Chinese Stroke Association guidelines on emergency stroke unit
- 1 China National Clinical Research Center for Neurological Diseases, Beijing, China
- 2 Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
- 3 Department of Medicine & Therapeutics, The Chinese University of Hong Kong, Hong Kong, China
- 4 Department of Neurology, University of Illinois College of Medicine at Peoria, Peoria, IL, USA
- 5 National Center for Healthcare Quality Management in Neurological Diseases, Beijing, China
- Correspondence to Dr Yongjun Wang; yongjunwang{at}ncrcnd.org.cn
- Received 3 December 2024
- Accepted 3 December 2024
Abstract
Organised stroke care has become a keystone in delivering efficient and effective treatment to patients with stroke with improved outcomes. Delivering timely acute reperfusion therapy to those with acute ischaemic strokes is key to good recovery. Emergency stroke unit (ESU) is a novel organised stroke care system developed in China. It centralises all necessary procedures for the diagnosis and treatment of acute stroke into one unit that can perform clinical assessment, imaging examination and acute treatments. In ESU, artificial intelligence algorithms are used to aid in reading brain images and making clinical decisions. Therefore, ESU can significantly enhance the efficiency of emergent stroke care. In this guideline, we aim to clarify the concept, construction standards and personnel requirements of an ESU, standardise ESU-based acute stroke triage and treatment workflow, establish metrics of quality control, facilitate the construction and promotion of ESU and continue the improvement of the quality of stroke care.
- Stroke
Introduction
In 1995, the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study marked the beginning of the reperfusion therapy era for acute ischaemic stroke (AIS).1 ‘Time is brain’ has become a core concept in acute reperfusion therapy, emphasising on the importance of reducing delays of providing reperfusion therapy in order to save as much at-risk brain tissue as possible.
To improve the efficiency of reperfusion therapy, the American Brain Attack Coalition established the standards for stroke centre certification, aiming to ensure that patients with stroke receive efficient and standardised management at all stages (from prehospital identification to in-hospital treatment).2 In the past few years, systems of organised stroke care have significantly increased the efficiency of reperfusion therapy in AIS, but prehospital and in-hospital delays have not improved much in clinical practices. Previous studies have shown a loss of 1.9 million neurons and 14 billion synapses with every minute of delay from onset to reperfusion treatment,3 while every 30 min of delay could reduce the likelihood of a favourable outcome by 12%.4
To reduce prehospital delays, a novel organised stroke care model, the mobile stroke unit (MSU), was developed in Germany. It was based on an ambulance equipped with a small-sized, mobile CT and relevant equipment for acute stroke work-ups, aiming to provide thrombolysis on board if the CT of the head showed no haemorrhage. In the Berlin Prehospital Or Usual Delivery of acute stroke care5 and BEnefits of Stroke Treatment Delivered Using a Mobile Stroke Unit Compared with Standard Management by Emergency Medical Services (BEST-MSU)6 studies, MSU significantly reduced prehospital delays and increased the rate of intravenous thrombolysis (IVT) for patients with AIS.
However, compared with prehospital delays, in-hospital delays are more common since every hospital has challenges in space, imaging and laboratory capacities and personnel shortages, etc.7 In-house delay reduces the chance of successful recanalisation, especially in patients with AIS who need mechanical thrombectomy for large vessel occlusion (LVO) type of stroke.8
Establishing an in-hospital efficient and organised stroke care system is key to reducing in-hospital delays for reperfusion therapy. It has been identified that delayed brain imaging is one of the main causes of in-hospital delays, for example, approximately 39.5% of patients with stroke experience delays in receiving stroke imaging examinations/results.7 9 Therefore, we, here, propose a novel, in-hospital, organised stroke care model, the emergency stroke unit (ESU), which integrates the operations of clinical assessment, imaging examination and initial treatments into one unit/room. It aims to minimise in-hospital delays and facilitate rapid reperfusion treatment, and ultimately improve patient outcomes. To facilitate the construction and promotion of ESU across the country and continuous improvement of the quality of stroke care, experts from the Chinese Stroke Association developed this guideline.
