Digital subtraction angiographic characteristics of progression of moyamoya disease 6 months prior to surgical revascularisation
- Peicong Ge,
- Qian Zhang,
- Xun Ye,
- Xingju Liu,
- Xiaofeng Deng,
- Jia Wang,
- Rong Wang,
- Yan Zhang,
- Dong Zhang,
- Ji Zong Zhao
- Correspondence to Professor Ji Zong Zhao; zhaojz205{at}163.com
- Received 12 December 2019
- Revised 29 January 2020
- Accepted 31 January 2020
Abstract
Background Evidence on the natural angiographic course of moyamoya disease (MMD) is lacking. It takes about 6 months for waiting for revascularisation surgery. The issue of when to perform subtraction angiography (DSA) for follow-up remains unclear. We investigated the natural course of MMD by DSA and attempted to determine the best interval to perform the follow-up DSA.
Methods This is a single-centre cohort study of Chinese MMD inpatients treated from 1 January 2015 to 31 August 2019. Their angiographic findings were evaluated on Suzuki stage and collateral circulation between two follow-ups of the same hemisphere.
Results A total of 110 patients who met the criteria were enrolled in this study. After a median 6 months follow-up, five patients (4.5%) had progression, four females and one male. Time interval of progression ranged from 4 to 137 months with a mean of 61.4 months. Of five patients with progression, four had unilateral lesion (two ipsilateral and two contralateral) and one had bilateral lesions. Collateral circulation was changed in three of five patients.
Conclusions The angiographic evidence of progression in MMD was rare in the short-term follow-up, and most patients with progression had initial unilateral involvement. DSA re-examination may be not needed in patients with bilateral MMD, but needed in unilateral MMD.
- stroke
- catheter
- history
Introduction
Moyamoya disease (MMD) is a chronic cerebrovascular occlusive disorder characterised by progressive occlusion of the internal carotid arteries and/or their main branches with compensatory of development of a basal collateral network.1 MMD is an uncommon cerebrovascular disease, but it is the leading cause of stroke in children and young adults among Japan, Korea and China.2 3 According to the presentation of MMD, there are two main phenotypes of MMD in the Eastern countries: ischaemic and haemorrhagic type.4
The current goals of managing MMD are to improve neurological/neurocognitive function and prevent ischaemic stroke.3 5 In spite of some controversy, surgical revascularisation is currently considered as the most effective treatment for MMD. Beijing Tiantan Hospital is one of the major referral centres for MMD in China. Because of the limited medical resources and large number of patients with MMD, a 6-month waiting is needed before the revascularisation surgery can be scheduled. The dilemma, therefore, is when will be appropriate to perform a digital subtraction angiography (DSA) during this period, of if DSA re-examination is actually needed. Therefore, understanding the progression of MMD is crucial. Recently, clinical course of haemorrhagic MMD has been well documented,6–9 However, the use of DSA to follow the progression of MMD has rarely been reported. We conducted this retrospective study to examine the 6-month progression of MMD by DSA.
Methods
This is a single-centre retrospective study. Data on Chinese MMD inpatients treated at Beijing Tiantan Hospital, Capital Medical University from 1 January 2015 to 31 August 2019 was reviewed. Patients met the following criteria was included in this study: (1) diagnosis of MMD by DSA according to the Japanese guidelines published in 201210; (2) received at least two DSA examinations before the surgical revascularisation; (3) received no craniotomy (including decompressive craniectomy, ipsilateral and contralateral hemisphere surgical revascularisation) and (4) patients were not in the acute stage of stroke. Patients with moyamoya syndromes (moyamoya phenomenon caused by conditions such as meningitis, neurofibromatosis and Down’s syndrome) were excluded.11
Information on patient sex, age, risk factors, such as hypertension, smoking, diabetes, alcohol use, hyperlipidaemia and thyroid disease, was tabulated. The clinical course was followed by clinic visits and telephone interviews. Stroke was defined as a new neurological deficit that persisted for more than 24 hours and associated with a new infarct or haemorrhage on MRI or CT imaging. Radiological data were evaluated blindly by two neurosurgeons and one radiologist. Suzuki stage, collateral circulation and aneurysm were documented. Discrepancies on the radiological findings were discussed before a final decision was made. Collateral circulation was evaluated by the following method.12 On lateral views of vertebrobasilar artery angiograms, the leptomeningeal collateral networks from the posterior cerebral artery (PCA) territory to the anterior cerebral artery (ACA) territory:13 (1) one point: blood supply to the cortical border zone between the ACA and PCA territory; (2) two points: blood supply over the central sulcus via the posterior pericallosal artery. On anteroposterior view of vertebrobasilar artery angiograms, the leptomeningeal collateral networks from the PCA territory to the middle cerebral artery (MCA) territory: (1) one point: the anastomoses of the anterior temporal branches of PCA and MCA or the parieto-occipital PCA anastomoses to MCA; (2)two points: blood supply extended into the Sylvian fissure and (3)three points: blood supply extended into the occlusion within the M1 or proximal M2 segments.
