16 17 Based on the composite persistence, patients were divided into three groups (level I: persistence=0%; level II: 0%<persistence<100%; level III: persistence=100%). In addition, regimen persistence was referred to an all-or-none measure where patients were either persistent or non-persistent. Patients who continued all discharge medication classes at the 3-month follow-up were considered persistent, whereas patients who discontinued at least one class of discharge medications were considered non-persistent.16 17
Outcome assessment
The primary outcome was recurrent ischaemic or haemorrhagic stroke from 3 months to 1 year after initial symptom onset. Secondary outcomes included new composite vascular events (stroke, myocardial infarction or death from cardiovascular cause), all-cause death and stroke disability were assessed at 3, 6 and 12 months of follow-up. Specifically, disability was defined as modified Rankin Scale (mRS) score 3–5.
Statistical analysis
The baseline hospital-level and patient-level variables of different groups were analysed. Continuous variables were presented as medians with IQRs and categorical variables as frequencies and percentages. Continuous variables were analysed by the Wilcoxon rank-sum test and categorical variables by the χ2 test. Multivariate Cox regression models were used to assess differences in the hazard of having a recurrent stroke, composite events and all-cause death among groups. Multivariate logistic regression models were used to test disability (mRS=3–5) among groups, and the generalised estimating equations were used to account for in-hospital clustering. Two models were used. In the first model, only age and sex were adjusted. In the second model, all the potential confounding variables in hospital and patient level were adjusted. Time to the efficacy outcome for each group was shown in a Kaplan-Meier curve and compared by the log-rank test. All tests were two-tailed, and p values less than 0.05 were considered statistically significant. All statistical analyses were performed by using SAS (SAS Institute), V.9.3.
Results
Study population
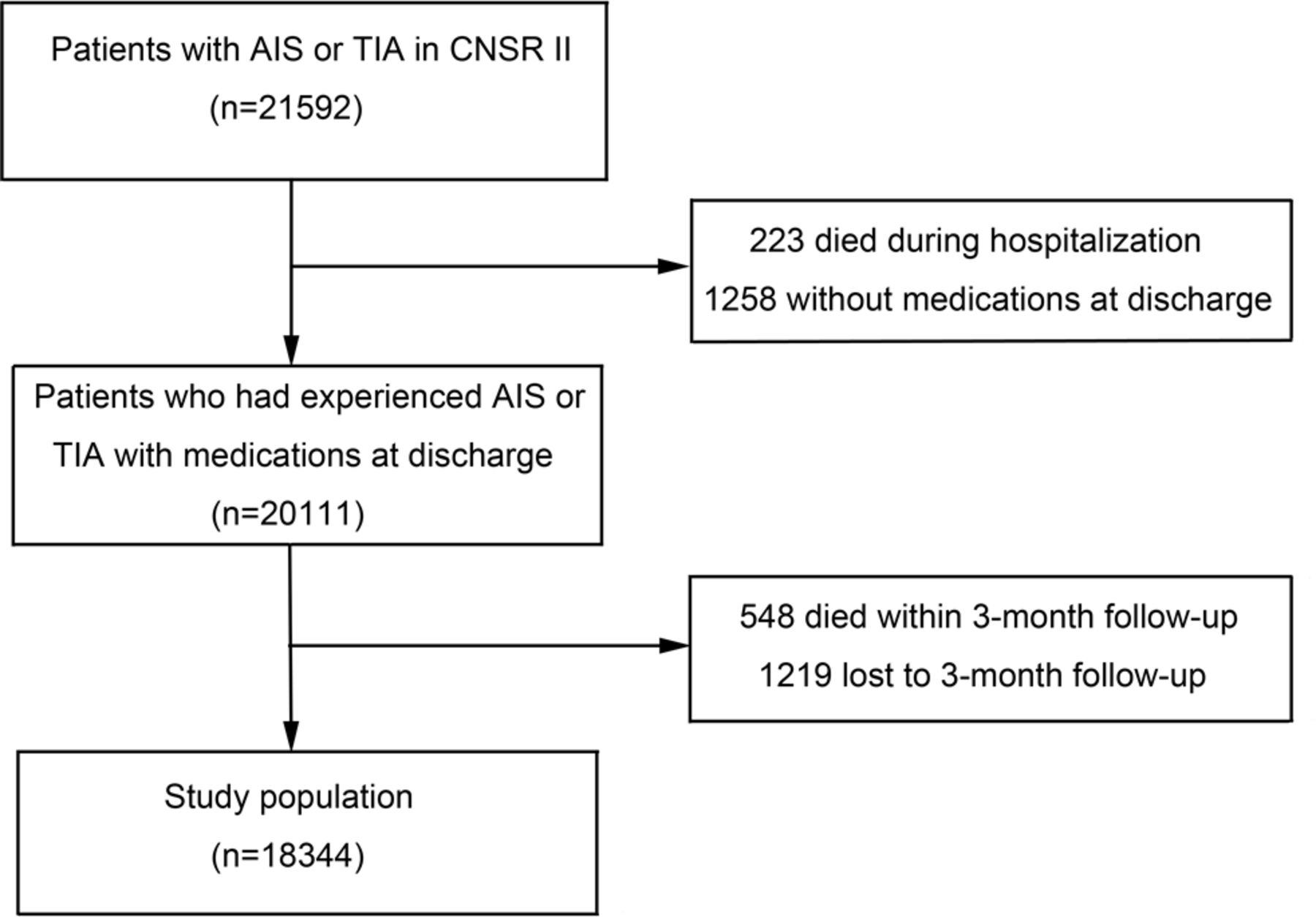
