

Article Figures & Data
Figures
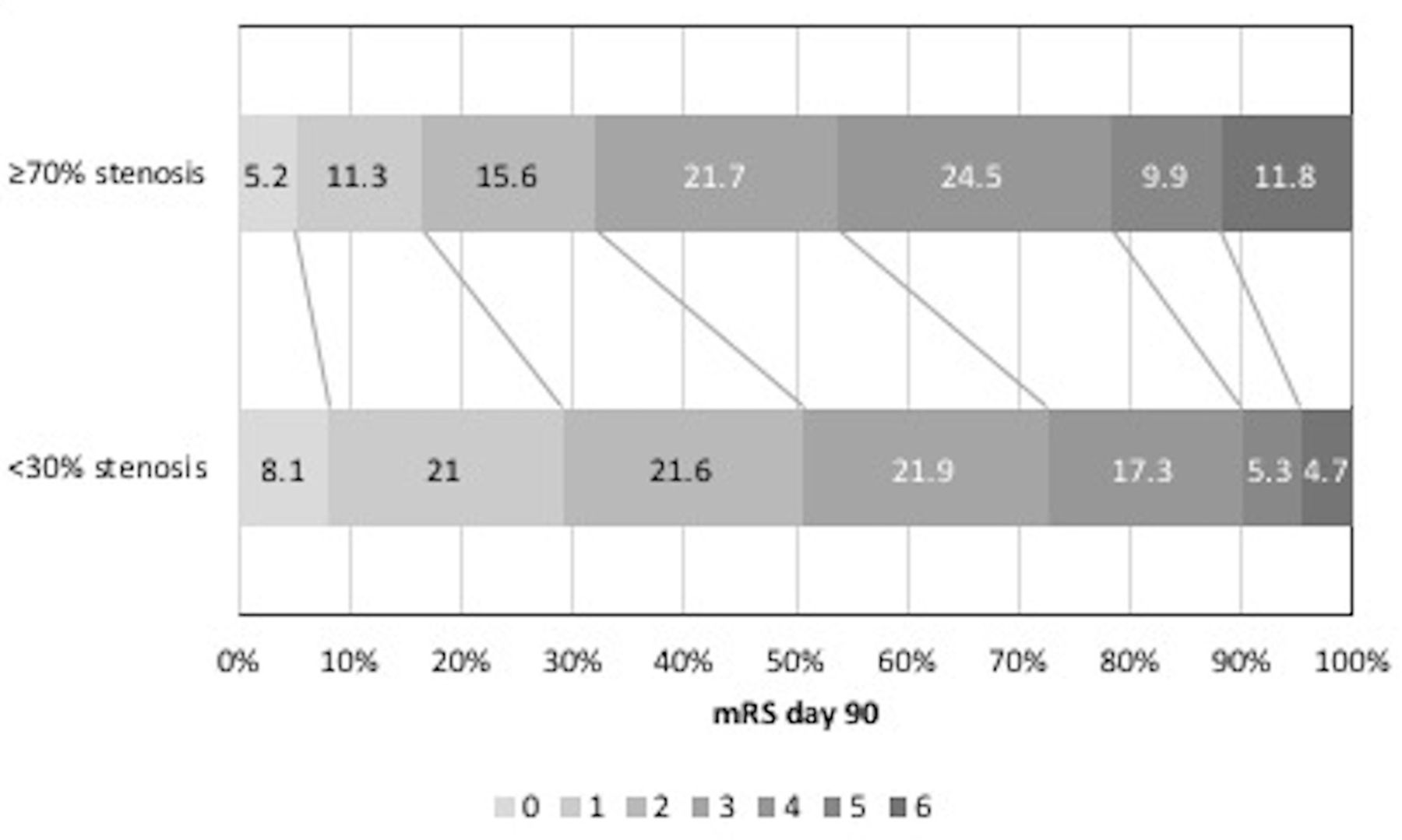
- Figure 1
mRS at day 90 <30% vs ≥70% ipsilateral stenosis. mRS, modified Rankin Scale.
- Figure 2
mRS at day 90 in those with ≥70% ipsilateral stenosis GTN versus no GTN. GTN, glyceryl trinitrate; mRS, modified Rankin Scale.