Definition and impact of ESU
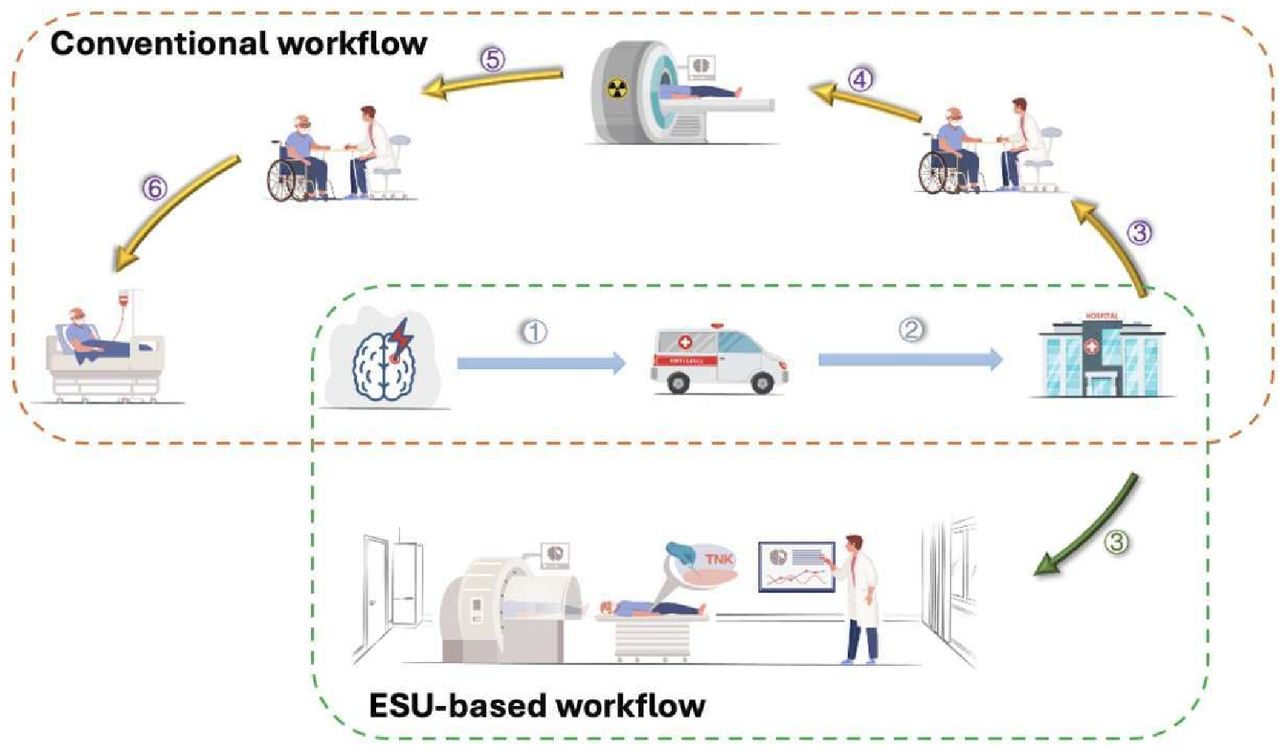
ESU is a stroke unit located in the emergency department. ESU integrates clinical assessment, brain imaging and initial treatments of patients with suspected stroke (figure 1). Compared with conventional workflow for a patient with AIS, ESU simplifies the procedures (figure 2). ESU aims to provide an integrated in-hospital acute stroke care system, which minimises in-hospital delays and provides rapid diagnosis and appropriate treatments within critical time windows for patients with AIS.

The layout of an emergency stroke unit.

Comparison of ESU-based workflow and conventional workflow for acute stroke patient triage and treatment. Conventional workflow: ① Stroke onset - ② arrival to a hospital - ③ initial clinical assessment - ④ transfer in CT/MRI room for imaging examination - ⑤ transfer out of CT/MRI room for further clinical assessment - ⑥ reperfusion therapy in eligible patients. ESU-based workflow: ① Stroke onset - ② arrival to a hospital - ③ one-stop clinical and imaging assessment, and initiation of reperfusion therapy in eligible patients. ESU, emergency stroke unit.
Configuration standards of an ESU
Equipment of ESU
ESU needs a dedicated area that could accommodate clinical assessment, brain imaging and provide initial treatments to patients with AIS. It is the first stop where a patient with possible stroke will be assessed. ESU should be clearly marked so that patients could be directed to ESU immediately on arrival to a hospital.
Mandatory equipment
Bedside brain imaging equipment: small, mobile brain imaging equipment capable of performing rapid and accurate brain imaging to diagnose an ischaemic stroke or intracerebral haemorrhage. Currently, a low-field (0.23T) MRI (made in China) is installed inside an ESU, which can detect an ischaemic stroke and with the Hematoma Enhanced Inversion Recovery (HEIR) sequence, intracerebral haemorrhage can be diagnosed. Its capability is similar to a 1.5/3.0T MRI.10 11
Artificial intelligence-based imaging analysis platform: This platform allows optimisation of the images (eg, improving the signal-to-noise ratio) and automatic analysis of image data (eg, automatic identification of the location, volume and nature of the lesions) which could assist in stroke diagnosis. It can also automatically assess Alberta Stroke Program Early CT Score (ASPECTS) score and diffusion-weighted imaging (DWI) - fluid-attenuated inversion recovery (FLAIR) mismatch, to guide clinical decisions.