Out of 25 018 patients with ischaemic or haemorrhagic stroke in CNSR II, 21 592 were diagnosed with acute ischaemic stroke or TIA. We excluded 223 patients who died in the hospital, 548 patients who died before the 3-month follow-up, 1258 patients who were not prescribed medications at discharge and 1219 patients who were lost to follow-up at 3 months. A total of 18 344 patients were included in the final analytic sample (figure 1). Baseline characteristics of included and excluded patients in our study are shown in online supplemental table S5. The median age of study population was 64 (56–73) years. Of these patients, 6651 (36.3%) were female, 16 563 (90.3%) had an acute ischaemic stroke and 1781 (9.7%) had a TIA (table 1).
Supplementary data

Flowchart of the study. AIS, acute ischaemic stroke; CNSR II, China National Stroke Registry II; TIA, transient ischaemic attack.
Baseline characteristics in patient level and 3-month composite persistence of the study population
Patient-level characteristics and 3-month composite persistence
Baseline characteristics of the study population in patient level are shown in table 1. At 3 months after symptom onset, 46.2% of the study population were taking 100% of the prescribed discharge medications (level III), 29.8% were taking 0% to 100% (level II) and 24.0% were taking 0% (level I). Participants in the level III group were more likely to have higher levels of education, urban basic medical insurance schemes, higher family income per month, and a history of hypertension, diabetes, dyslipidaemia, non-atrial fibrillation or drinking. Participants in the level III group had lower admission National Institutes of Health Stroke Scale (NIHSS) scores, lower severity of illness at discharge and were more likely to have an ischaemic stroke as the index event (table 1).
Hospital-level characteristics and 3-month composite persistence
Baseline characteristics of the study population in hospital level are shown in table 2. Participants in the level III group were more likely to be treated in hospitals in the western region, hospitals with a stroke unit, hospitals with less than 1000 beds and hospitals with more than 80 beds in the neurological ward (table 2).