Statistical analyses
All analyses was carried out by using the IBM SPSS statistical software (V.23.0). Ordinal categorical variables were compared with paired Wilcoxon rank-sum test. Cumulative stroke risk was performed using Kaplan-Meier methods using a log-rank test. Differences with a p value of 0.05 or less were defined as statistically significance.
Results
Patient characteristics
A total of 110 patients (220 hemispheres) were enrolled in this study. The female to male ratio was 1.0:1.1, and the median age at the diagnosis was 39. Of the 110 patients, 2 (2.7%) had a familial history, 37 (33.6%) had a history of hypertension, 18 (16.4%) had a history of smoking, 12 (10.9%) had diabetes, 12 (9.1%) had a history of alcohol use, 6 (5.5%) had hyperlipidaemia and 5 (4.5%) had thyroid disease (table 1).
Patientcharacteristics
The initial clinical manifestations were divided into two groups, ischaemic (66 patients) or haemorrhagic (44 patients), respectively. Of the 66 patients in the ischaemic group, 44 (66.7%) presented with infarction, and 22 (33.3%) had a transient ischaemic attack. Of 44 patients in the haemorrhagic group, 19 (43.2%) had an intraventricular haemorrhage (IVH), 11 (25.0%) had intracranial haemorrhage (ICH) with IVH, 9 (20.5%) had only ICH and 5 (11.3%) had subarachnoid haemorrhage.
The angiographic course of MMD
Of 110 patients, 21 (19.1%) had unilateral lesion and 89 (80.9%) had bilateral lesions. Of 21 patients with an unilateral lesion, 12 had right-sided involvement and 9 left-sided involvement. The distribution of the initial Suzuki stage was as follows: stage 0, n=21 (9.5%); stage 1, n=13 (5.9%); stage 2, n=48 (21.8%); stage 3, n=65 (29.5%); stage 4, n=45 (20.5%); stage 5, n=17 (7.7%); stage 6, n=11 (5.0%). The distribution of the initial collateral circulation was as follows: PCA-ACA: 0 point, n=48 (21.8%); 1 point, n=43 (19.5%); 2 points, n=129 (58.6%). PCA-MCA: 0 point, n=42 (19.1%); 1 point, n=40 (18.2%); 2 points, n=45 (20.5%); 3 points, n=68 (30.9%); 4 points, n=25 (11.4%). And eight aneurysms were observed in eight hemispheres (table 2).
