

Hot debates exist regarding whether patients who had an acute large vessel occlusion stroke (LVOS) can skip tissue plasminogen activator (tPA) and go directly to thrombectomy in comprehensive stroke centres. Three head-to-head randomised clinical trials (RCTs) of direct endovascular treatment (dEVT) versus bridge therapy (BT) with intravenous alteplase have been recently completed in the Asian population. The DIRECT-MT (Direct Intraarterial Thrombectomy in Order to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals: a Multicenter Randomized Clinical Trial) Study randomly enrolled 656 patients who had an acute ischaemic stroke with anterior circulation LVOS across 41 large teaching hospitals in China to receive BT or dEVT within 4.5 hours after symptom onset.1 The study showed that the dEVT group was non-inferior to BT in terms of 90-day clinical outcomes (median 90-day modified Rankin Scale (mRS), 3 vs 3; OR 1.07; 95% CI 0.81 to 1.40; p=0.04).1 Likewise, the recently published DEVT (Direct Endovascular Thrombectomy vs Combined IVT and Endovascular Thrombectomy for Patients With Acute Large Vessel Occlusion in the Anterior Circulation) trial involving 234 Chinese patients who had an anterior circulation LVOS found that the rate of functional independence (90-day mRS ≥2) in dEVT group was numerically higher than that in the BT group (54.3% vs 46.6%, difference: 7.7%, 1-sided 97.5% CI: −5.1% to ∞; p=0.003 for non-inferiority).2 With prespecified non-inferiority threshold of 10% for the favourable outcome proportion difference, the trial concluded that dEVT was non-inferior to BT.2 Simultaneously published with DEVT, the SKIP (Direct Mechanical Thrombectomy in Acute LVO Stroke) trial included 204 patients who had an acute ischaemic stroke with internal carotid artery or middle cerebral artery M1 occlusions presenting within 4.5 hours of stroke onset across 23 sites in Japan.3 Favourable outcome occurred in 60 patients (59.4%) in the dEVT group and 59 patients (57.3%) in the BT group, with no significant between-group difference (difference, 2.1% (1-sided 97.5% CI −11.4% to ∞); OR 1.09 (1-sided 97.5% CI 0.63 to ∞); p=0.18 for non-inferiority).3 Noted that the trial used a reduced dose of alteplase (0.6 mg/kg), which did not show the non-inferiority to standard dose of alteplase (0.9 mg/kg).4
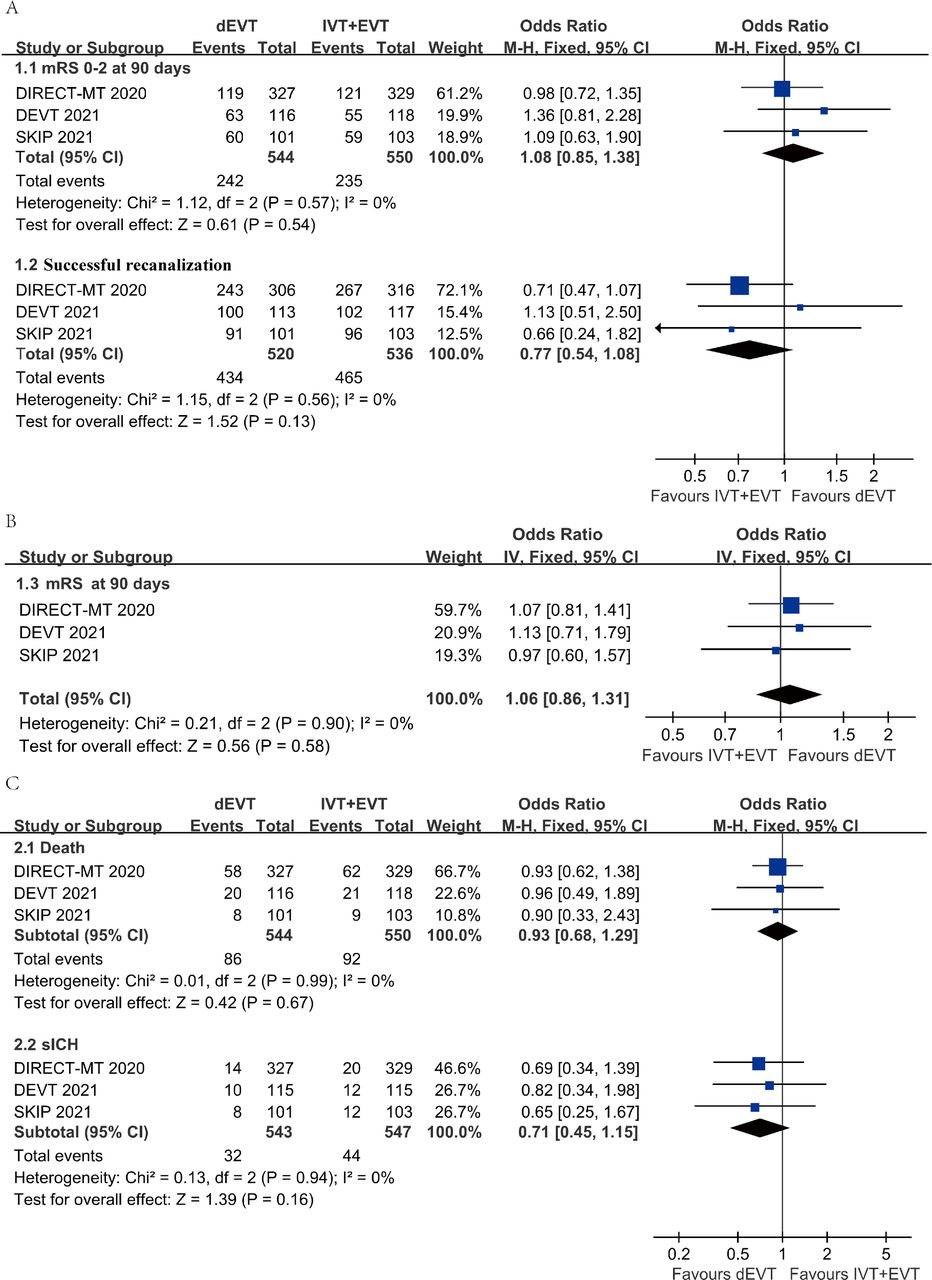