Baseline characteristics in hospital level and 3-month composite persistence of the study population
Outcomes by composite persistence
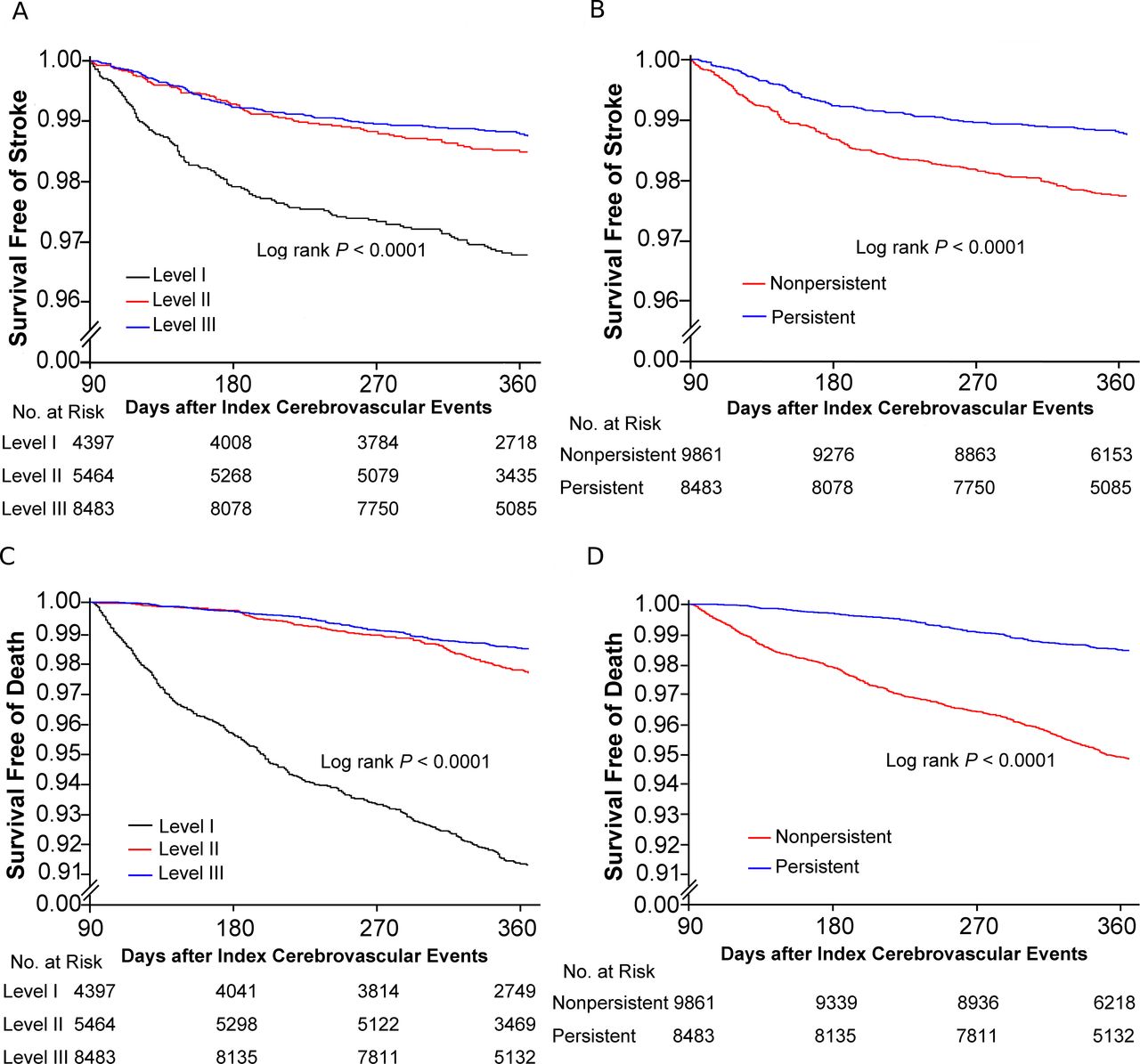
From 3 months to 1 year after onset, there were 315 (1.7%) new strokes, 381 (2.1%) composite events, 610 (3.3%) all-cause deaths and 2321 (14.0%) participants who progressed to stroke disability (mRS=3–5). Table 3 shows the association between 3-month composite persistence and clinical outcomes. Patients in the level III group had better outcomes from 3 months to 1 year after onset, including a lower hazard of recurrent stroke, composite events, all-cause death and lower odds of stroke disability. Compared with patients in the level I group, patients in the level II group had decreased hazard of recurrent stroke (HR 0.41, 95% CI 0.31 to 0.54), composite events (HR 0.41, 95% CI 0.32 to 0.53), all-cause death (HR 0.28, 95% CI 0.23 to 0.35) and decreased odds of stroke disability (OR 0.89, 95% CI 0.77 to 1.03). Patients in the level III group also had decreased hazard of recurrent stroke (HR 0.37, 95% CI 0.28 to 0.48), composite events (HR 0.38, 95% CI 0.30 to 0.49), all-cause death (HR 0.20, 95% CI 0.16 to 0.24) and decreased odds of stroke disability (OR 0.82, 95% CI 0.72 to 0.93) compared with those in the level I group. Kaplan-Meier curves for recurrent stroke or all-cause death by composite persistence are presented in figure 2. Meanwhile, the results of recurrent ischaemic or haemorrhagic stroke by 3-month composite persistence are shown in online supplemental table S6. There were 288 (1.6%) recurrent ischaemic strokes and 17 (0.09%) recurrent haemorrhagic strokes, among which one patient experienced both recurrent ischaemic and haemorrhagic stroke at the same time, and another 11 recurrent strokes (ischaemic or haemorrhagic not described in the database). Furthermore, we reclassified the patients based on the distribution of composite persistence and obtained similar results (online supplemental table S7).