Thrombolysis kit: The thrombolysis kit should contain intravenous thrombolytics (tenecteplase or alteplase) and antihypertensives (such as labetalol, sodium nitroprusside, hydralazine). It should also have a glucometer, needles, 0.9% sodium chloride solution and documents (such as treatment algorithm, National Institute of Health Stroke Scale (NIHSS) cards and instructions and weight-based dosing chart for thrombolytics).
Bed with a scale: It is recommended to integrate a bed with a scale to measure the patient’s body weight inside the brain imaging equipment, which can be used to calculate the dosage of intravenous thrombolytics.
Optional equipment
Bedside rapid genetic testing system that can provide the CYP2C19 genotype for personalised antiplatelet treatment in patients withAIS.
Intelligent wearable devices that can monitor patients’ vital signs, blood pressure, blood glucose and ECG in real time, and detect any arrhythmia such as atrial fibrillation.
Staff configuration in ESU
An ESU should be staffed with a 24/7 stroke team. The team should include a physician certified in treating AIS. This physician can assess the patient, review the indications for acute reperfusion treatment, make the treatment decisions and obtain informed consent. The team should also include a certified nurse, who obtains timely vital signs, performs rapid blood glucose testing, establishes an intravenous line and administers thrombolytics according to the protocol.
An ESU doctor must meet the following conditions: (1) completing at least 1 month training and practice of ESU-based IVT for patients with stroke; (2) proficiency in operating bedside brain imaging equipment (eg, low-field MRI scanner) and interpreting brain images with stroke-related lesions and vasculature (need to pass the examinations); (3) certified for ESU-based thrombolysis.
ESU-based stroke triage and treatment workflow and quality control
ESU-based emergency stroke triage and treatment workflow
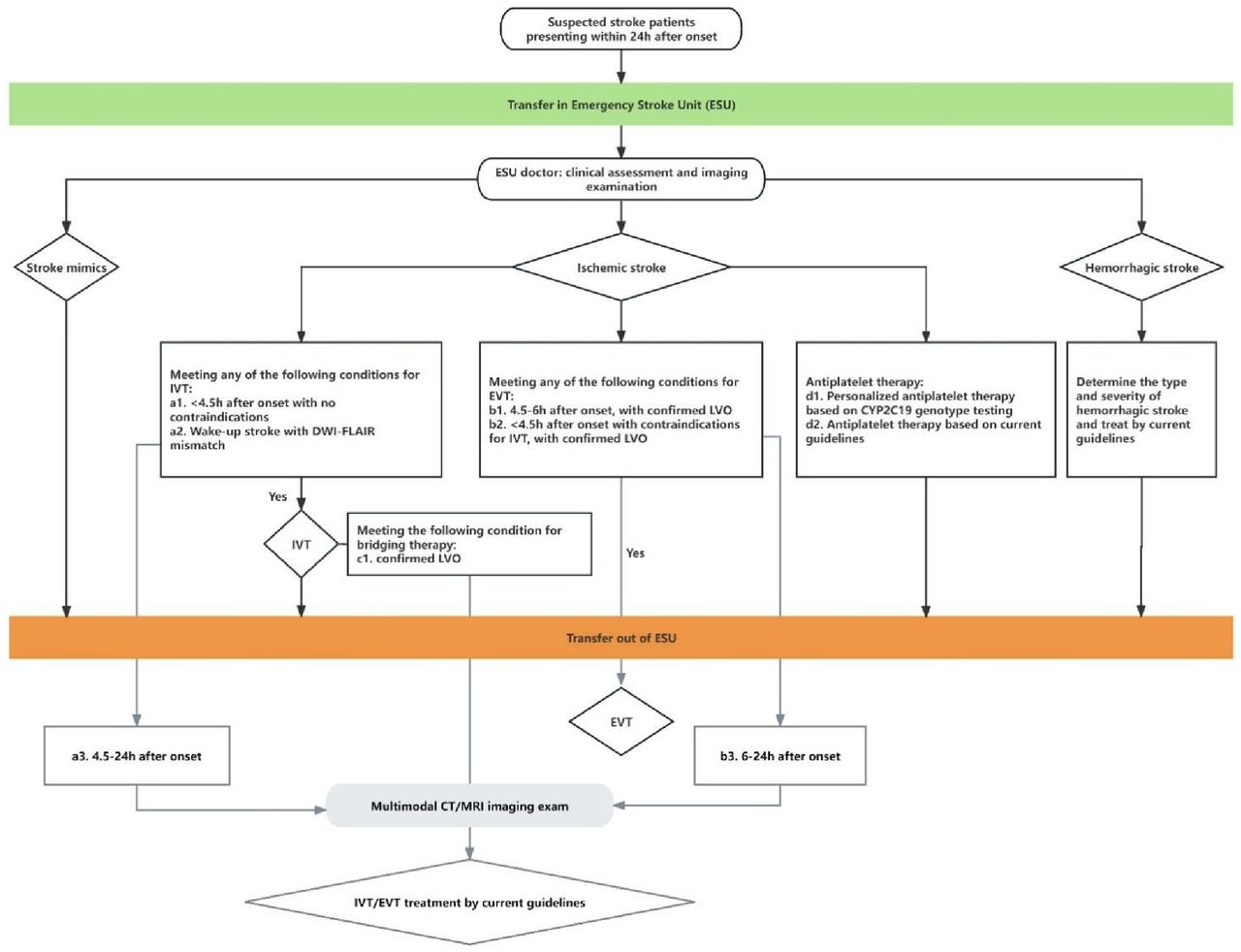
The one-stop ESU-based emergency stroke triage and treatment workflow is shown in figure 3. After initial triage on arrival at the hospital, patients with suspected stroke will be directed immediately to the ESU. Then an ESU doctor should immediately take the medical history, perform physical examination, complete imaging examinations, determine the type of stroke (haemorrhagic/ischaemic stroke) and eligibility for acute reperfusion treatment, and obtain informed consent accordingly. Patients with AIS of different conditions as below should receive IVT±endovascular thrombectomy (EVT) as soon as possible, according to the guidelines. Patients who have completed assessment or treatment in the ESU should be transferred to the stroke unit or (neuro) intensive care unit for further treatment.