Tables
- Table 1
Baseline characteristics of all patients with ischaemic stroke with carotid data and by ipsilateral carotid stenosis
All IS GTN No GTN Continue Stop Stenosis <30% Stenosis 30–<50% Stenosis 50–<70% Stenosis ≥70% P value Number of patients 2023 1002 1021 534 525 1431 224 148 213 Age (years) 69.1 (11.4) 68.8 (11.3) 69.4 (11.5) 71.6 (10.5) 70.9 (10.5) 68.3 (11.6) 71.2 (10.7) 73.3 (9.9) 68.9 (10.8) <0.001 Sex, male (%) 1193 (59.0) 599 (59.8) 594 (58.2) 286 (53.6) 283 (53.9) 817 (57.1) 141 (62.9) 91 (61.5) 141 (66.2) 0.036 Premorbid mRS>1 (%) 209 (10.3) 95 (9.5) 114 (11.2) 71 (13.3) 64 (12.2) 135 (9.4) 27 (12.1) 20 (13.5) 24 (11.3) 0.29 Medical history (%) Hypertension 1307 (64.6) 624 (47.7) 683 (66.9) 512 (95.9) 503 (95.8) 903 (63.1) 146 (65.2) 108 (73.0) 144 (67.6) 0.078 Treated hypertension 1072 (53.0) 516 (51.5) 556 (54.5) 533 (99.8) 522 (99.4) 720 (50.3) 134 (59.8) 98 (66.2) 115 (54.0) <0.001 Diabetes mellitus 353 (17.4) 164 (16.4) 189 (18.5) 125 (23.4) 121 (23.0) 245 (17.1) 38 (17.0) 38 (25.7) 28 (13.1) 0.020 Atrial fibrillation 333 (16.5) 169 (16.9) 164 (16.1) 135 (25.3) 116 (22.1) 224 (15.7) 43 (19.2) 36 (24.3) 30 (14.1) 0.024 Stroke 295 (14.6) 150 (15.0) 145 (14.2) 113 (21.2) 97 (18.5) 207 (14.5) 37 (16.5) 25 (16.9) 22 (10.3) 0.22 TIA 286 (14.1) 147 (14.7) 139 (13.6) 91 (17.0) 96 (18.3) 179 (12.5) 43 (19.2) 24 (16.2) 39 (18.3) 0.010 IHD 380 (18.8) 191 (19.1) 189 (18.5) 136 (25.5) 153 (29.1) 248 (17.3) 59 (26.3) 38 (25.7) 34 (16.0) 0.001 PAD 65 (3.2) 29 (2.9) 36 (3.5) 23 (4.3) 22 (4.2) 35 (2.4) 10 (4.5) 8 (5.4) 12 (5.6) 0.018 Hyperlipidaemia 587 (29.0) 293 (29.2) 294 (28.8) 204 (38.2) 216 (41.1) 412 (28.8) 60 (26.8) 52 (35.1) 57 (26.8) 0.29 Smoking, current 573 (28.3) 278 (27.7) 295 (28.9) 111 (20.8) 109 (20.8) 380 (26.6) 71 (31.7) 37 (25.0) 83 (39.0) 0.010 Alcohol >21 units per week 176 (8.7) 92 (9.2) 84 (8.2) 38 (7.1) 29 (5.5) 116 (8.1) 19 (10.9) 11 (7.4) 28 (13.1) 0.10 Side of lesion, right (%) 1047 (51.8) 509 (50.8) 538 (52.7) 278 (52.4) 264 (50.4) 722 (50.5) 109 (48.7) 89 (60.1) 127 (59.6) 0.010 NIHSS (/42), calculated 9.9 (5.3) 9.8 (5.3) 10.0 (5.4) 10.3 (5.5) 10.2 (5.4) 9.7 (5.2) 10.1 (5.4) 9.6 (5.0) 11.6 (5.6) <0.001 GCS <15 (%) 460 (22.7) 222 (22.2) 238 (23.3) 134 (25.1) 145 (27.6) 300 (21.0) 61 (27.2) 32 (21.6) 65 (30.5) 0.006 TOAST classification* Cardioembolic 358 (17.7) 181 (18.1) 177 (17.3) 133 (24.9) 117 (22.3) 271 (18.9) 41 (18.3) 24 (16.2) 22 (10.3) 0.021 Large vessel 527 (26.1) 254 (25.3) 273 (26.7) 143 (49.5) 146 (27.8) 200 (14.0) 53 (23.7) 90 (60.8) 180 (84.5) <0.001 Small Vessel 808 (39.9) 402 (40.1) 406 (39.8) 188 (35.2) 199 (37.9) 649 (45.4) 105 (46.9) 34 (23.0) 16 (7.5) <0.001 Other 394 (19.5) 202 (20.2) 192 (18.8) 93 (17.4) 87 (16.6) 333 (23.3) 32 (14.3) 17 (11.5) 12 (5.6) <0.001 Haemodynamics BP, systolic (mm Hg) 166.6 (18.5) 167.1 (18.3) 166.1 (18.7) 165.4 (18.9) 167.7 (17.8) 166.6 (18.6) 166.6 (18.7) 165.1 (17.2) 167.5 (18.3) 0.70 BP, diastolic (mm Hg) 89.2 (13.0) 89.9 (13.1) 88.5 (12.8) 87.5 (13.3) 88.2 (12.6) 90.1 (13.0) 88.2 (13.3) 87.7 (12.9) 86.7 (11.8) <0.001 Heart rate (bpm) 76.8 (14.4) 77.1 (14.5) 76.5 (14.2) 75.8 (14.5) 76.1 (14.5) 76.5 (14.6) 78.4 (13.1) 78.7 (15.4) 75.3 (13.1) 0.039 Time to randomisation [hours] 25.6 [21.2] 24.9 [21.5] 26.0 [21.1] 25.2 [18.8] 23.9 [22.1] 26.0 [21.6] 24.0 [20.1] 23.9 [17.8] 24.8 [19.0] 0.08 Thrombolysis (%) 239 (11.8) 107 (10.7) 132 (12.9) 71 (13.3) 63 (12.0) 156 (10.9) 24 (10.7) 20 (13.5) 39 (18.3) 0.015 ↵*Total may exceed 100% due to mixed causality. χ2 test for categorical variables or one-way analysis of variance for continuous variables across grades of carotid stenosis.