Supplementary data
Supplementary data
Outcomes after ischaemic stroke or TIA by 3-month composite persistence

Probability of survival free of recurrent stroke or all-cause death after acute ischaemic stroke or transient ischaemic attack by the composite or regimen persistence. (A) Kaplan-Meier curves of survival free of recurrent stroke by the composite persistence. (B) Kaplan-Meier curves of survival free of recurrent stroke by the regimen persistence. (C) Kaplan-Meier curves of survival free of all-cause death by the composite persistence. (D) Kaplan-Meier curves of survival free of all-cause death by the regimen persistence.
Outcomes by regimen persistence
Similar associations between 3-month regimen persistence and clinical outcomes were observed after adjusting for covariates. Compared with non-persistent patients, those who were persistent had a decreased hazard of recurrent stroke (HR 0.57, 95% CI 0.45 to 0.73), composite events (HR 0.59, 95% CI 0.48 to 0.74), all-cause death (HR 0.32, 95% CI 0.26 to 0.39) and decreased odds of stroke disability (OR 0.87, 95% CI 0.79 to 0.97) (table 4). Kaplan-Meier curves for recurrent stroke or all-cause death by regimen persistence are presented in figure 2.
Outcomes after ischaemic stroke or TIA by 3-month regimen persistence
Outcomes by persistence in secondary prevention medication class
Persistence at 3 months after initial symptom onset for patients taking antiplatelet medications was 66.35%, followed by those taking warfarin (63.16%), statins (37.85%), antihypertensive medications (69.84%) and antidiabetic medications (71.82%) (online supplemental figure 3). Compared with those who were non-persistent, the hazard of recurrent stroke decreased in those who were persistent in taking antiplatelets (HR 0.52, 95% CI 0.41 to 0.66), statins (HR 0.67, 95% CI 0.46 to 0.99), antihypertensives (HR 0.47, 95% CI 0.35 to 0.62) and antidiabetics (HR 0.40, 95% CI 0.25 to 0.64) (online supplemental table S8). Associations between 3-month persistence by class and outcomes including composite events, all-cause death and stroke disability (mRS=3–5) are also shown in online supplemental table S8.
Supplementary data
Supplementary data
Discussion
In this cohort study using data from CNSR II, we found that persistence in secondary prevention medications, especially in all classes of medications prescribed by the physician, was associated with a decreased risk of recurrent stroke in patients with acute ischaemic stroke or TIA. Compared with level I patients, level III patients had significant relative risk reductions in stroke (63%), composite events (62%), all-cause death (80%) and stroke disability (18%) from 3 months to 1 year after initial symptom onset. Of note, new strokes were also reduced by 59% in patients in the level II group.