Radiologic profiles of 220 hemispheres
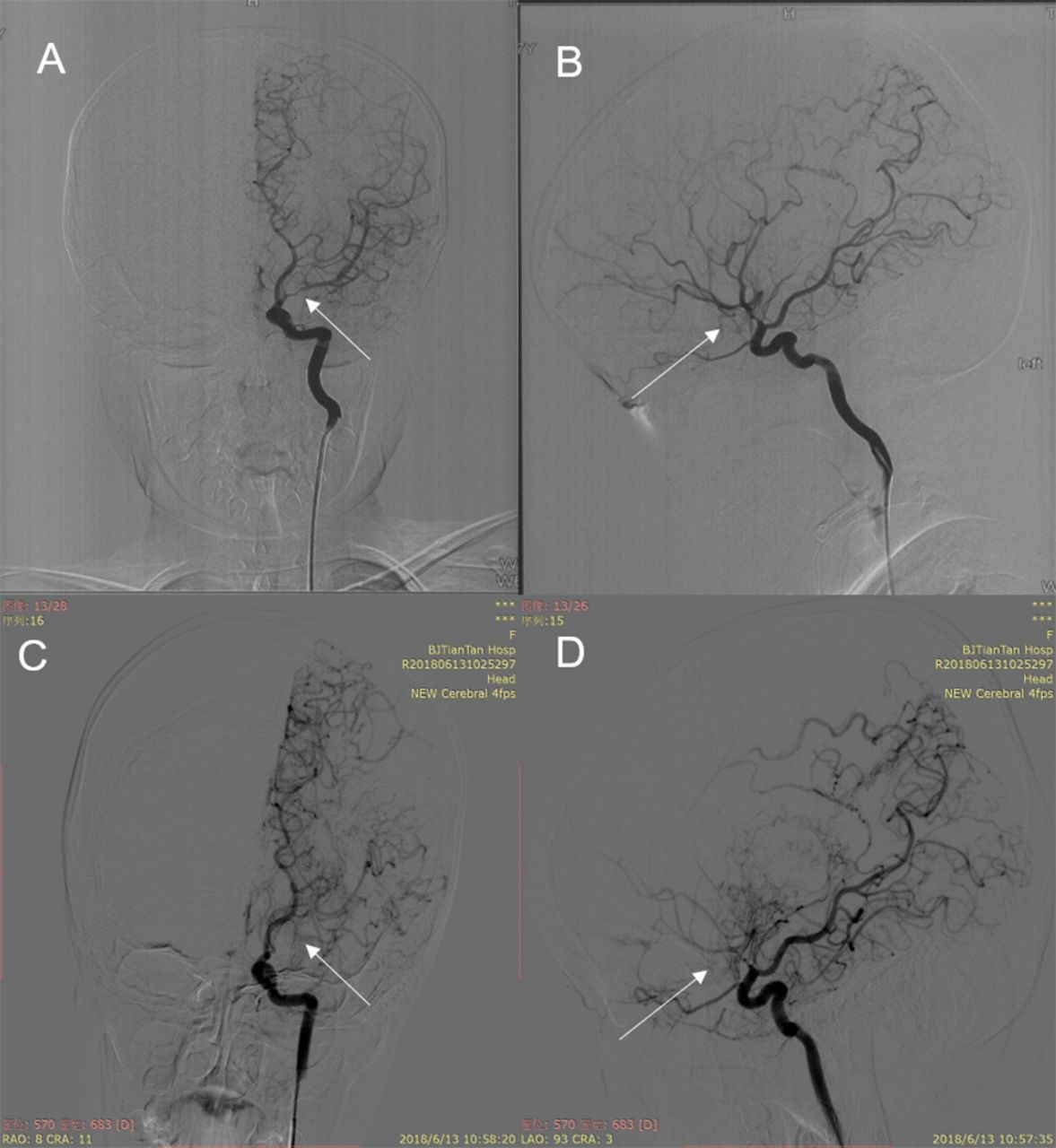
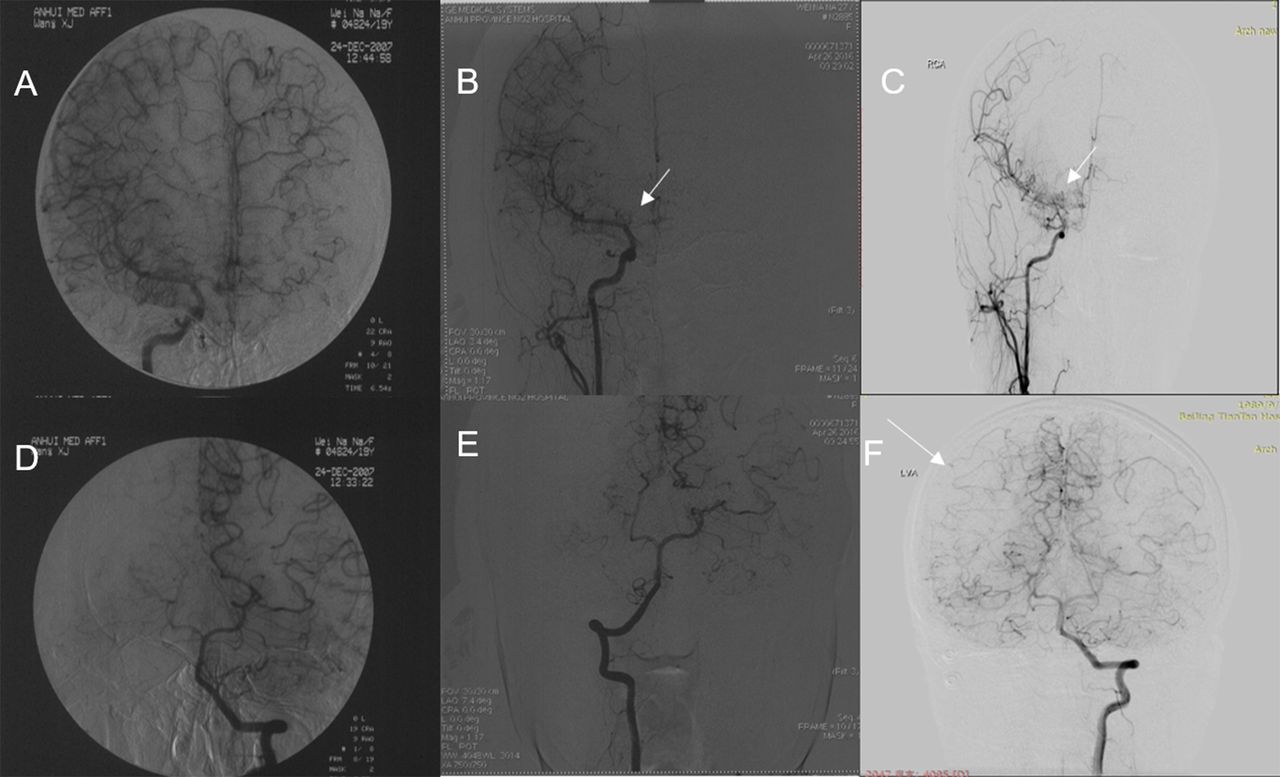
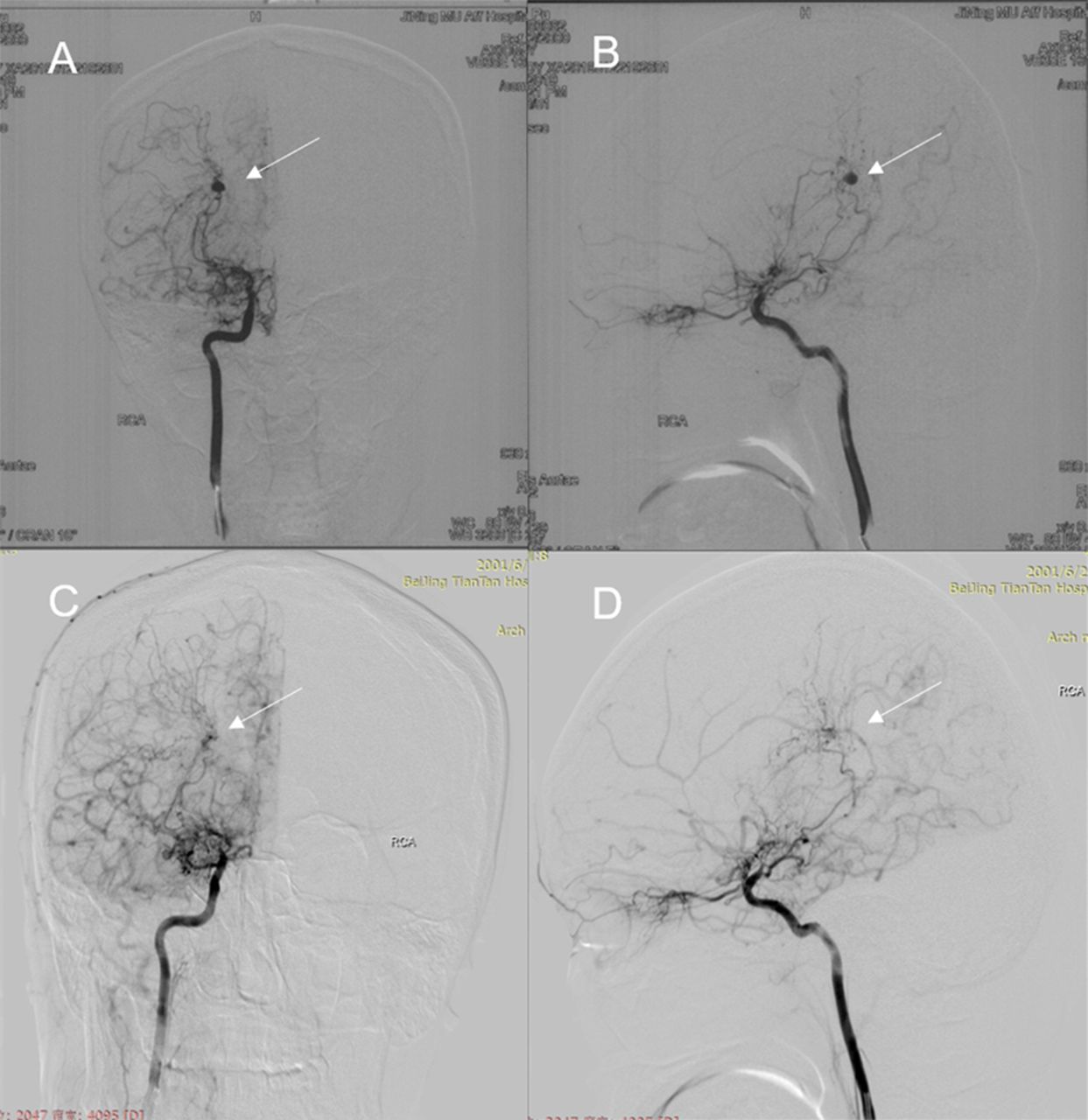
After a median 6 months follow-up, of these 110 patients, progression was identified only in five patients (4.5%). Four patients were female (table 3). Time interval of progression ranged from 4 to 137 months. Of five patients with progression, four had unilateral lesion and one bilateral (figure 1). Of four patients with unilateral involvement, two had contralateral progression (figure 2), and the other two ipsilateral. Collateral circulation was changed with progression of disease, three of five patients changed collateral circulation with progression of disease. And two anterior choroidal artery aneurysms disappeared in the follow-up DSA (figure 3).
Summary of five patients with progression of MMD

(A) Anteroposterior view of internal carotid in the initial DSA. (B) Lateral view of internal carotid in the initial DSA. (C) Progression in anteroposterior view of internal carotid in the second DSA. (D) Progression in lateral view of internal carotid in the second DSA. DSA, digital subtraction angiography.