BP, blood pressure; GCS, Glasgow Coma Scale; GTN, glyceryl trinitrate; IHD, ischaemic heart disease; mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; PAD, peripheral arterial disease; TIA, transient ischaemic attack.
- Table 2
Functional outcome and death at day 90 by degree of ipsilateral carotid stenosis
Stenosis <30% Stenosis 30–<50% Stenosis 50–<70% Stenosis ≥70% n (%)
/median [IQR]OR (95% CI) P value n (%)
/median [IQR]OR (95% CI) P value n (%)
/median [IQR]OR (95% CI) P value Number of participants 1431 224 – – 148 – – 213 – – mRS (/6)* 2 [3] 2 [2] 1.03 (0.80 to 1.33) 0.83 3 [2] 1.21 (0.89 to 1.64) 0.23 3 [2] 1.88 (1.44 to 2.44) <0.001 Death (%) 67 (4.7) 21 (9.4) 1.85 (1.06 to 3.22) 0.030 11 (7.4) 1.43 (0.71 to 2.90) 0.32 25 (11.8) 2.52 (1.48 to 4.27) 0.001 Data are n (%), median (IQR) or OR with 95% CIs. Comparison using logistic or ordinal regression with <30% stenosis as reference group. Adjusted for age, sex, baseline mRS, history of previous stroke, history of diabetes mellitus, TACS, nitrate use, baseline SSS, thrombolysis, feeding status, time to randomisation, baseline SBP, GTN/no GTN and continue/stop.
*Ordinal logistic regression.
GTN, glyceryl trinitrate; mRS, modified Rankin Scale; SSS, Scandinavian Stroke Scale.
- Table 3
Functional outcome and death at day 90 by randomised treatment by degree of ipsilateral carotid stenosis
Stenosis 30–<50% Stenosis 50–<70% Stenosis ≥70% GTN No GTN OR (95% CI) P value GTN No GTN OR (95% CI) P value GTN No GTN OR (95% CI) P value Number of participants 102 122 – – 77 71 – – 94 119 – – mRS (/6)* 2 [3] 3 [2] 0.77 (0.47 to 1.27) 0.31 3 [2] 3 [2] 0.71 (0.39 to 1.31) 0.28 3 [2] 4 [2] 0.56 (0.34 to 0.93) 0.024 Death (%) 7 (6.9) 14 (11.5) 0.43 (0.14 to 1.32) 0.14 3 (3.9) 8 (11.3) 0.18 (0.03 to 1.03) 0.054 9 (9.7) 16 (13.4) 0.63 (0.23 to 1.75) 0.37 Continue Stop Continue Stop Continue Stop Number of
participants65 68 – – 52 47 – – 57 57 – – mRS (/6)* 2 [3] 2.5 [3] 0.93 (0.48 to 1.80) 0.82 3 [2] 3 [2] 1.92 (0.86 to 4.27) 0.11 4 [3] 4 [3] 1.46 (0.73 to 2.93) 0.29 Death (%) 9 (13.8) 7 (10.3) 1.59 (0.42 to 6.01) 0.49 6 (11.5) 1 (2.1) 81.00 (1.08 to 6093.98) 0.046 12 (21.4) 6 (10.5) 3.11 (0.85 to 11.44) 0.09 Data are n (%), median (IQR) or OR with 95% CIs. Comparison using logistic or ordinal regression. Adjusted for age, sex, baseline mRS, history of previous stroke, history of diabetes mellitus, TACS, nitrate use, baseline SSS, thrombolysis, feeding status, time to randomisation, baseline SBP and continue/stop or GTN/no GTN, respectively.
*Ordinal logistic regression.
GTN, glyceryl trinitrate; mRS, modified Rankin Scale; SBP, systolic blood pressure; SSS, Scandinavian Stroke Scale; TACS, total anterior circulation syndrome.
Supplementary data





{kind=link}
{kind=link}