Closely related to outcomes of ischaemic stroke and TIA, secondary prevention medication persistence is suboptimal, especially in developing countries like China.8 17–19 Furthermore, reliable data on the potential influence of secondary prevention medication persistence on the prognosis of patients with acute ischaemic stroke or TIA in China are limited. Studies have indicated that persistence in antithrombotics, antihypertensives or statins can reduce adverse outcomes and improve the long-term prognosis of patients who had a stroke.20–25 However, these studies did not assess the impact of combined secondary prevention medication classes on stroke outcomes. Tan et al 26 only investigated the association between secondary prevention medication persistence and the clinical outcomes of acute minor stroke (NIHSS score ≤5). Though the median NIHSS score was low in our study, all the patients with ischaemic stroke and TIA were included, thus making our study more representative. The REduction of Atherothrombosis for Continued Health (REACH) Registry study showed that adherence of secondary prevention medications significantly decreased the risk of vascular events and all-cause mortality in patients with atherosclerosis.27 Park and Ovbiagele28 found that optimal combination of secondary prevention medication classes including antihypertensives, lipid modifiers and antithrombotics after a recent non-cardioembolic stroke was associated with a significantly lower risk of stroke. Our study also indicated that combined secondary prevention medication classes including antiplatelets, warfarin, statins, antihypertensives and antidiabetics can significantly decrease the risk of adverse events after stroke. The results of these two studies are consistent and can provide clinical value to the precision medicine. Compared with Park’s study, our study was more comprehensive. Patients with cardioembolic stroke or TIA were included, and the large-sample and multi-centre design allowed us to conduct subgroup analysis for persistence in various medications. Furthermore, we assessed the impact of combined secondary prevention medications on stroke outcomes, while hospital-level and patient-level confounders were also taken into account.29 30
Our study showed that persistence in secondary prevention medications, especially in all classes of medications prescribed by the physician, can significantly decrease the risk of adverse events after stroke. These findings support the current guidelines set by the Chinese Stroke Association and the American Stroke Association on secondary prevention. Secondary prevention is an important part of the comprehensive strategy for stroke prevention, and all appropriate secondary prevention medications should be prescribed and continued for eligible patients who have experienced an ischaemic stroke or TIA.
There are several limitations in our study. Since the hospitals participated in this study were voluntary, compared with other hospitals, they may have more motivations which may lead to better outcomes. Persistence is often defined as the duration of treatment, while adherence is often defined as the extent to which patients took medications according to the provider’s advice.14–17 Our study analysed the association between stroke prognosis and secondary prevention medication persistence, but not adherence. As such, we did not know whether patients stopped taking medications due to their provider’s instructions or due to other reasons. Furthermore, with the improvement of people’s living standards and awareness of stroke, more and more patients with mild symptoms go to hospital for treatment as soon as possible. Despite representative as a whole, potential bias was unavoidable in this study since participants at admission had a median NIHSS score of 3. In addition, persistence was defined from discharge to 3 months, while the relevant data of factors such as blood pressure, glucose and lipids of the patients at 3 months were not collected, but these factors may confound the observed relationships. Finally, medication persistence and stroke outcomes were only analysed from 3 months to 1 year after onset. Further studies are needed to determine the association between secondary prevention medications and long-term stroke outcomes.
Conclusions
Persistence in secondary prevention medications, especially in all classes of medications prescribed by the physician, was associated with a lower hazard of recurrent stroke, composite events, all-cause death and lower odds of stroke disability in patients with acute ischaemic stroke or TIA. Our findings highlight the need to strengthen secondary prevention measures such as medication persistence through medical quality control as well as health education in the clinic and in the community, especially as the stroke burden in China increases in the coming decades.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Central Institution Review Committee of Beijing Tiantan Hospital (ID of the approval: 2011BA108B02).
Acknowledgments
We thank all participating hospitals, their doctors and nurses, and members of the China National Stroke Registry II Steering Committee.
Footnotes
Twitter @chelsealiu96
Contributors LZ, XM and YW contributed to the design of the study. ZL, JS, CL and WL contributed to the management of the study, literature search and draft writing. YP and HY contributed to the data cleansing and analysis.
Funding This work was supported by grants from National Key R&D Program of China (2018YFC1312903), National Science and Technology Major Project (2017ZX09304018), National Natural Science Foundation of China (81971091), Beijing Municipal Science & Technology Commission (D171100003017002, Z181100001818001), and Beijing Hospitals Authority Youth Programme (QML20190501).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
References





{kind=link}
{kind=link}