(A) Anteroposterior view of internal carotid in the initial DSA. (B) Progress in anteroposterior view of internal carotid in the second DSA. (C) Progression in anteroposterior view of internal carotid in the third DSA. (D) Anteroposterior view of vertebrobasilar artery in the initial DSA. (E) Progress in anteroposterior view of vertebrobasilar artery in the second DSA. (F) Progress in anteroposterior view of vertebrobasilar artery in the third DSA. DSA, digital subtraction angiography.

(A) Anteroposterior view of internal carotid in the initial DSA. (B) Lateral view of internal carotid in the initial DSA. (C) Anteroposterior view of internal carotid in the second DSA. (D) Lateral view of internal carotid in the second DSA. DSA, digital subtraction angiography.
Natural clinical course of MMD
There were a total of 38 new events (16 infarctions and 22 haemorrhages) in 34 patients (table 4). Four patients had two strokes. In the ischaemic group, the strokes occurred in 18 of 66 patients (27.3%); In the haemorrhagic group, the strokes occurred in 16 of 44 patients (36.4%). Stroke events occurred more frequently in the haemorrhagic group than ischaemic group (36.4% vs 27.3%). However, there was no statistically significant difference in the Kaplan-Meier curve of stroke free between ischaemic and haemorrhagic types of MMD (figure 4A). Among 18 patients with recurrent strokes in the ischaemic group, there were 14 ischaemic and 5 haemorrhagic strokes. Among 16 patients with recurrent stroke in the haemorrhagic group, there were 2 ischaemic and 17 haemorrhagic strokes. The incidence of haemorrhagic strokes in the haemorrhagic group was higher than that in the ischaemic type group, and the incidence of ischaemic stroke in the ischaemic group was higher than that in the haemorrhagic type group. In patients with progression, the strokes occurred in two of five patients (40%). In patients without progression, the strokes occurred in 32 of 105 patients (30.5%). There was no statistically significant difference in stroke risks between two groups (figure 4B).
Stroke events in each group

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The Kaplan-Meier estimate of follow-up stroke event in each group. (A) Kaplan-Meier cumulative hazard curve for stroke recurrence comparing ischaemic type and haemorrhagic-type group. (B) Kaplan-Meier cumulative hazard curve for stroke recurrence comparing patients with progression and patients without progression.