{kind=link}
{kind=link}
{kind=link}
One-stop ESU-based emergency stroke triage and treatment workflow. DWI, diffusion-weighted imaging; EVT, endovascular thrombectomy; FLAIR, fluid-attenuated inversion recovery; IVT, intravenous thrombolysis; LVO, large vessel occlusion.
Patients with AIS within 4.5 hours of onset: IVT should be administered, and those with an LVO should undergo EVT.
Patients with AIS within 4.5–6 hours of onset: those with an LVO should undergo EVT.
Patients with AIS patients with unknown onset time (eg, wake-up stroke): IVT can be administered if there is a DWI/FLAIR mismatch.
Patients with AIS patients within 6 hours of onset: EVT should be performed, if there is an LVO confirmed with multimodal CT/MRI examinations.
Patients with AIS within 4.5–24 hours of onset: IVT can be administered based on findings from multimodal CT/MRI examinations if the patient can not receive EVT.
Quality control indicators
The proportion of patients completing imaging examinations at ESU within 10 min of hospital arrival, among patients with suspected stroke presenting to the hospital within 4.5 hours of onset who are directed to the ESU, within a certain period of time (eg, 1 month).
The proportion of patients with door-to-needle time <20 minutes at ESU, among all patients with AIS receiving IVT within a certain period of time (eg, 1 month).
The proportion of patients receiving IVT within 4.5 hours of onset at ESU, among all patients with AIS presenting to the hospital within 4.5 hours of onset, within a certain period of time (eg, 1 month).
Summary
ESU can provide efficient and cohesive service to patients with AIS. It will facilitate the guideline-driven standardised rapid stroke work-up and IVT treatment of patients with AIS at any emergency room that can meet the requirement. This will further enhance the quality of acute reperfusion treatment for patients with AIS in China, and achieve the goal of reaching the rate of IVT to 80% and EVT rate to 30% for eligible patients with AIS by 2030, as advocated in the ‘Healthy China Action Plan (2023–2030)’.12 This guideline will facilitate the integration and optimisation of regional medical resources, and organise a more efficient emergency stroke care system in China.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
JJ, XX and XL contributed equally.