Herein, we provide an aggregate data meta-analysis of the DIRECT-MT,1 the DEVT2 and the SKIP3 trials. The OR for 90-day functional independence (90-day mRS 0–2) was 1.08 (95% CI 0.85 to 1.38) while the OR for any 1-point improvement across the disability scale (ordinal shift 90-day mRS) was 1.06 (95% CI 0.86 to 1.31). The percentage of achieving a Thrombolysis in Cerebral Infarction score 2b–3 was numerically higher in the bridging group, around 5% in DIRECT-MT1 and 3% in SKIP.3 The rates of successful recanalisation, 90-day mortality, and symptomatic intracerebral haemorrhage were not significantly different between the dEVT and the BT groups (figure 1).

Meta-analysis of the efficacy and safety outcomes of three randomised trials. (A) 1.1 mRS 0–2; 1.2 successful recanalisation (eTICI ≥2b in the DIRECT-MT1 and DEVT,2 and TICI ≥2b in the SKIP3; (B) 1.3 mRS at 90 days; (C) 2.1 death; 2.2 sICH (Heidelberg criteria in the DIRECT-MT1; NINDS criteria in the DEVT2 and the SKIP.3 dEVT, direct EVT; eTICI, expanded Thrombolysis in Cerebral Infarction; EVT, endovascular thrombectomy; IVT, intravenous thrombolysis; mRS, modified Rankin Scale; NINDS, National Institute of Neurological Disorders and Stroke; sICH, symptomatic intracerebral haemorrhage.
Merits and shortcomings
These trials were well-conducted head-to-head comparisons of dEVT with BT in tPA-eligible patients. There was no significant delay of door-to-puncture time between dEVT and BT groups across these trials, which facilitated the direct comparisons between these two strategies. However, there are some aspects related to the study design that deserve additional discussions when considering the clinical implications of these three trials.
A major concern for the direct endovascular thrombectomy is the generous boundary for non-inferiority margins of the three randomised trials.5 The DIRECT-MT1 set a 0.80 for OR, the SKIP3 set a 0.74 for OR as the non-inferiority margin, whereas the DEVT2 set a 10% absolute difference of proportion of favourable functional outcome as the non-inferiority margin. All the non-inferiority margins used in the three trials were clearly lower than the minimal clinically important differences (MCIDs) recommended by stroke expert survey studies, which suggested MCIDs of 3.5%–4.4% proportion of the functional independence and a stricter criterion of 1%–1.5% in novel endovascular thrombectomy devices trials for acute ischaemic stroke.6 Even lower boundary of CI of the combined OR based on the meta-analysis of the three randomised trials (figure 1) only marginally reached the suggested non-inferiority margin of OR 0.85 (corresponding to 4% proportion of the functional independence suggested by stroke expert survey studies, median of 3.5% and 4.4%). Therefore, the unequivocal non-inferiority of direct versus bridging endovascular thrombectomy remains controversial and requires further validation.