Discussion
This study investigated the angiographic course of MMD with a relatively large number of patients. We gained valuable information about the angiographic features of MMD. Angiographic progression in MMD was rare, only in five patients (4.5%). And most patients (four of five patients) with progression had initial unilateral involvement, with one bilateral. Furthermore, collateral circulation was changed with progression of disease.
Natural clinical course of MMD has been well documented, especially in haemorrhagic type of MMD.6–9 14–17 Kobayashi et al conducted a study of natural history of 42 patients with haemorrhagic MMD and found that the annual rebleeding rate was 7.09%/person/year, and the hemisphere and type of haemorrhage may change.7 Morioka et al performed long-term observation of 36 haemorrhagic patients with MMD and found that rebleeding was the most important factor in unsatisfactory outcomes, and rebleeding was age related (46–55 years).14 Cho et al performed a natural clinical course of haemodynamically stable adult MMD and found that the annual stroke rate was 4.3% per person per year, and the stroke type tended to correspond to their initial presentation.8 In our study, we also found that the incidence of haemorrhagic strokes in the haemorrhagic group was higher than that in the ischaemic group, and the incidence of ischaemic stroke in the ischaemic group was higher than that in the haemorrhagic group. Recently, Kim et al found that the presence of IVH was a significant risk factor for recurrent haemorrhage.9 Takahashi et al found that patients with posterior-type haemorrhage were at higher risk of rebleeding.18 And our previous study had found that the annual incidence of stroke was 4.5% per person per year, smoking was a risk factor for rebleeding, and hypertension was associated with increased mortality.6
Paucity of study monitored the natural angiographic course of MMD by using DSA.19 There were only a few studies about unilateral MMD.20–22 Park et al performed a study of 34 paediatric patients with unilateral MMD by using MR angiography and found that 20 patients (58.8%) progressed to bilateral disease.19 Kelly et al found that contralateral progression in the adult form MMD occurred more commonly than previously reported.22 Our previous study showed that 16.5% of adult patients with MMD had contralateral progression.22 23 Takahashi et al conducted long-term follow-up angiography of 11 patients with MMD and found that the progression of angiographical stages was observed in 95% of sides.19 In this study, we found that angiographic progression in MMD was rare in the short-term follow-up, which was identified only in five patients (4.5%). And most patients (four of five patients) with progression had initial unilateral involvement, and only one had initial bilateral lesions. These findings reminded us that a second DSA examination may be not necessary for patients with initial bilateral lesions in the short term, brain CT angiography or MR angiography may be sufficient. However, for patients with initial unilateral MMD, careful and long-term follow-up would be essential to evaluate the progression of disease. Interestingly, we found that three of five patients changed collateral circulation with progression of disease, which indicated that collateral circulation can change with the progression of disease. Collateral circulation may influence the therapeutic prognosis.12
This study has some limitations. First, this study was a non-randomised, retrospective and single-centre study, so selection bias could exist. Second, the time from the initial DSA to second DSA was not long enough to evaluate the natural angiographic course of MMD, however, this situation may be more natural in the clinical setting. Third, follow-up DSA was not routinely performed for most of patients, only a few patients received a second DSA, selection bias may exist.
Conclusions
The angiographic evidence of progression in MMD was rare in the short-term follow-up, and most patients with progression had initial unilateral involvement. DSA re-examination may not be needed for patients with bilateral MMDs, but needed for unilateral MMDs.
Acknowledgments
We thank Lebao Yu, Yahui Zhao, Jiaxi Li and Chengjun Wang for their contributions to the data collection.
Footnotes
Contributors PG, QZ and JZZ: conception and design. PG, XY, XL and XD: acquisition of data. PG, JW and QZ: analysis and interpretation of data. PG: drafting the article. RW, YZ and DZ: technical supports and surgery. All authors critically revising the article and approved the final version of the manuscript. JZZ and QZ: study supervision.
Funding This study was supported by the National Key Technology Research and Development Programme of the Ministry of Science and Technology of China (grants 2006BAI01A13 and 2015BAI12B04), Beijing Municipal Organisation Department Talents Project (grant 2015000021469 G219), Beijing Municipal ST Commission (grant D161100003816005) and National Natural Science Foundation of China (grant 81701137).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The hospital institutional review board approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The datasets supporting the conclusions of this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.