Collaborators Xueli Cai, Department of Neurology, Lishui Central Hospital (the Fifth Hospital Affiliated to Wenzhou Medical University/Lishui Hospital of Zhejiang University), Zhejiang, China; Liguo Chang, Department of Neurology, The third People's Hospital of Liaocheng, Shandong, China; Jianhuang Chen, Department of Neurology, Liuyang Jili Hospital, Changsha, Hunan, China; David Wang, Department of Neurology, University of Illinois College of Medicine at Peoria, Peoria, IL, USA; Qiang Dong, Department of Neurology, Huashan Hospital, Fudan University, Shanghai, China; Wanliang Du, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Wen Gao, Department of Cardiology, Bayannur City Hospital, Inner Mongolia, China; Yangtai Guan, Department of Neurology, Punan Branch of Renji Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China; Xinsheng Han, Department of Neurology, Kaifeng Central Hospital, Henan, China; Qiuhong Ji, Department of Neurology, Affiliated Hospital of Nantong University, Jiangsu, China; Jing Jing, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Xinyi Leng, Department of Medicine and Therapeutics, the Chinese University of Hong Kong, Hong Kong, China; Thomas W Leung, Department of Medicine and Therapeutics, the Chinese University of Hong Kong, Hong Kong, China; Hao Li, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Juntao Li, Department of Neurology, HanDan Central Hospital, Hebei, China; Tong Li, Department of Neurology, the Second Nanning People's Hospital, Nanning, Guangxi, China; Zixiao Li, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Jianmin Liu, Department of Neurology, The First Affiliated Hospital of Naval Military Medical University, Shanghai, China; Tao Liu, Beijing Advanced Innovation Center for Biomedical Engineering, School of Biological Science and Medical Engineering, Beihang University, Beijing, China; Yaou Liu, Department of Radiology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Guozhi Lu, Department of Neurology, Zhongmeng Hospital of Hexigten Banner, Chifeng City, China; Bin Mei, Department of Neurology, Zhongnan Hospital of Wuhan University, Hubei, China; Xia Meng, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Zhen Mi, Department of Neurology, People's Hospital of Lhasa, Lhasa, China; Zhongrong Miao, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Zhongyong Peng, Department of Neurology, The Second People's Hospital of Guiyang, Guizhou, China; Xuchen Qi, Department of Neurosurgery, Shaoxing People's Hospital (Shaoxing Hospital, Zhejiang University School of Medicine), Shaoxing, China; Zeguang Ren, Department of Neurosurgery, The Affiliated Hospital of Guizhou Medical University, Guiyang, Guizhou, China; Xueqin Song, Department of Neurology, Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, China; Zefeng Tan, Department of Neurology, The First People's Hospital of Foshan, Guangdong, China; Lusha Tong, Department of Neurology, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Baojun Wang, Department of Neurology, Baotou City Central Hospital, Inner Mongolia, China; Yihuai Wang, Ray Plus Medical Technology Co., Ltd., Foshan, Guangdong, China; Jialing Wu, Department of Neurology, Tianjin Huanhu Hospital, Tianjin, China; Yiping Wu, Department of Neurology, HanDan Central Hospital, Hebei, China; Xuewei Xie, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Wenli Xing, Department of Cerebrovascular Disease, Suining Central Hospital, Suining, Sichuan, China; Anding Xu, Department of Neurology, The First Affiliated Hospital of Jinan University, Guangdong, China; Chenghua Xu, Department of Neurology, Taizhou First People's Hospital, Zhejiang, China; Qi Yang, Department of Radiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, China; Xiaoxi Yao, Department of Neurology, The First People's Hospital of Chenzhou, Hunan, China; Tingyu Yi, Department of Neurology, Zhangzhou Affiliated Hospital of Fujian Medical University, Fujian, China; Jinglin Yuan, Department of Neurology, Beijing Daxing District People’s Hospital, Beijing, China; Yonghong Zhang, Department of Epidemiology, School of Public Health, Suzhou Medical College of Soochow University, Suzhou, China; Jing Zhao, Department of Neurology, Minhang Hospital, Fudan University, Shanghai, China; Xingquan Zhao, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; Chongke Zhong, Department of Epidemiology, School of Public Health, Suzhou Medical College of Soochow University, Suzhou, China; Li Zhou, Department of Neurology, Weifang People's Hospital, Shandong, China; Zhiming Zhou, Department of Neurology, Yijishan Hospital of Wannan Medical College, Wuhu, China.
Contributors YW proposed the concept of Emergency Stroke Unit and outline of this guideline. JJ, XX and XL drafted the article. DW and YW revised the article. All members of the Writing Committee of Emergency Stroke Unit Alliance, Chinese Stroke Association approved the final version of the guideline.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.