The door-to-needle times of DIRECT-MT,1 DEVT2 and SKIP3 were 59 (45–78) min, 61 (49–81) min and 50 min, respectively, which represent a substantial delay in relation to the 40 (29–55) min reported in the HERMES meta-analysis (Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials) and may have resulted in lower rates of favourable outcomes than what would have been accomplished with shorter door-to-needle times.7 Moreover, the rates of favourable outcomes noted in DIRECT–MT1 were significantly lower than those noted in DEVT2 and SKIP.3 This may be related to the differences of stroke aetiology across the trials with varying proportions of undetermined causes and intracranial atherosclerosis. Moreover, whether intravenous tPA infusion was completed in the bridging groups of these three trials prior to thrombectomy began was not reported.
Regarding patient populations studied, the three trials largely excluded drip-and-ship patients. Although SKIP3 allowed transfer, the interval between tPA and groin puncture in this trial was around 8 min, and therefore, it is fair to assume that the vast majority of patients presented directly. In the real world, intravenous tPA use is particularly efficient in drip-and-ship patients. The successful recanalisation rate of tPA for LVOS is between 10% and 40% depending on vessel size and timing of assessment,8 9 and it completely averts the need for endovascular treatment.
Notably, a recent meta-analysis summarising data of dEVT and BT across 30 studies involving 7191 patients in the BT group and 4891 patients in the dEVT group supported the continuous use of BT for eligible patients. Specifically, compared with patients in the dEVT group, patients in the BT group showed significantly better proportion of functional independence (mRS 0–2) at 90 days (OR 1.43 (95% CI 1.28 to 1.61)), had lower 90-day mortality (OR 0.67 (95% CI 0.60 to 0.75)), and achieved higher rates of successful recanalisation (modified Thrombolysis in Cerebral Ischemia score 2b–3) (OR 1.23 (95% CI 1.07 to 1.42)).10 However, we must acknowledge several limitations associated with the meta-analysis of observational studies. Only 5 out of the 30 studies in the meta-analysis were restricted to intravenous thrombolysis eligible patients and only one study (DIRECT-MT) had a randomised design. Importantly, this meta-analysis included a different patient population than the recent RCTs. In contrast to the three recent RCTs, transferred patients (a population where equipoise about BT clearly does not exist) were included in this meta-analysis. The meta-analysis also included wake-up and uncertain onset time strokes as well as posterior circulation occlusions. There were also remarkable differences in stroke severity with a median National Institutes of Health Stroke Scale score of only 10 in the meta-analysis vs 16–19 in the recent RCTs. The median Alberta Stroke Program Early CT Score was unexpectedly lower in the meta-analysis at 6 versus in the RCTs at 7–9 despite the higher stroke severity in the latter. Therefore, meta-analysis of the actual RCTs of dEVT and BT will be much more informative.
Future directions
While the current results do not necessarily support the dismissal of intravenous tPA in BT, they open up the opportunity for greater individualisation in the decision-making for patient who had LVOS presenting directly to thrombectomy-capable centres that can promptly perform endovascular treatment.5 In this context, BT may still be advantageous in a large proportion of patients but it might be reasonable to withhold tPA in certain situations such as those occlusions associated with very high clot burden (such as internal carotid artery occlusions), those with large baseline infarcts who may be at higher risk for intracerebral haemorrhage and those requiring stenting due to the need for dual antiplatelet agents. In addition, forgoing intravenous tPA reduces cost, which in many medical systems represents an important part of the decision-making process. Finally, it is critical to acknowledge the potential advantages of tenecteplase over tPA including easier and faster administration as well as higher rates of recanalisation in patients who had LVOS who are subsequently treated with thrombectomy.8 Therefore, in the future, additional exploration of BT remains valuable, especially with tenecteplase.
All patients were from Asia, which may not be generalised to other ethnic profiles. Additional ongoing RCTs comparing dEVT with BT including DIRECT-SAFE (A Randomized Controlled Trial of DIRECT Endovascular Clot Retrieval vs Standard Bridging Thrombolysis With Endovascular Clot Retrieval Within 4.5 Hours of Stroke Onset) in Australia and China (NCT03494920), SWIFT DIRECT (Solitaire With the Intention for Thrombectomy Plus Intravenous t-PA vs DIRECT Solitaire Stent-Retriever Thrombectomy in Acute Anterior Circulation Stroke) in Europe and Canada (NCT03192332), MR CLEAN-NO IV in the Netherlands (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands-No-Intravenous tPA; ISRCTN80619088) will hopefully provide more robust evidence.
Ethics statements
Patient consent for publication
Footnotes
Contributors YX and YP contributed equally. Manuscript draft and editorial design—YX and YP. Statistical analysis—YP. Critical revision of the manuscript—RGN, TGJ and ZR. Editorial design—YW.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.





{kind=link}